Вам также может понравиться
- Chennai CMDA Master Plan 2026 Volume 3 Sectorial BackgroundДокумент270 страницChennai CMDA Master Plan 2026 Volume 3 Sectorial BackgroundMalathi Kathirvel100% (1)
- Notes in Judicial AffidavitДокумент11 страницNotes in Judicial AffidavitguibonganОценок пока нет
- Jsa - Cable TerminationДокумент4 страницыJsa - Cable TerminationSantos Rex73% (15)
- Natural Gas ENgineering - Jann Rune Ursin PDFДокумент361 страницаNatural Gas ENgineering - Jann Rune Ursin PDFDanitza Pamela Quisbert100% (1)
- Oral Health-Related Quality of Life, Sense of Coherence and Dental Anxiety: An Epidemiological Cross-Sectional Study of Middle-Aged WomenДокумент6 страницOral Health-Related Quality of Life, Sense of Coherence and Dental Anxiety: An Epidemiological Cross-Sectional Study of Middle-Aged WomenAlexandru Codrin-IonutОценок пока нет
- The Psycho-Social Impact of Malocclusions and Trea PDFДокумент10 страницThe Psycho-Social Impact of Malocclusions and Trea PDFClaypella MaskОценок пока нет
- Comparison of Two Survey Instruments Measuring Quality of Life in Pediatric Dentofacial PatientsДокумент6 страницComparison of Two Survey Instruments Measuring Quality of Life in Pediatric Dentofacial PatientsFrancelia Quiñonez RuvalcabaОценок пока нет
- Oral Health Related Quality of Life ThesisДокумент5 страницOral Health Related Quality of Life Thesisb0sus1hyjaf2100% (2)
- 04 Agou Locker 2011 Psych Well Being OHrQolДокумент9 страниц04 Agou Locker 2011 Psych Well Being OHrQolamalia rieska mauliddyaОценок пока нет
- GeriatriaДокумент6 страницGeriatriaGoku BlackОценок пока нет
- Prpposal Presentation Oct 2011 RevДокумент34 страницыPrpposal Presentation Oct 2011 RevLeilawati SulaimanОценок пока нет
- Quality of Life and Psychosocial Outcomes After Fixed Orthodontic TreatmentДокумент11 страницQuality of Life and Psychosocial Outcomes After Fixed Orthodontic TreatmentAhmad Ulil AlbabОценок пока нет
- JBM - Effect of MalocclusionДокумент10 страницJBM - Effect of MalocclusionAma AmuasiОценок пока нет
- Impact of Orthodontic Treatment On Oral Health-Related Quality of Life in The Slovak Republic: A Cross-Sectional StudyДокумент10 страницImpact of Orthodontic Treatment On Oral Health-Related Quality of Life in The Slovak Republic: A Cross-Sectional StudyKornist BufuОценок пока нет
- Effect of Ageing On Oral Health-Related Quality of Life: Review ArticleДокумент3 страницыEffect of Ageing On Oral Health-Related Quality of Life: Review ArticlejoephinОценок пока нет
- Item-Level Analysis of The Relationship Between Orthodontic Treatment Need and Oral Health - Related Quality of Life in Korean SchoolchildrenДокумент7 страницItem-Level Analysis of The Relationship Between Orthodontic Treatment Need and Oral Health - Related Quality of Life in Korean SchoolchildrenMonojit DuttaОценок пока нет
- Poor Oral HealthДокумент10 страницPoor Oral HealthAwais FaridiОценок пока нет
- Impact of Dental Caries On Preschool Children's Quality of Life: An UpdateДокумент6 страницImpact of Dental Caries On Preschool Children's Quality of Life: An UpdateNgakan OkaОценок пока нет
- Thesis On Oral Health Related Quality of LifeДокумент5 страницThesis On Oral Health Related Quality of Lifeafknawjof100% (2)
- Adj 12774Документ5 страницAdj 12774Irfan HussainОценок пока нет
- Antoun 2015Документ8 страницAntoun 2015yina montoyaОценок пока нет
- 1 s2.0 S0300571216302202 MainДокумент6 страниц1 s2.0 S0300571216302202 MainRaluca ChisciucОценок пока нет
- Articol 2Документ6 страницArticol 2Georgian CalimanОценок пока нет
- Improvement of Patient S Satisfaction and Oral Health-Related Quality of Life by The Implant and Prosthodontic TreatmentДокумент29 страницImprovement of Patient S Satisfaction and Oral Health-Related Quality of Life by The Implant and Prosthodontic TreatmentLouis HutahaeanОценок пока нет
- 10 1111@idj 12576Документ7 страниц10 1111@idj 12576badria bawazirОценок пока нет
