Академический Документы
Профессиональный Документы
Культура Документы
Nej Mo A 1214726
Загружено:
Vincent LivandyОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Nej Mo A 1214726
Загружено:
Vincent LivandyАвторское право:
Доступные форматы
The n e w e ng l a n d j o u r na l of m e dic i n e
original article
Probability of Cancer in Pulmonary Nodules
Detected on First Screening CT
Annette McWilliams, M.B., Martin C. Tammemagi, Ph.D., John R. Mayo, M.D.,
Heidi Roberts, M.D., Geoffrey Liu, M.D., Kam Soghrati, M.D.,
Kazuhiro Yasufuku, M.D., Ph.D., Simon Martel, M.D., Francis Laberge, M.D.,
Michel Gingras, M.D., Sukhinder Atkar-Khattra, B.Sc., Christine D. Berg, M.D.,
Ken Evans, M.D., Richard Finley, M.D., John Yee, M.D., John English, M.D.,
Paola Nasute, M.D., John Goffin, M.D., Serge Puksa, M.D., Lori Stewart, M.D.,
Scott Tsai, M.D., Michael R. Johnston, M.D., Daria Manos, M.D., Garth Nicholas, M.D.,
Glenwood D. Goss, M.D., Jean M. Seely, M.D., Kayvan Amjadi, M.D.,
Alain Tremblay, M.D.C.M., Paul Burrowes, M.D., Paul MacEachern, M.D.,
Rick Bhatia, M.D., Ming-Sound Tsao, M.D., and Stephen Lam, M.D.
A BS T R AC T
Background
From Vancouver General Hospital (A.M., Major issues in the implementation of screening for lung cancer by means of low-
J.R.M., K.E., R.F., J.Y., J.E., S.L.) and the dose computed tomography (CT) are the definition of a positive result and the
British Columbia Cancer Agency (A.M.,
S.A.-K., S.L.), Vancouver, BC; the Depart- management of lung nodules detected on the scans. We conducted a population-
ment of Community Health Sciences, based prospective study to determine factors predicting the probability that lung
Brock University, St. Catharines, ON nodules detected on the first screening low-dose CT scans are malignant or will be
(M.C.T.); University Health Network–
Princess Margaret Cancer Centre and To- found to be malignant on follow-up.
ronto General Hospital, Toronto (H.R., Methods
G.L., K.S., K.Y., M.-S.T.); Juravinski Hospi-
tal and Cancer Center, Hamilton, ON
We analyzed data from two cohorts of participants undergoing low-dose CT screen-
(J.G., S.P., L.S., S.T.), Ottawa Hospital ing. The development data set included participants in the Pan-Canadian Early
Cancer Centre, Ottawa (G.N., G.D.G., Detection of Lung Cancer Study (PanCan). The validation data set included partici-
J.M.S., K.A.); Institut Universitaire de
Cardiologie et de Pneumologie de Qué-
pants involved in chemoprevention trials at the British Columbia Cancer Agency
bec, Quebec City, QC (S.M., F.L., M.G.); (BCCA), sponsored by the U.S. National Cancer Institute. The final outcomes of all
Dalhousie University, Halifax, NS (M.R.J., nodules of any size that were detected on baseline low-dose CT scans were tracked.
D.M.); University of Calgary, Calgary, AB
(A.T., P.B., P.M.); and Memorial University
Parsimonious and fuller multivariable logistic-regression models were prepared to
of Newfoundland, St. John’s (R.B.) — all estimate the probability of lung cancer.
in Canada; the National Cancer Institute, Results
National Institutes of Health, Bethesda,
MD (C.D.B.); and Hospital Universitario In the PanCan data set, 1871 persons had 7008 nodules, of which 102 were malig-
Austral, Pilar, Buenos Aires (P.N.). Address nant, and in the BCCA data set, 1090 persons had 5021 nodules, of which 42 were
reprint requests to Dr. Lam at the Depart-
ment of Integrative Oncology, British Co-
malignant. Among persons with nodules, the rates of cancer in the two data sets
lumbia Cancer Agency, 675 W. 10th Ave., were 5.5% and 3.7%, respectively. Predictors of cancer in the model included older
Vancouver, BC V5Z 1L3, Canada. age, female sex, family history of lung cancer, emphysema, larger nodule size, loca-
N Engl J Med 2013;369:910-9. tion of the nodule in the upper lobe, part-solid nodule type, lower nodule count, and
DOI: 10.1056/NEJMoa1214726 spiculation. Our final parsimonious and full models showed excellent discrimination
Copyright © 2013 Massachusetts Medical Society.
and calibration, with areas under the receiver-operating-characteristic curve of more
than 0.90, even for nodules that were 10 mm or smaller in the validation set.
Conclusions
Predictive tools based on patient and nodule characteristics can be used to accurately
estimate the probability that lung nodules detected on baseline screening low-dose
CT scans are malignant. (Funded by the Terry Fox Research Institute and others;
ClinicalTrials.gov number, NCT00751660.)
910 n engl j med 369;10 nejm.org september 5, 2013
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
Probability of Cancer in CT-Detected Pulmonary Nodules
T
he U.S. National Lung Screening ers between 50 and 75 years of age without a
Trial showed that screening with the use history of lung cancer. Eligible participants had a
of low-dose thoracic computed tomogra- 3-year risk of lung cancer of at least 2% as deter-
phy (CT) reduces mortality from lung cancer by mined by a prototype of risk-prediction models in
20%.1 Major clinical issues in the implementa- the Prostate, Lung, Colorectal, and Ovarian Can-
tion of low-dose CT screening at the population cer Screening Trial.7,8 Participants were recruited
level include the definition of a positive screening from September 2008 through December 2010.
