Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Drug ListДокумент30 страницDrug ListKristineОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- AutacoidsДокумент38 страницAutacoidsdrmayangОценок пока нет
- Top 100 OTCДокумент4 страницыTop 100 OTCBen Thomas Moore92% (12)
- Anti-Viral and Anti-Fungal AgentsДокумент212 страницAnti-Viral and Anti-Fungal Agentsmiguel cuevas100% (1)
- Lecture On Subcutaneous MycosesДокумент75 страницLecture On Subcutaneous Mycosesmiguel cuevasОценок пока нет
- Pharmacy & Medical Store Procedure.Документ22 страницыPharmacy & Medical Store Procedure.Google BdОценок пока нет
- Drug Study DMДокумент8 страницDrug Study DMJana Ross Serranilla100% (2)
- Cell Cycle, Apoptosis, and CancerДокумент13 страницCell Cycle, Apoptosis, and Cancermiguel cuevas100% (1)
- Glycogenolysis and GlycogenesisДокумент11 страницGlycogenolysis and Glycogenesismiguel cuevas100% (2)
- Infectious Diseases - BacteriaДокумент9 страницInfectious Diseases - Bacteriamiguel cuevas100% (1)
- 1 Patho5 - Kidney I 2015bДокумент10 страниц1 Patho5 - Kidney I 2015bmiguel cuevasОценок пока нет
- Cholelithiasis Case PresentationДокумент25 страницCholelithiasis Case PresentationMarcos AquinoОценок пока нет
- GastrointestinalДокумент8 страницGastrointestinalFilipino Nurses Central100% (2)
- Git MCQДокумент27 страницGit MCQPadmavathi C100% (8)
- Vitamins Notes PDFДокумент3 страницыVitamins Notes PDFmiguel cuevas100% (1)
- Surgical Pathology Trans No 7. The LIVER DR ROXAS by MCD Recoverd 1Документ14 страницSurgical Pathology Trans No 7. The LIVER DR ROXAS by MCD Recoverd 1miguel cuevasОценок пока нет
- Pathology Final Practical ExaminationДокумент40 страницPathology Final Practical Examinationmiguel cuevasОценок пока нет
- Sex Determination and DifferentiationДокумент3 страницыSex Determination and Differentiationmiguel cuevasОценок пока нет
- Cytogenetics Disorders PDFДокумент7 страницCytogenetics Disorders PDFmiguel cuevasОценок пока нет
- Minerals SummaryДокумент2 страницыMinerals Summarymiguel cuevasОценок пока нет
- Male PhysiologyДокумент2 страницыMale Physiologymiguel cuevasОценок пока нет
- Histo Pracs - Respi and Brain PDFДокумент17 страницHisto Pracs - Respi and Brain PDFmiguel cuevasОценок пока нет
- Diseases of The Peripheral Nervous SystemДокумент8 страницDiseases of The Peripheral Nervous Systemmiguel cuevasОценок пока нет
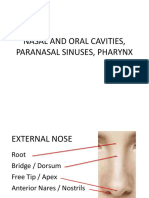
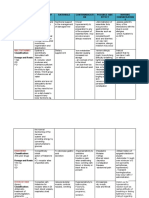
- Nasal and Oral Cavities, Paranasal Sinuses, PharynxДокумент112 страницNasal and Oral Cavities, Paranasal Sinuses, Pharynxmiguel cuevasОценок пока нет
- First Aid: FM 4-25.11 NTRP 4-02.1 AFMAN 44-163 (I)Документ224 страницыFirst Aid: FM 4-25.11 NTRP 4-02.1 AFMAN 44-163 (I)Giuseppe TrovatoОценок пока нет
- Hypolipedemic AgentsДокумент9 страницHypolipedemic Agentsmiguel cuevasОценок пока нет
- RBC - Patho BДокумент129 страницRBC - Patho Bmiguel cuevasОценок пока нет
- Anesthesia - Dr. FirmalinoДокумент14 страницAnesthesia - Dr. Firmalinomiguel cuevasОценок пока нет