- Lifecourse Socioeconomic Position Indicators and Tooth Loss in Korean AdultsДокумент10 страницLifecourse Socioeconomic Position Indicators and Tooth Loss in Korean AdultsStephanyОценок пока нет
- The Role of Dental Pain and Psychosocial Factors On The Relationship Between Dental Caries and Oral Health-Related Quality of Life in ChildrenДокумент10 страницThe Role of Dental Pain and Psychosocial Factors On The Relationship Between Dental Caries and Oral Health-Related Quality of Life in ChildrenTiaraОценок пока нет
- Proposal 2Документ4 страницыProposal 2Yussuf OmarОценок пока нет
- Ecde 18 01269Документ11 страницEcde 18 01269haneenhayazaaОценок пока нет
- JCM 10 00426 v3Документ12 страницJCM 10 00426 v3novia chantikaОценок пока нет
- Kragt 2017Документ7 страницKragt 2017zhrieeОценок пока нет
- Association of Orthodontic Treatment Needs and Oral Health-Related Quality of Life in Young AdultsДокумент6 страницAssociation of Orthodontic Treatment Needs and Oral Health-Related Quality of Life in Young AdultsNaliana LupascuОценок пока нет
- Combining Normative and Psychosocial Perceptions For Assessing Orthodontic Treatment NeedsДокумент10 страницCombining Normative and Psychosocial Perceptions For Assessing Orthodontic Treatment NeedsAndres TandeanОценок пока нет
- Uoi 142 FДокумент9 страницUoi 142 FbkprosthoОценок пока нет
- Capstone PaperДокумент6 страницCapstone Paperapi-708882162Оценок пока нет
- Impact of Systemic Lupus Erythematosus On Oral Health-Related Quality of LifeДокумент7 страницImpact of Systemic Lupus Erythematosus On Oral Health-Related Quality of LifegugicevdzoceОценок пока нет
- Marcela Baraúna Magno - Lucas Alves Jural - Ayla Do Valle Nogueira - Michele Machado Lenzi - Matheus Melo Pithon - Lucianne Cople MaiaДокумент8 страницMarcela Baraúna Magno - Lucas Alves Jural - Ayla Do Valle Nogueira - Michele Machado Lenzi - Matheus Melo Pithon - Lucianne Cople MaiafghdhmdkhОценок пока нет
- Oral HealthДокумент44 страницыOral HealthSaria AbbasОценок пока нет
- Impact of Systemic Lupus Erythematosus On Oral Health-Related Quality of LifeДокумент7 страницImpact of Systemic Lupus Erythematosus On Oral Health-Related Quality of LifeGissellePantojaОценок пока нет
- Psychosocial Impact of Dental Esthetics On Quality of Life in AdolescentsДокумент6 страницPsychosocial Impact of Dental Esthetics On Quality of Life in AdolescentsClaypella MaskОценок пока нет
- Psychosocial Impact of Dental Esthetics On Quality of Life in AdolescentsДокумент6 страницPsychosocial Impact of Dental Esthetics On Quality of Life in Adolescentsamalia rieska mauliddyaОценок пока нет
- Clefts CareimpactДокумент13 страницClefts CareimpactStollery SandboxОценок пока нет
- The Role of Dental Pain and Psychosocial Factors oДокумент11 страницThe Role of Dental Pain and Psychosocial Factors oTiaraОценок пока нет
- Psychosocial Impact of Dental Esthetics On Quality of Life in AdolescentsДокумент7 страницPsychosocial Impact of Dental Esthetics On Quality of Life in Adolescentssumbu pendekОценок пока нет
- Psychosocial Impact of Dental Esthetics On Quality of Life in AdolescentsДокумент7 страницPsychosocial Impact of Dental Esthetics On Quality of Life in Adolescentssumbu pendekОценок пока нет
- Sis Cho 2011Документ8 страницSis Cho 2011朱嘉琪Оценок пока нет
- Oral HygieneДокумент9 страницOral HygieneemeraldwxyzОценок пока нет
- To What Extent Do Oral Disorders Compromise The Quality of LifeДокумент10 страницTo What Extent Do Oral Disorders Compromise The Quality of LifeAhmad Ulil AlbabОценок пока нет
- Dental Aesthetic and Self Confidence Among Filipino AdolescentsДокумент9 страницDental Aesthetic and Self Confidence Among Filipino Adolescentssumbu pendekОценок пока нет
- I0003 3219 91 3 377Документ7 страницI0003 3219 91 3 377aОценок пока нет
- ORTODONCIAchildren 10 00176Документ11 страницORTODONCIAchildren 10 00176EstreLLA ValenciaОценок пока нет