result and the appropriate management of lung In the BCCA studies, current and former
nodules detected on a scan. More than 20% of smokers between 50 and 74 years of age without
participants in low-dose CT screening programs a history of lung cancer and with a smoking his-
were found on their first scan to have one or tory of at least 30 pack-years were recruited from
more lung nodules that required further investi- the community from July 2000 through Novem-
gation.1-4 The proportion of invasive diagnostic ber 2010. The study methods have been reported A Quick Take
procedures ranged from 1 to 4%.1,3 The risk of previously.9,10 animation is
available at
major complications was 4.5 complications per NEJM.org
10,000 persons screened, and 25% of the surgical Thoracic CT Scans
procedures in the National Lung Screening Trial In the PanCan, a multidetector-row CT scanner
were performed on nodules that were determined with maximum section collimation of 1.25 mm
to be benign.1 An accurate and practical model and four or more data-acquisition channels was
that can predict the probability that a lung nod- used at each participating site. The CT scans were
ule is malignant and that can be used to guide obtained at 120 kVp, 40 to 50 mA, and a tube-
clinical decision making will reduce costs and rotation time of less than 1 second. Contiguous
the risk of morbidity and mortality in screening images were reconstructed in the transaxial plane
programs. We report the development and vali- at up to 1.25-mm thickness. Lung image sets
dation of models and calculators for predicting were reconstructed with the use of a high-spatial-
the probability of lung cancer in pulmonary nod- frequency algorithm, and mediastinal image sets
ules using data from two separate low-dose CT with the use of an intermediate-spatial-frequency
screening cohorts. algorithm. A designated radiologist at each site
who had specific training in chest radiology re-
Me thods viewed the CT scans (see Text S1 in the Supple-
mentary Appendix).
Study Oversight In the BCCA studies, low-dose CT scanning
The development data set included participants was initially performed on a single-slice CT
enrolled in the multicenter Pan-Canadian Early scanner and subsequently on 4-, 8-, or 16-detec-
Detection of Lung Cancer Study (PanCan). The tor CT scanners, as reported previously.9,10 The
validation data set included participants enrolled CT scans were obtained at 120 kVp, 40 to 80 mA,
in several chemoprevention trials sponsored by and rotation times of up to 1 second. Initially,
the U.S. National Cancer Institute and conducted images were reconstructed at 7 mm in the 22%
by the British Columbia Cancer Agency (BCCA). of the participants who were enrolled between
In both the PanCan and BCCA studies, an epide- 2000 and early 2002; subsequently, images were
miologic questionnaire was administered and reconstructed at a 1.25-mm and 1-mm slice
spirometry was performed5,6 at baseline. Ethics width with the use of both the intermediate
approval was obtained from each participating (standard or B35f) and high-spatial-frequency
study center, and written informed consent was (bone or B60f) reconstruction algorithms. A sin-
provided by all participants. The first three au- gle radiologist who had specific training in chest
thors and the last author vouch for the accuracy radiology reviewed all images.
and completeness of the data. In both cohorts, a CT scan was considered to
be abnormal if it showed any noncalcified pul-
Study Participants monary nodule or area of nonsolid density at
Details of the PanCan are provided in the Supple- least 1 mm in diameter on lung parenchymal
mentary Appendix, available with the full text of windows. A nodule was considered to be benign
this article at NEJM.org. In brief, the population- if it showed a benign calcification pattern (e.g.,
based sample included current and former smok- fully calcified or popcorn calcification) or if the
n engl j med 369;10 nejm.org september 5, 2013 911
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
size of a solid nodule was unchanged for at least that included only predictors that were signifi-
2 years. Documented characteristics of the nod- cant (at P<0.05), and the second set, a fuller model
ules included their maximum transverse size, that included additional predictors that were
the visually determined type (nonsolid or with thought a priori to be associated with the risk of
ground-glass opacity, part-solid or subsolid, or lung cancer if the P values for them were less
solid or perifissural), and the location in the lung. than 0.25. In these analyses, the unit of analysis
The presence of visually detected emphysema was the nodule. Because some persons had mul-
was noted.9,10 The presence or absence of spicu- tiple nodules, the variances of effect estimates
lation was recorded for nodules in the PanCan were adjusted for clustering of data within per-
cohort but not for those in the BCCA cohort. sons with the use of the Huber–White robust
Only participants with at least one noncalci- (sandwich) variance estimator.14
fied lung nodule on the baseline low-dose CT Nonlinear effects of continuous variables were
scan were included in this analysis. These par- evaluated with the use of locally weighted scat-
ticipants were followed with repeat low-dose CT terplot smoothing (LOWESS) plots and multi-
at 3-to-12-month intervals, with the interval de- variable fractional polynomials.15 We evaluated
termined by the maximum diameter of the long interactions between important predictors in fi-
axis of the largest nodule, until any of the follow- nal models by including interaction terms along
ing occurred: all nodules were seen to be stable with main-effect terms. None of the interactions
for at least 2 years, the nodules were no longer we tested were significant, and they are not dis-
visible, benign calcification developed, or the cussed further in this article.
nodules were determined to be benign or malig- We evaluated the predictive performance of
nant on biopsy or surgical resection. the model by assessing its discrimination (ability
to classify correctly) and its calibration (whether
Diagnosis of Lung Cancer probabilities predicted by the model match ob-
The diagnosis of lung cancer was made by histo- served probabilities). Discrimination was mea-
pathological examination of resection specimens sured with the use of the area under the receiver-
or cytopathological examination of needle-aspi- operating-characteristic curve (AUC). All AUCs
ration biopsy samples. A microcoil localization reported are presented with bootstrap bias-
technique was used to mark the nodule under CT corrected 95% confidence intervals, with boot-
guidance before surgical resection.11 Resected strapping techniques based on 1000 bootstrapped
tumors were classified with the use of the World samples.16 We evaluated calibration by subtract-
Health Organization classification of lung neo- ing the model-estimated probability from the
plasms.12 observed probability for each study participant,
placing these absolute errors in rank order, and
Statistical Analysis evaluating the magnitude of the median and
Descriptive statistics were prepared with the use 90th percentile of the absolute errors.17 In addi-
of contingency-table analyses for categorical data tion, the mean absolute errors for each decile of
and Fisher’s exact test. The 95% confidence in- model-predicted risk were evaluated.
tervals for proportions were estimated with the Prediction models developed in the PanCan
use of the binomial exact method. Ordinal data cohort (excluding spiculation as a predictor) were
were compared with the use of a nonparametric validated externally by means of an assessment
test of trend,13 and continuous data with the use of discrimination and calibration in BCCA data.
