Вам также может понравиться
- Intelect TENS Pocket Analog With TimerДокумент1 страницаIntelect TENS Pocket Analog With TimerPyrectic WilliamsОценок пока нет
- CH 11 Osteoarthritis - Primer On The Rheumatic Diseases 13th EdДокумент17 страницCH 11 Osteoarthritis - Primer On The Rheumatic Diseases 13th EdPyrectic WilliamsОценок пока нет
- Consumerism The Role of Patient ExperienceДокумент9 страницConsumerism The Role of Patient ExperiencePyrectic WilliamsОценок пока нет
- Cervical Traction 2Документ13 страницCervical Traction 2Dw Ipha Ma HaОценок пока нет
- CH 6-2 The Arthritic Knee - Clinical Orthopaedic RehabilitationДокумент17 страницCH 6-2 The Arthritic Knee - Clinical Orthopaedic RehabilitationPyrectic WilliamsОценок пока нет
- CH 41 LBP - Braddom's Physical Medicine & RehabilitationДокумент46 страницCH 41 LBP - Braddom's Physical Medicine & RehabilitationPyrectic WilliamsОценок пока нет
- Do Medical Outpatients Want 'Out of Hours' ClinicsДокумент4 страницыDo Medical Outpatients Want 'Out of Hours' ClinicsPyrectic WilliamsОценок пока нет
- Exercise Physiology: Dr. Patrick W. SPKFRДокумент89 страницExercise Physiology: Dr. Patrick W. SPKFRPyrectic WilliamsОценок пока нет
- Homeostasis and Feedback Loops AjarДокумент34 страницыHomeostasis and Feedback Loops AjarPyrectic WilliamsОценок пока нет
- Fisiologi Sel Dan JaringanДокумент39 страницFisiologi Sel Dan JaringanPyrectic Williams100% (1)
- Chronic Low Back PainДокумент14 страницChronic Low Back PainranggadrОценок пока нет
- Fisio OlahragaДокумент65 страницFisio OlahragaPyrectic WilliamsОценок пока нет
- Paediatric Cardiac Rehabilitation in Congenital Heart DiseaseДокумент11 страницPaediatric Cardiac Rehabilitation in Congenital Heart DiseasePyrectic WilliamsОценок пока нет
- Venous Thromboembolism in Acute Spinal Cord Injury PatientsДокумент11 страницVenous Thromboembolism in Acute Spinal Cord Injury PatientsPyrectic WilliamsОценок пока нет
- The RelationshipДокумент36 страницThe RelationshipPyrectic WilliamsОценок пока нет
- Comprehensive Mangement of ObesityДокумент21 страницаComprehensive Mangement of ObesityPyrectic WilliamsОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Practice Worksheet Class XiiДокумент7 страницPractice Worksheet Class XiiManjusha NayakОценок пока нет
- Prevalence of Seizure and Prescribing Patterns of Aed in Patients With NeuroДокумент120 страницPrevalence of Seizure and Prescribing Patterns of Aed in Patients With NeurosnigdhaОценок пока нет
- Barium Swallow Meal Follow-Through MealДокумент2 страницыBarium Swallow Meal Follow-Through MealPervez Ahmad AhmadОценок пока нет
- Epidemiology of Infectious DiseasesДокумент69 страницEpidemiology of Infectious Diseasesmus zaharaОценок пока нет
- Chapter 42 - Upper Urinary Tract: TraumaДокумент2 страницыChapter 42 - Upper Urinary Tract: TraumaSyahdat NurkholiqОценок пока нет
- SOAP NOTE SinusitisДокумент3 страницыSOAP NOTE SinusitisMaria Ines Ortiz0% (1)
- Sarcomas of The Head and Neck: Dr. DarwitoДокумент60 страницSarcomas of The Head and Neck: Dr. DarwitolaurasheerОценок пока нет
- OTC and PRESCRIPTION DRUGS Ppt. (TANTICO)Документ10 страницOTC and PRESCRIPTION DRUGS Ppt. (TANTICO)Ladyfair TanticoОценок пока нет
- HSG Maxessential Brochure W ForeignersДокумент18 страницHSG Maxessential Brochure W Foreignersswapnil.pandeyОценок пока нет
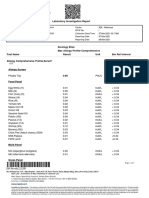
- Laboratory Investigation ReportДокумент7 страницLaboratory Investigation ReportAmarjeetОценок пока нет
- Acetaminophen (Paracetamol, Tylenol, Tempra, Panadol)Документ3 страницыAcetaminophen (Paracetamol, Tylenol, Tempra, Panadol)Jocelyn Rivera0% (1)
- Approach To Nursing Assessment 1Документ5 страницApproach To Nursing Assessment 1Taiye OkondoОценок пока нет
- Jurnal PDEДокумент9 страницJurnal PDEKyefasОценок пока нет
- Hemorrhagic Disease of The NewbornДокумент3 страницыHemorrhagic Disease of The NewbornDevi SuryandariОценок пока нет
- New Techniques in Chelonian Shell RepairДокумент8 страницNew Techniques in Chelonian Shell RepairChecko LatteОценок пока нет
- Mock Congress Bill Research EssayДокумент9 страницMock Congress Bill Research Essayapi-302890064Оценок пока нет
- Blaylock Forced0415 130Документ13 страницBlaylock Forced0415 130RAMO STEF SZEKERESОценок пока нет
- Paper 1Документ11 страницPaper 1api-499574410Оценок пока нет
- Question 1Документ87 страницQuestion 1hemihemaОценок пока нет
- Case Study On LBWДокумент43 страницыCase Study On LBWOmotosho Alex50% (2)
- How To Manage Cortisol Levels With Maca RootДокумент19 страницHow To Manage Cortisol Levels With Maca RootCalvin McDuffieОценок пока нет
- Tabel Severitas BPJS Tindakan JantungДокумент9 страницTabel Severitas BPJS Tindakan JantungTeduh ParamadinaОценок пока нет
- Agger NasiДокумент3 страницыAgger NasiDr Saikat SahaОценок пока нет
- General Examination For CVSДокумент29 страницGeneral Examination For CVSstudymedic100% (1)
- CONJUNCTIVITIS or Pink Eye, Emotional and Spiritual MeaningДокумент1 страницаCONJUNCTIVITIS or Pink Eye, Emotional and Spiritual MeaningSarah g.Оценок пока нет
- Unik Group-1Документ10 страницUnik Group-1Different PointОценок пока нет
- Musculoskeletal RehabilitationДокумент25 страницMusculoskeletal RehabilitationNadia Ayu TiarasariОценок пока нет
- FP Form ItrДокумент2 страницыFP Form ItrAlibasher Macalnas100% (1)
- Refractive Surgery Standards Dec 2004Документ7 страницRefractive Surgery Standards Dec 2004dr_jrcОценок пока нет
- Limpeza PedeДокумент9 страницLimpeza Pedemarisa araujoОценок пока нет