- Accepted Manuscript: 10.1016/j.jebdp.2017.06.007Документ7 страницAccepted Manuscript: 10.1016/j.jebdp.2017.06.007Ayik DarkerThan BlackОценок пока нет
- Result - 8 - 25 - 2023, 12 02 19 AMДокумент25 страницResult - 8 - 25 - 2023, 12 02 19 AMسارة العبيديОценок пока нет
- Association of Oral Healtherelated Quality of Life and Alzheimer Disease: A Systematic ReviewДокумент8 страницAssociation of Oral Healtherelated Quality of Life and Alzheimer Disease: A Systematic ReviewNetra TaleleОценок пока нет
- Development of A Conceptual Model of Oral Health For Malocclusion PatientsДокумент7 страницDevelopment of A Conceptual Model of Oral Health For Malocclusion PatientsSelvia MagdalenaОценок пока нет
- The Association Between Depression and Anxiety and Use of Oral Health Services and Tooth LossДокумент12 страницThe Association Between Depression and Anxiety and Use of Oral Health Services and Tooth LossAhmad Ulil AlbabОценок пока нет
- Dental Caries Experience and Oral Health Related Quality of Life in Working AdultsДокумент8 страницDental Caries Experience and Oral Health Related Quality of Life in Working AdultsArida BitanajshaОценок пока нет
- LUPUSДокумент43 страницыLUPUSGabriel SciberrasОценок пока нет
- Ijp 18 5 Mack 9Документ6 страницIjp 18 5 Mack 9kochikaghochiОценок пока нет
- Eating - and Oral Health-Related Quality of Life in Patients Under Fixed Orthodontic TreatmentДокумент10 страницEating - and Oral Health-Related Quality of Life in Patients Under Fixed Orthodontic TreatmentNaliana LupascuОценок пока нет
- Ew RWEREWQERДокумент8 страницEw RWEREWQERJakeCrОценок пока нет
- Your Dental Health Can Save Your Life: Unlocking the Secrets of Oral-Systemic Health: All About DentistryОт EverandYour Dental Health Can Save Your Life: Unlocking the Secrets of Oral-Systemic Health: All About DentistryОценок пока нет
- Sleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementОт EverandSleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementEdmund LiemОценок пока нет
- The Effect of Different Polishing Systems On The SДокумент8 страницThe Effect of Different Polishing Systems On The Samalia rieska mauliddyaОценок пока нет
- Psychosocial Impact of Dental Esthetics On Quality of Life in AdolescentsДокумент6 страницPsychosocial Impact of Dental Esthetics On Quality of Life in Adolescentsamalia rieska mauliddyaОценок пока нет
- Oral Health Impact Profile (OHIP-14) and Its Association With Dental Treatment Needs of Adolescents in A Rural Nigerian CommunityДокумент6 страницOral Health Impact Profile (OHIP-14) and Its Association With Dental Treatment Needs of Adolescents in A Rural Nigerian Communityamalia rieska mauliddyaОценок пока нет
- Self-Perception of Malocclusion Among Nigerian Adolescents Using The Aesthetic Component of The IotnДокумент7 страницSelf-Perception of Malocclusion Among Nigerian Adolescents Using The Aesthetic Component of The Iotnamalia rieska mauliddyaОценок пока нет
- Malocclusion and The Need For Orthodontic Treatment in Pa-Tients With Temporomandibular DysfunctionДокумент7 страницMalocclusion and The Need For Orthodontic Treatment in Pa-Tients With Temporomandibular Dysfunctionamalia rieska mauliddyaОценок пока нет
- Impact of Malocclusion On The Quality of Life of Brazilian Adolescents: A Population-Based StudyДокумент13 страницImpact of Malocclusion On The Quality of Life of Brazilian Adolescents: A Population-Based Studyamalia rieska mauliddyaОценок пока нет
- Dentino Jurnal Kedokteran Gigi: Vol II. No 1. Maret 2017Документ4 страницыDentino Jurnal Kedokteran Gigi: Vol II. No 1. Maret 2017amalia rieska mauliddyaОценок пока нет
- Dentino Jurnal Kedokteran Gigi: Vol II. No 1. Maret 2017Документ4 страницыDentino Jurnal Kedokteran Gigi: Vol II. No 1. Maret 2017amalia rieska mauliddyaОценок пока нет
- Aktivitas Antibakteri Ekstrak Terstandar Akar Sidaguri (S.rhombifolia) TerhadapДокумент5 страницAktivitas Antibakteri Ekstrak Terstandar Akar Sidaguri (S.rhombifolia) Terhadapamalia rieska mauliddyaОценок пока нет