of Student’s t-test. Multivariable logistic-regres- We assessed the performance of the model, ex-
sion models were prepared to estimate the risk of cluding and including spiculation, by calculating
lung cancer associated with potential predictors, the AUC in the PanCan data. In addition, we
including sociodemographic variables and clini- analyzed the improvement in the classification
cal variables such as smoking exposure and nod- of cases, noncases, and overall data with the
ule characteristics. Inclusion of variables in the inclusion of spiculation in the final model using
models was based on existing knowledge of risk net reclassification improvement with the follow-
factors for lung cancer and on nodule character- ing risk strata: low-risk (<5%), intermediate-risk
istics that are readily discernible on low-dose CT (≥5% to <10%), and high-risk (≥10%).18 All re-
images. Two sets of predictive models were pre- ported P values are two-sided, unless otherwise
pared. The first set was a parsimonious model indicated. The statistical analysis was performed
912 n engl j med 369;10 nejm.org september 5, 2013
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
Probability of Cancer in CT-Detected Pulmonary Nodules
and figures were prepared with the use of Stata/ lung cancer in a significant nonlinear relation-
MP, version 12.1. ship (P<0.001 for nonlinearity). The nonlinear
relationship was modeled with the use of multi-
R e sult s variable fractional polynomials and is depicted
graphically in Figure 1. The transformation of
Study Participants nodule size used in modeling is described in
A total of 2537 persons were enrolled in the Pan- Table 2.
Can, and at the time of the current analysis, the The majority of nodules were solid in appear-
median overall follow-up was 3.1 years (range, ance (78.9% in the PanCan data set and 79.8%
2.1 to 4.3). During this period, 187 participants in the BCCA data set) (Table 1). Nonsolid and
(7.4%) were lost to follow-up. The mean time un- part-solid nodules accounted for 15.8% and 4.3%
til loss to follow-up among participants without of nodules, respectively, in the PanCan group
nodules and those with nodules was 1.03 and and 9.3% and 0.9%, respectively, in the BCCA
1.12 years, respectively. Overall, loss to follow-up group. The remaining nodules were perifissural.
was significantly less likely to occur among par- The relationships between these nodule types
ticipants with nodules than among those without and cancer are described in the section below
nodules (odds ratio, 0.65; 95% confidence inter- describing the predictive model. No perifissural
val [CI], 0.47 to 0.99; P = 0.007). In the PanCan, nodule was malignant. When the data from the
1871 of the 2537 participants (73.7%) had a total two studies were pooled, the probability of lung
of 7008 lung nodules. Of the participants with cancer in perifissural nodules was zero (0 of 571
nodules, 102 had nodules that were malignant nodules; one-sided 97.5% CI, 0 to 0.006).
(5.5%). In the BCCA validation study, 1090 par- The location of a nodule was evaluated ac-
ticipants had 5021 nodules, and 40 of the 1090 cording to lobar distribution. A larger number of
persons with nodules (3.7%) were found to have nodules and a larger number of cancers were
42 lung cancers during a median follow-up of observed in the left upper and right upper lobes
8.6 years (range, 2.6 to 12.6). The characteristics than in the left or right lower lobes or the right
of the participants are described in Table S1 in middle lobe (Table 1). For this reason, the left
the Supplementary Appendix. The PanCan and upper and right upper lobes were compared with
BCCA study populations were similar with re- the other lobes in multivariable analysis.
spect to age, sex, body-mass index, percentage of The number of nodules per person was simi-
patients with emphysema, and percent of pre- lar in the two data sets: a median of 5 nodules
dicted forced expiratory volume in 1 second per person (interquartile range, 3 to 9) among the
(FEV1). The BCCA participants were less likely PanCan participants and 7 (interquartile range,
than the participants in the PanCan to have a 4 to 13) among BCCA participants. In both data
family history of lung cancer (18.4% vs. 32.4%) sets, the mean and median nodule counts were
and more likely to be former smokers (81.0% vs. lower when cancer was present (Table 1).
38.8%) and had a history of fewer pack-years of
smoking (48.3 vs. 54.8). In a univariate analysis, Predictive Model
the following variables were consistently associ- Because data on the presence or absence of spic-
ated with lung cancer: older age, any emphysema ulation were not collected in the BCCA studies,
as observed on CT images, and lower percent of we prepared parsimonious and full models that
predicted FEV1. did not include spiculation as a variable (Table 2,
models 1a and 2a, respectively) and that did in-
Pulmonary Nodules clude spiculation as a variable (Table 2, models 1b
The characteristics of the nodules, according to and 2b, respectively). The variables listed in Table 1
lung-cancer status, are shown in Table 1. In a and in Table S1 in the Supplementary Appendix
univariate analysis, significant consistent predic- were evaluated for inclusion in the models.
tors of lung cancer included the size, type (non- In the parsimonious model with spiculation
solid, part-solid, or solid), and location of the (Table 2, model 1b), the diagnosis of cancer in a
nodules, and the number of nodules that were nodule was associated with female sex, increas-
detected. Spiculation was a significant predictor ing size of the nodule, location of the nodule in
in the PanCan data. the upper lung, and spiculation, and in the full
The size of the nodule was associated with models (models 2a and 2b) additional predictors
n engl j med 369;10 nejm.org september 5, 2013 913
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
914
Table 1. Distribution of Nodule Variables, According to Lung-Cancer Status, in the Development and Validation Study Data Sets.*
Variable PanCan Development Cohort BCCA Validation Cohort