- 1.18 MycobacteriumДокумент6 страниц1.18 Mycobacteriummiguel cuevasОценок пока нет
- Female PathologyДокумент16 страницFemale Pathologymiguel cuevasОценок пока нет
- CHF and Diuretics Trans Limpin MissionДокумент12 страницCHF and Diuretics Trans Limpin Missionmiguel cuevasОценок пока нет
- Breast PathologyДокумент27 страницBreast Pathologymiguel cuevasОценок пока нет
- Anti-Psychotic NewestДокумент118 страницAnti-Psychotic Newestmiguel cuevasОценок пока нет
- He Ma To PoiesisДокумент98 страницHe Ma To Poiesismiguel cuevasОценок пока нет
- Microbiology Lecture 8 & 9 - Systemic & Opportunistic Mycoses (Raroromiki Trans)Документ3 страницыMicrobiology Lecture 8 & 9 - Systemic & Opportunistic Mycoses (Raroromiki Trans)miguel cuevasОценок пока нет
- SynapseДокумент45 страницSynapsemiguel cuevasОценок пока нет
- Second Messengers-OLFU-MD 2017Документ66 страницSecond Messengers-OLFU-MD 2017Melissa SalayogОценок пока нет
- Health Risk Assessment and Analysis of Nitrosamine Impurities in Drugs AssДокумент35 страницHealth Risk Assessment and Analysis of Nitrosamine Impurities in Drugs AssYegezu MebratuОценок пока нет
- AntihistaminДокумент46 страницAntihistaminVenerandaОценок пока нет
- Rani Ti DineДокумент2 страницыRani Ti Dinejordan11111111Оценок пока нет
- GerdДокумент19 страницGerdpadma ShriniОценок пока нет
- Jurnal CimetidineДокумент7 страницJurnal CimetidineAidahОценок пока нет
- Final Drug StudyДокумент14 страницFinal Drug StudyStephany Rae MamauagОценок пока нет
- Dosis Ranitidin cw1Документ5 страницDosis Ranitidin cw1Cristine Indria Pieter IIОценок пока нет
- Antacid - Wikipedia, The Free EncyclopediaДокумент4 страницыAntacid - Wikipedia, The Free Encyclopediaumesh123patilОценок пока нет
- Emergency DrugsДокумент10 страницEmergency DrugsnieacatleyaОценок пока нет
- (GPHC) (Autumn) (Closed Book) 2004Документ18 страниц(GPHC) (Autumn) (Closed Book) 2004aliОценок пока нет
- Drugs Acting On Git - En.idДокумент35 страницDrugs Acting On Git - En.idRidho PangestuОценок пока нет
- HSAUpdate HSAStopsSupplyRanitidine8Документ3 страницыHSAUpdate HSAStopsSupplyRanitidine8sabitpurnomoОценок пока нет
- Case Study 1 - Head InjuryДокумент9 страницCase Study 1 - Head InjuryTara McNeillОценок пока нет
- WHO Information Note: BackgroundДокумент4 страницыWHO Information Note: BackgroundRajan MahalingamОценок пока нет
- HEPATITIS A DRUG STUDY FinalДокумент3 страницыHEPATITIS A DRUG STUDY FinalJordz PlaciОценок пока нет
- Upper GI BleedДокумент4 страницыUpper GI BleedAdela SusanОценок пока нет
- Angell Medical Center HandbookДокумент63 страницыAngell Medical Center Handbookjohnabear7Оценок пока нет
- H2 BlockersДокумент2 страницыH2 BlockersteddypolОценок пока нет
- SMS Life Sciences India Limited Financial ReportДокумент7 страницSMS Life Sciences India Limited Financial Reportsaikiran reddyОценок пока нет
- Anti Ulcer AgentsДокумент37 страницAnti Ulcer AgentsKakai Ablanque LopozОценок пока нет
- Big Drugs!!Документ2 145 страницBig Drugs!!Solomon Seth SallforsОценок пока нет
- Drug StudiesДокумент32 страницыDrug StudiesKelly ChanОценок пока нет