- Dealing With ComplaintsДокумент16 страницDealing With Complaintsamalia rieska mauliddyaОценок пока нет
- Indirect Veneer Treatment of Anterior Maxillary Teeth With Enamel HypoplasiaДокумент5 страницIndirect Veneer Treatment of Anterior Maxillary Teeth With Enamel Hypoplasiaamalia rieska mauliddyaОценок пока нет
- Laporan Tutorial SGD 2 Blok 5 Skenario V: Tutor: Drg. Retno Kusniati SGD 2Документ1 страницаLaporan Tutorial SGD 2 Blok 5 Skenario V: Tutor: Drg. Retno Kusniati SGD 2amalia rieska mauliddyaОценок пока нет
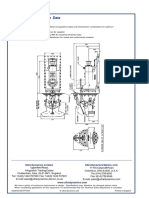
- Ultrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedДокумент2 страницыUltrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedhaujesОценок пока нет
- Pricelist Jan 2023Документ7 страницPricelist Jan 2023Rahmat FadilОценок пока нет
- Puch Moped Horn Wiring Diagram (Chrome Oval Switches)Документ1 страницаPuch Moped Horn Wiring Diagram (Chrome Oval Switches)MopedgalОценок пока нет
- The World Wide WebДокумент22 страницыThe World Wide WebSa JeesОценок пока нет
- Orphanage Project ProposalДокумент3 страницыOrphanage Project ProposaldtimtimanОценок пока нет
- Lesson Worksheet: 6.1A MeanДокумент7 страницLesson Worksheet: 6.1A Meanwaiman fuОценок пока нет
- Uniarch Network Video Recorders User Manual-V1.00Документ99 страницUniarch Network Video Recorders User Manual-V1.00amurjiantoОценок пока нет
- Cold Rolled CoilДокумент23 страницыCold Rolled Coilmametcool100% (1)
- Management of Health Care Services For Ood Victims: The Case of The Shelter at Nakhon Pathom Rajabhat University Central ThailandДокумент7 страницManagement of Health Care Services For Ood Victims: The Case of The Shelter at Nakhon Pathom Rajabhat University Central ThailandAnonymous C06qenyfkmОценок пока нет
- The Cycle of Leadership Through Transformational, Eccles - (Leadership) PDFДокумент16 страницThe Cycle of Leadership Through Transformational, Eccles - (Leadership) PDFEliana LopezОценок пока нет
- Jurnal Stamina: E-ISSN 2655-2515 P-ISSN 2655-1802Документ9 страницJurnal Stamina: E-ISSN 2655-2515 P-ISSN 2655-1802Yogi TioОценок пока нет
- 2.1 Article On Reasonable Compensation Job Aid 4-15-2015Документ3 страницы2.1 Article On Reasonable Compensation Job Aid 4-15-2015Michael GregoryОценок пока нет
- Urban Issues: Rio Case StudyДокумент4 страницыUrban Issues: Rio Case Studyxbox pro hiОценок пока нет
- HP Training Diagnostics 75 Usage and AdministrationДокумент2 страницыHP Training Diagnostics 75 Usage and AdministrationraviskskskОценок пока нет
- Picasso OperatingInstructions Manual 211018 WEBДокумент27 страницPicasso OperatingInstructions Manual 211018 WEBBill McFarlandОценок пока нет
- Brick Bonding AssignmentДокумент4 страницыBrick Bonding AssignmentNija AsifОценок пока нет
- Best of SEO#1 SEO Training & Content Marketing Course 2022Документ2 страницыBest of SEO#1 SEO Training & Content Marketing Course 2022Oscar MascarenoОценок пока нет
- Lust V Animal Logic MSJ OppositionДокумент34 страницыLust V Animal Logic MSJ OppositionTHROnlineОценок пока нет
- Project On Brand Awareness of ICICI Prudential by SajadДокумент99 страницProject On Brand Awareness of ICICI Prudential by SajadSajadul Ashraf71% (7)
- Computing The Maximum Volume Inscribed Ellipsoid of A Polytopic ProjectionДокумент28 страницComputing The Maximum Volume Inscribed Ellipsoid of A Polytopic ProjectiondezevuОценок пока нет
- PF2579EN00EMДокумент2 страницыPF2579EN00EMVinoth KumarОценок пока нет
- Spice Board BBLДокумент24 страницыSpice Board BBLvenkatpficoОценок пока нет
- Daftar Kalibrasi Peralatan MedisДокумент34 страницыDaftar Kalibrasi Peralatan Medisdiklat rssnОценок пока нет
- Tugas-MPSI-P1-P14 - Kelompok 2 - 19.4A.04Документ29 страницTugas-MPSI-P1-P14 - Kelompok 2 - 19.4A.04gilang putraОценок пока нет
- EC1002 Commentary 2022Документ32 страницыEC1002 Commentary 2022Xxx V1TaLОценок пока нет
- MCMCHistoryДокумент18 страницMCMCHistoryAli S.Оценок пока нет