Benign Nodule Lung Cancer Total Benign Nodule Lung Cancer Total
(N = 6906) (N = 102) (N = 7008) P Value (N = 4979) (N = 42) (N = 5021) P Value
Nodule size — mm
Mean 4.1±3.1 15.7±12.2 4.3±3.7 <0.001† 3.6±2.2 13.9±7.4 3.7±2.5 <0.001†
Median 3.4 13 3.5 3 12.8 3
Range 1–70 2–86 1–86 1–29 3–45 1–45
Interquartile range 2.7–5.0 8–19 2.8–5.0 2.0–4.5 9–18 2.0–4.8
The
Nodule type — no./total no. (%)
Nonsolid or ground-glass opacity 1084/1105 (98.1) 21/1105 (1.9) 1105/6989 (15.8) 461/467 (98.7) 6/467 (1.3) 467/5021 (9.3)
Perifissural 70/70 (100) 0/70 70/6989 (1.0) 501/501 (100) 0/501 501/5021 (10.0)
Part-solid 283/303 (93.4) 20/303 (6.6) 303/6989 (4.3) 35/45 (77.8) 10/45 (22.2) 45/5021 (0.9)
Solid 5450/5511 (98.9) 61/5511 (1.1) 5511/6989 (78.9) <0.001‡ 3982/4008 (99.4) 26/4008 (0.6) 4008/5021 (79.8) <0.001‡
Nodule location — no./total no. (%)
Left lower lobe 1116/1128 (98.9) 12/1128 (1.1) 1128/6964 (16.2) 852/863 (98.7) 11/863 (1.3) 863/5021 (17.2)
Left upper lobe 1581/1612 (98.1) 31/1612 (1.9) 1612/6964 (23.1) 1277/1285 (99.4) 8/1285 (0.6) 1285/5021 (25.6)
n e w e ng l a n d j o u r na l
Right lower lobe 1249/1270 (98.3) 21/1270 (1.7) 1270/6964 (18.2) 829/830 (99.9) 1/830 (0.1) 830/5021 (16.5)
The New England Journal of Medicine
of
Right middle lobe 685/687 (99.7) 2/687 (0.3) 687/6964 (9.9) 503/504 (99.8) 1/504 (0.2) 504/5021 (10.0)
Right upper lobe 2232/2267 (98.5) 35/2267 (1.5) 2267/6964 (32.6) 0.01‡ 1518/1539 (98.6) 21/1539 (1.4) 1539/5021 (30.7) 0.002‡
n engl j med 369;10 nejm.org september 5, 2013
Nodule count at baseline
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
m e dic i n e
Mean 6.2±4.0 4.8±3.5 6.2±4.0 <0.001† 10.3±9.8 4.7±3.7 10.2±9.8 <0.001†
Median 5 4 5 7 4 7
Range 1–31 1–19 1–31 1–60 1–14 1–60
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Interquartile range 3–9 2–6 3–9 4–13 2–6 4–13
Spiculation — no./total no. (%)§
No 6739/6811 (98.9) 72/6811 (1.1) 6811/7008 (97.2)
Yes 167/197 (84.8) 30/197 (15.2) 197/7008 (2.8) 0.001‡
Probability of Cancer in CT-Detected Pulmonary Nodules
included older age, family history of lung cancer,
emphysema, lower nodule count, and part-solid
¶ Adenocarcinoma in situ (formerly bronchioloalveolar carcinoma) was defined according to the International Association for the Study of Lung Cancer–American Thoracic Society–
nodules as compared with solid nodules (with
nonsolid or ground-glass opacity nodules at a
reduced risk as compared with solid nodules).
Both parsimonious and full models showed ex-
cellent discrimination in the PanCan and BCCA
(validation) data with all AUCs more than 0.90
(Fig. S1 and Table S2 in the Supplementary Ap-
pendix). In the PanCan and BCCA data sets,
32/42 (76.2)
5/42 (11.9)
* Plus–minus values are means ±SD. BCCA denotes British Columbia Cancer Agency, and PanCan Pan-Canadian Early Detection of Lung Cancer Study.
3/42 (7.1)
1/42 (2.4)
1/42 (2.4)
model-predicted probabilities of lung cancer
showed good separation between participants in
0/42
whom lung cancer was diagnosed and those in
whom it was not diagnosed, with only modest
overlap (Fig. 2). The models performed well even
when applied to nodules 10 mm or smaller,
which are the most clinically challenging and
most numerous nodules. For those nodules, the
AUCs in model 1a were 0.894 and 0.907 in the
PanCan and BCCA data, respectively (Fig. S1 in
§ The presence or absence of spiculation was recorded for nodules in the PanCan cohort but not in the BCCA cohort.
the Supplementary Appendix).
In the PanCan data, a modified model 1b in
which nodule size was treated as a linear term
‖ Other histologic types included neuroendocrine and mixed small-cell and non–small-cell lung cancers.
had a significantly lower AUC than did the model
in which nodule size was treated as a nonlinear
term (0.918 vs. 0.941, P = 0.01 for the difference
in AUCs). Although nodule size was the single
most important predictor in the multivariable
models, the largest lung nodule in a person was
† This P value was calculated with the use of Student’s t-test with unequal variance.
not necessarily determined to be malignant.
75/102 (73.5)
14/102 (13.7)
5/102 (4.9)
3/102 (2.9)
3/102 (2.9)
2/102 (2.0)
Among the 102 PanCan participants with lung
cancer, cancer was detected in the largest nodule
European Respiratory Society classification of lung adenocarcinoma.19
in 82 participants, in the second largest in 16, in
the third largest in 1, in the fourth largest in 2,
and in the fifth largest in 1.
‡ This P value was calculated with the use of Fisher’s exact test.
In the BCCA validation data, the full model
performed significantly better than the parsimo-
nious model: the AUC was 0.960 (95% CI, 0.927
to 0.980) in model 1a as compared with 0.970
(95% CI, 0.947 to 0.986) in model 2a (P = 0.009
Histopathological type — no./total no. (%)
Non–small-cell lung cancer, not other-
for the difference in AUC), and the difference was
particularly pronounced for the clinically rele-
vant group of nodules 10 mm or smaller in size:
an AUC of 0.907 (95% CI, 0.822 to 0.963) as com-
Adenocarcinoma in situ¶
pared with an AUC of 0.938 (95% CI, 0.872 to
0.978) (P = 0.002). The difference in AUC of 0.031
wise specified
Adenocarcinoma
is 6.2% of the distance between random and per-
Squamous cell
fect classification.
Small-cell
In model 1a, the median and 90th percentile
Other‖
absolute errors (observed minus predicted prob-
abilities) in the analysis of the PanCan data were
0.0003 and 0.0007, respectively, and the corre-
n engl j med 369;10 nejm.org september 5, 2013 915
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
A All Nodules B Nodules ≤20 mm
0.6 0.15
Probability of Lung Cancer
Probability of Lung Cancer
0.4 0.10
0.2 0.05
0.0 0.00
0 20 40 60 80 0 5 10 15 20
Nodule Size (mm) Nodule Size (mm)
C Nodules ≤10 mm D Nodules ≤6 mm
0.04 0.008
Probability of Lung Cancer
Probability of Lung Cancer
0.03 0.006
0.02 0.004
0.01 0.002
0.00 0.000
0 2 4 6 8 10 1 2 3 4 5 6
Nodule Size (mm) Nodule Size (mm)
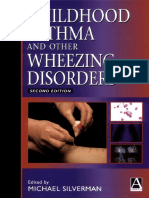
Figure 1. Relationship between Nodule Size and Probability That a Nodule Is Lung Cancer.
The reference variables for this model were male sex, lower or middle lobe location, and no spiculation. Estimates
of variables are taken from the parsimonious model with spiculation.
sponding absolute errors in the analysis of the study. Current clinical guidelines are complex
BCCA validation data were 0.0002 and 0.003. In and vary according to the size and appearance of
model 1a, the mean absolute error in all deciles the nodule. Figure S3 and Table S2 in the Supple-
of model-predicted risk in the PanCan and BCCA mentary Appendix show the way in which the pre-
data was less than 0.015 (Fig. S2 in the Supplemen- diction accuracies of our models vary according
tary Appendix), indicating excellent calibration. to risk cutoff points for defining a positive screen-
The final models with spiculation are present- ing result. For example, if a threshold of at least
ed in Table 2, models 1b and 2b. A comparison a 5% risk of cancer is used with the parsimoni-
of the model with and without spiculation re- ous model including spiculation (Table 2, model
vealed no significant difference in AUC (Table S2 1b), the sensitivity, specificity, positive predictive
in the Supplementary Appendix). However, the value, and negative predictive value are 71.4%,
net reclassification improvement between model 95.5%, 18.5% and 99.6%, respectively. Only 5.5%
1a and model 1b was 4.3% (P = 0.09), suggesting of the nodules would be classified as positive.
that spiculation might improve prediction.
We provide spreadsheet calculators for Ta- Discussion
ble 2, models 1b and 2b, at www.brocku.ca/
cancerpredictionresearch. These calculators fa- This evidence-based, prospective study of two
cilitate the calculation of the probability that a high-risk screening cohorts determined the prob-
pulmonary nodule is lung cancer. ability that pulmonary nodules detected by screen-
ing low-dose CT would be cancerous; each nod-
Application in the Screening Setting ule was prospectively followed for at least 2 years.
In the screening setting, one of the most difficult Our models show excellent predictive accuracy,
decisions is whether CT or another investigation with AUCs of at least 0.94 in an external vali
is needed before the next annual low-dose CT dation cohort. Even for lung nodules that were
916 n engl j med 369;10 nejm.org september 5, 2013
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
Probability of Cancer in CT-Detected Pulmonary Nodules
Table 2. Prediction Models for the Probability of Lung Cancer in Pulmonary Nodules.*
Model 1a: Model 2a:
Predictor Variables Parsimonious Model, No Spiculation Full Model, No Spiculation
Odds Ratio Beta Odds Ratio Beta
(95% CI) P Value Coefficient (95% CI) P Value Coefficient
Age, per yr 1.03 (0.99–1.07) 0.11 0.0321
Sex, female vs. male 1.79 (1.13–2.82) 0.01 0.5806 1.76 (1.09–2.83) 0.02 0.5635
Family history of lung cancer, yes vs. no 1.35 (0.84–2.16) 0.21 0.3013
Emphysema, yes vs. no 1.41 (0.82–2.42) 0.21 0.3462
Nodule size <0.001† −5.8616 <0.001† −5.6693
Nodule type
Nonsolid or with ground-glass opacity 0.74 (0.40–1.35) 0.33 −0.3005
Part-solid 1.40 (0.72–2.74) 0.32 0.3395
Solid Reference Reference
Nodule location, upper vs. middle or 1.90 (1.78–3.08) 0.009 0.6439 2.04 (1.22–3.41) 0.007 0.7116
lower lobe
Nodule count per scan, per each additional 0.92 (0.85–1.00) 0.05 −0.0803
nodule
Model constant −6.5929 −6.8071
Model 1b: Model 2b:
Parsimonious Model, with Spiculation Full Model, with Spiculation
Odds Ratio P Value Beta Odds Ratio P Value Beta
(95% CI) Coefficient (95% CI) Coefficient
Age, per yr 1.03 (0.99–1.07) 0.16 0.0287
Sex, female vs. male 1.91 (1.19–3.07) 0.008 0.6467 1.82 (1.12–2.97) 0.02 0.6011
Family history of lung cancer, yes vs. no 1.34 (0.83–2.17) 0.23 0.2961
Emphysema, yes vs. no 1.34 (0.78–2.33) 0.29 0.2953
Nodule size <0.001† −5.5537 <0.001† −5.3854
Nodule type
Nonsolid or with ground-glass opacity 0.88 (0.48–1.62) 0.68 −0.1276
Part-solid 1.46 (0.74–2.88) 0.28 0.3770
Solid Reference Reference
Nodule location, upper vs. middle or 1.82 (1.12–2.98) 0.02 0.6009 1.93 (1.14–3.27) 0.02 0.6581
lower lobe
Nodule count per scan, per each additional 0.92 (0.85–1.00) 0.049 −0.0824
nodule
Spiculation, yes vs. no 2.54 (1.45–4.43) 0.001 0.9309 2.17 (1.16–4.05) 0.02 0.7729
Model constant −6.6144 −6.7892
* Models 1a and 1b are parsimonious prediction models, and Models 2a and 2b are full logistic-regression prediction models. Age is centered
on the mean of 62 years, nodule size is centered on 4 mm, and nodule count is centered on 4 (i.e., 62 is subtracted from the actual age,
4 mm is subtracted from the actual nodule size, and 4 is subtracted from the actual number of nodules).
† Nodule size had a nonlinear relationship with lung cancer and is transformed in this model. The odds ratio of the transformed variable has
no direct interpretation without back-transformation. Nodule-size transformation, which is based on multiple fractional polynomial analy-
( )
ses, was performed with the following calculation: (Nodule size)−0.5 −1.58113883; nodule size was measured in millimeters.
10
10 mm or smaller, for which clinical manage- upper lobes increased the probability of cancer.20
ment decisions are the most challenging, the We have provided strong evidence that perifis-
AUC remained excellent (>0.90) in the validation sural nodules represent a minimal risk of lung
cohort. Our results showed that the relationship cancer and probably do not require longitudinal
between nodule size and cancer was nonlinear. follow-up with CT.21,22 Although variables such
We also confirmed that nodule location in the as smoking history, body-mass index, and per-
n engl j med 369;10 nejm.org september 5, 2013 917
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
A No Lung Cancer, PanCan Data (6774 nodules) B Lung Cancer, PanCan Data (98 nodules)
100 100
Percent of Nodules
Percent of Nodules
50 50
0 0
0 0.2 0.4 0.6 0.8 0 0.2 0.4 0.6 0.8
Probability Probability
C No Lung Cancer, BCCA Data (4478 nodules) D Lung Cancer, BCCA Data (42 nodules)
100 100
Percent of Nodules
Percent of Nodules
50 50
0 0
0 0.2 0.4 0.6 0 0.2 0.4 0.6
Probability Probability
Figure 2. Distributions of Lung-Cancer Probabilities.
The distribution of lung-cancer probabilities, based on the parsimonious model without spiculation, is shown among
persons with lung cancer and those without lung cancer in the Pan-Canadian Early Detection of Lung Cancer Study
(PanCan) and British Columbia Cancer Agency (BCCA) data sets. Perifissural nodules and nodules with any missing
value in any predictor were not included in the calculation.
cent of predicted FEV1 identify smokers at risk for or part-solid nodules, which are rarely visible on
lung cancer,8 they were not independently associ- a chest radiograph. Split-sample development and
ated with lung cancer in the fully adjusted model. validation sets were generally used in the previ-
The usefulness of the model in low-risk persons ous studies, and the split-sample approach is
for whom screening is not currently recommend- inferior to the use of a true external validation
ed is beyond the scope of our study. Our model set from a unique sample. When their models
also does not apply to persons with hilar or me- are validated externally, the accuracies of their
diastinal lymphadenopathy, for whom further predictions appear to be inferior to those of our
investigations are warranted irrespective of the models.25 Our models are coupled with risk cal-
nodule size. culators, which make possible the rapid and easy
Previous prediction models for lung nodules calculation of lung-cancer risk given the charac-
were hospital-based or clinic-based and showed teristics of the person and the nodules.
a high prevalence of lung cancer — 23 to 75%, CT practice guidelines for the follow-up of
as compared with 5.5% in our study.23-25 Some noncalcified nodules have been developed on the
studies were retrospective in design, had smaller basis of expert opinion and clinic or hospital
sample sizes, and did not evaluate nonlinear ef- databases that include large proportions of per-
fects; in addition, chest radiography was used to sons with lung cancer.4,26-28 Currently, the follow-
detect lung nodules.23,24 These models may not up strategy is based on the size of the largest de-
be applicable to screening by means of low-dose tected lesion and may vary depending on whether
CT, since more than 50% of lung cancers detected the lung nodule is solid, part-solid, or non
by low-dose CT are 2 cm in size or smaller and solid.4,27,28 Our study showed that in 20% of the
almost one quarter of lung nodules are nonsolid participants, the largest lung nodule was not the
918 n engl j med 369;10 nejm.org september 5, 2013
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
Probability of Cancer in CT-Detected Pulmonary Nodules
one that was malignant or determined to be In approximately 25% of the surgical procedures,
malignant on follow-up. Although volumetric the nodule was determined to be benign.1,31
CT may be useful to characterize volume and Discrimination of nodules that are lung cancer
mass,29,30 a second CT is required to determine from those that are not is a primary medical
the growth rate or a change in mass, and cur- concern. The accurate assessment of risk before
rently volumetric CT cannot be performed accu- additional imaging and volumetric analysis has
rately for nonsolid or part-solid lesions. In previ- an important place in lung-cancer screening.
ously reported studies, including the Dutch–Belgian The implementation of our nodule risk-predic-
Randomized Lung Cancer Screening Trial tion models and coupled calculators is expected
(NELSON), more than 20% of participants who to improve clinical and public health practice.
underwent low-dose CT screening required a Supported by the Terry Fox Research Institute, the Canadian
repeat CT, positron-emission tomographic imag- Partnership Against Cancer, and U.S. Public Health Service con-
ing, or a biopsy procedure within 12 months tracts (N01-CN-85188, U01CA96109, PO1 CA096964-01A1, and
N01-CN 35000) from the National Cancer Institute.
after their first screening low-dose CT because Disclosure forms provided by the authors are available with
of suspicious or intermediate lung nodules.1,3,29,30 the full text of this article at NEJM.org.
References
1. Aberle DR, Adams AM, Berg CD, et al. coscopic surgical resection. Radiology H, Prokop M. Pulmonary perifissural
Reduced lung cancer mortality with low- 2009;250:576-85. nodules on CT scans: rapid growth is not
dose computed tomographic screening. 12. International Agency for Research on a predictor of malignancy. Radiology 2012;
N Engl J Med 2011;365:395-409. Cancer. Pathology and genetics of tumors 265:611-6.
2. Croswell JM, Baker SG, Marcus PM, of the lung, pleura, thymus and heart. 23. Swensen SJ, Silverstein MD, Ilstrup
Clapp JD, Kramer BS. Cumulative inci- Lyon, France: IARC Press, 2004. DM, Schleck CD, Edell ES. The probability
dence of false-positive results in lung can- 13. Cuzick J. A Wilcoxon-type test for of malignancy in solitary pulmonary nod-
cer screening: a randomized trial. Ann trend. Stat Med 1985;4:87-90. ules: application to small radiologically
Intern Med 2010;152:505-12. 14. White H. A heteroskedasticity-consis- indeterminate nodules. Arch Intern Med
3. Bach PB, Mirkin JN, Oliver TK, et al. tent covariance matrix estimator and a 1997;157:849-55.
Benefits and harms of CT screening for direct test for heteroskedasticity. Econo- 24. Gould MK, Ananth L, Barnett PG.
lung cancer: a systematic review. JAMA metrica 1980;48:817-38. A clinical model to estimate the pretest
2012;307:2318-29. 15. Royston P, Sauerbrei W. Multivariable probability of lung cancer in patients with
4. Wood DE, Eapen GA, Ettinger DS, et al. model-building: a pragmatic approach to solitary pulmonary nodules. Chest 2007;
Lung cancer screening. J Natl Cancer regression analysis based on fractional 131:383-8.
Compr Netw 2012;10:240-65. polynomials for modelling continuous 25. Schultz EM, Sanders GD, Trotter PR,
5. American Thoracic Society. Standard- variables. Hoboken, NJ: Wiley, 2008. et al. Validation of two models to estimate
ization of spirometry, 1994 update. Am J 16. Pepe M, Longton G, Janes H. Estima- the probability of malignancy in patients
Respir Crit Care Med 1995;152:1107-36. tion and comparison of receiver operating with solitary pulmonary nodules. Thorax
6. Crapo RO, Morris AH, Gardner RM. characteristic curves. Stata J 2009;9:1. 2008;63:335-41.
Reference spirometric values using tech- 17. Harrell FE. Regression modeling strat- 26. Ost DE, Gould MK. Decision making
niques and equipment that meet ATS rec- egies: with applications to linear models, in patients with pulmonary nodules. Am J
ommendations. Am Rev Respir Dis 1981; logistic regression, and survival analysis. Respir Crit Care Med 2012;185:363-72.
123:659-64. New York: Springer, 2001. 27. MacMahon H, Austin J, Gamsu G,
7. Tammemagi CM, Pinsky PF, Caporaso 18. Pencina MJ, D’Agostino RB Sr, D’Agos et al. Guidelines for management of small
NE, et al. Lung cancer risk prediction: tino RB Jr, Vasan RS. Evaluating the added pulmonary nodules detected on CT scans:
Prostate, Lung, Colorectal and Ovarian predictive ability of a new marker: from a statement from the Fleischner Society.
Cancer Screening Trial models and vali- area under the ROC curve to reclassifica- Radiology 2005;237:395-400.
dation. J Natl Cancer Inst 2011;103:1058- tion and beyond. Stat Med 2008;27:157-72. 28. Naidich DP, Bankier AA, MacMahon H,
68. 19. Travis WD, Brambilla E, Noguchi M, et al. Recommendations for the manage-
8. Tammemägi MC, Katki HA, Hocking et al. International Association for the ment of subsolid pulmonary nodules de-
WB, et al. Selection criteria for lung-cancer Study of Lung Cancer/American Thoracic tected at CT: a statement from the Fleisch-
screening. N Engl J Med 2013;368:728-36. Society/European Respiratory Society in- ner Society. Radiology 2013;266:304-17.
9. McWilliams A, Mayo J, MacDonald S, ternational multidisciplinary classification 29. van Klaveren RJ, Oudkerk M, Prokop M,
et al. Lung cancer screening: a different of lung adenocarcinoma. J Thorac Oncol et al. Management of lung nodules de-
paradigm. Am J Respir Crit Care Med 2011;6:244-85. tected by volume CT scanning. N Engl J
2003;168:1167-73. 20. Horeweg N, van der Aalst CM, Thun- Med 2009;361:2221-9.
10. McWilliams AM, Mayo JR, Ahn MI, nissen E, et al. Characteristics of lung 30. Ru Zhao Y, Xie X, de Koning HJ, Mali
MacDonald SL, Lam SC. Lung cancer cancers detected by computer tomography WP, Vliegenthart R, Oudkerk M. NELSON
screening using multi-slice thin-section screening in the randomized NELSON lung cancer screening study. Cancer Im-
computed tomography and autofluores- trial. Am J Respir Crit Care Med 2013; aging 2011;11:S79-S84.
cence bronchoscopy. J Thorac Oncol 2006; 187:848-54. 31. Swensen SJ, Jett JR, Hartman TE, et al.
1:61-8. 21. Ahn MI, Gleeson TT, Chan IH, et al. CT screening for lung cancer: five-year
11. Mayo JR, Clifton JC, Powell TI, et al. Perifissural nodules seen at CT screening prospective experience. Radiology 2005;
Lung nodules: CT-guided placement of for lung cancer. Radiology 2010;254:949-56. 235:259-65.
microcoils to direct video-assisted thora- 22. de Hoop B, van Ginneken B, Gietema Copyright © 2013 Massachusetts Medical Society.
n engl j med 369;10 nejm.org september 5, 2013 919
The New England Journal of Medicine
Downloaded from nejm.org on January 16, 2018. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
Вам также может понравиться
- Aula LogisticaДокумент64 страницыAula LogisticaglaucomassotoОценок пока нет
- Nejmoa1208962 PDFДокумент12 страницNejmoa1208962 PDFPutri Alif PermatasariОценок пока нет
- MicronodulosДокумент9 страницMicronodulosWildcane SalmeronОценок пока нет
- Circulating Tumor DNA and Radiological Tumor VolumДокумент7 страницCirculating Tumor DNA and Radiological Tumor Volumnaomireyes01Оценок пока нет
- Management of The Solitary Pulmonary NoduleДокумент6 страницManagement of The Solitary Pulmonary Nodulevictor ibarra romeroОценок пока нет
- 408 2020 Article 407Документ11 страниц408 2020 Article 407CuchuluuОценок пока нет
- Pros: Long-Term CT Scan Follow-Up Should Be The Standard of Care in Patients Who Are Curatively Treated For An Early-Stage Non-Small Cell Lung CancerДокумент3 страницыPros: Long-Term CT Scan Follow-Up Should Be The Standard of Care in Patients Who Are Curatively Treated For An Early-Stage Non-Small Cell Lung CancerPaulius GecasОценок пока нет
- Lung SOL - Cytology and Histological Correlation in A Tertiary Care CentreДокумент7 страницLung SOL - Cytology and Histological Correlation in A Tertiary Care CentreIOSRjournalОценок пока нет
- Diagnosis and Staging of Lung Carcinoma With CT Scan and Its Histopathological CorrelationДокумент7 страницDiagnosis and Staging of Lung Carcinoma With CT Scan and Its Histopathological CorrelationinesОценок пока нет
- ACCP Lung Cancer 2013Документ25 страницACCP Lung Cancer 2013Hendarsyah SuryadinataОценок пока нет
- The Solitary Pulmonary NoduleДокумент11 страницThe Solitary Pulmonary NoduleShahid HussainОценок пока нет
- JTD 11 03 936Документ8 страницJTD 11 03 936Heru SigitОценок пока нет
- Survival of Patients With Stage I Lung Cancer Detected On CT SCR 2006Документ9 страницSurvival of Patients With Stage I Lung Cancer Detected On CT SCR 2006Mara MoránОценок пока нет
- Jama Mazzone 2022 RV 210019 1641843868.64143Документ10 страницJama Mazzone 2022 RV 210019 1641843868.64143Javier RiquelmeОценок пока нет
- Predicting Lung Nodules MalignancyДокумент7 страницPredicting Lung Nodules MalignancyhajajОценок пока нет
- Multi-Institutional External Validation of Urinary TWIST1 and NID2 Methylation As A Diagnostic Test For Bladder CancerДокумент6 страницMulti-Institutional External Validation of Urinary TWIST1 and NID2 Methylation As A Diagnostic Test For Bladder CancerFarlinda AlyaОценок пока нет
- Jurnal Radiologi 2Документ21 страницаJurnal Radiologi 2Adelya Dwi AsyifaОценок пока нет
- HHS Public AccessДокумент15 страницHHS Public AccessSamuel WidjajaОценок пока нет
- 10 Rosenberg Vitamin CДокумент78 страниц10 Rosenberg Vitamin CЩербакова ЛенаОценок пока нет
- Ekstravasation of Ionated Contrast Medium in Cancer Patients Undergoing Computed TomographyДокумент6 страницEkstravasation of Ionated Contrast Medium in Cancer Patients Undergoing Computed TomographyHelena ChristyОценок пока нет
- Lungcancerscreening: Why, When, and How?Документ19 страницLungcancerscreening: Why, When, and How?Nelson William UsnayoОценок пока нет
- Comparison of Three View Thoracic Radiography and Computed Tomography For Detection of Pulmonary Nodules in Dogs With NeoplasiaДокумент7 страницComparison of Three View Thoracic Radiography and Computed Tomography For Detection of Pulmonary Nodules in Dogs With NeoplasiaJoffre VelasquezОценок пока нет
- DetectionДокумент9 страницDetectionHarshvardhan RavalОценок пока нет
- Hutchinson 2019 - Spectrum of Lung Adenocarcinoma PDFДокумент33 страницыHutchinson 2019 - Spectrum of Lung Adenocarcinoma PDFlutfiaОценок пока нет
- Lung Cancer Current Therapies and New Targeted TreatmentsДокумент13 страницLung Cancer Current Therapies and New Targeted TreatmentsWlad PaCaОценок пока нет
- Metastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyДокумент6 страницMetastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyMara PitrezОценок пока нет
- Review Article: Screening For Lung Cancer With Low-Dose Computed Tomography: A Review of Current StatusДокумент16 страницReview Article: Screening For Lung Cancer With Low-Dose Computed Tomography: A Review of Current StatusAnnizada Intan PratiwiОценок пока нет
- DX TX Cancer PulmonДокумент13 страницDX TX Cancer PulmonFernando AtenciaОценок пока нет
- Atm 08 20 1292Документ11 страницAtm 08 20 1292Ethel GeanОценок пока нет
- Cancers 15 03981 v2Документ33 страницыCancers 15 03981 v2abhi16243Оценок пока нет
- Nej Mo A 0900043Документ8 страницNej Mo A 0900043anggiОценок пока нет
- Assessment of Tumor Parameters As Factors of Aggressiveness in Colon Cancer 1584 9341 10 4 6Документ5 страницAssessment of Tumor Parameters As Factors of Aggressiveness in Colon Cancer 1584 9341 10 4 6Panuta AndrianОценок пока нет
- Thy 2011 0317Документ10 страницThy 2011 0317astriОценок пока нет
- ChestДокумент25 страницChestAmir RahbaranОценок пока нет
- NotesДокумент4 страницыNotesRaza HodaОценок пока нет
- 1 s2.0 S0169500221000453 MainДокумент4 страницы1 s2.0 S0169500221000453 MainNoman M HasanОценок пока нет
- A Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerДокумент9 страницA Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerOtoyGethuОценок пока нет
- Mccormick 2015Документ8 страницMccormick 2015Maria de Jesus Diaz SosaОценок пока нет
- Seminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresДокумент13 страницSeminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresseruniallisaaslimОценок пока нет
- The Solitary Pulmonary NoduleДокумент8 страницThe Solitary Pulmonary NoduleRafa IsaacОценок пока нет
- Imaging Characteristics of Nasopharyngeal Carcinoma For Predicting Distant MetastasisДокумент7 страницImaging Characteristics of Nasopharyngeal Carcinoma For Predicting Distant MetastasisJose JulianОценок пока нет
- Lotan Et Al. Molecular Marker For Rec and Cancer Specific Survival Post Radical CystectomyДокумент7 страницLotan Et Al. Molecular Marker For Rec and Cancer Specific Survival Post Radical CystectomyyuenkeithОценок пока нет
- CancerДокумент9 страницCancerFranklin MartinezОценок пока нет
- 10 1053@j Semnuclmed 2020 07 005Документ10 страниц10 1053@j Semnuclmed 2020 07 005anon_813722240Оценок пока нет
- Low-Dose Abdominal CT For Evaluating Suspected Appendicitis: Original ArticleДокумент10 страницLow-Dose Abdominal CT For Evaluating Suspected Appendicitis: Original ArticleThyo Amando PurbaОценок пока нет
- PNAS 2011 Ruiz 1104009108Документ6 страницPNAS 2011 Ruiz 1104009108TomO'MahoneyОценок пока нет
- Research Paper Feb 27Документ23 страницыResearch Paper Feb 27Bharath KОценок пока нет
- 1 s2.0 S014067362300020X MainДокумент14 страниц1 s2.0 S014067362300020X MainGERIATRIA 72Оценок пока нет
- 10.1097@00005382 201509000 00004 PDFДокумент6 страниц10.1097@00005382 201509000 00004 PDFJheyson Javier Barrios PereiraОценок пока нет
- 10 11648 J Ijmi 20170505 12Документ5 страниц10 11648 J Ijmi 20170505 12Anchit AggarwalОценок пока нет
- Lymph Nodes Esophageal Cancer Staging: Improved Accuracy by Endoscopic Ultrasound of CeliacДокумент5 страницLymph Nodes Esophageal Cancer Staging: Improved Accuracy by Endoscopic Ultrasound of CeliacPoonam JoshiОценок пока нет
- Research Paper On Lung DetecionДокумент5 страницResearch Paper On Lung DetecionHirdesh KumarОценок пока нет
- Esophageal Cancer Recurrence Patterns and Implicati 2013 Journal of ThoracicДокумент5 страницEsophageal Cancer Recurrence Patterns and Implicati 2013 Journal of ThoracicFlorin AchimОценок пока нет
- 2012 - Yoon Et Al. - Contouring Guidelines of The Inguinal Lymph Nodes Using Lymphangiograms For The Delivery of Radiation Therapy in GastroДокумент1 страница2012 - Yoon Et Al. - Contouring Guidelines of The Inguinal Lymph Nodes Using Lymphangiograms For The Delivery of Radiation Therapy in GastroPoljarLijanОценок пока нет
- Core Needle Biopsy For Screening Detected Lung Cancer-Does It Capture All in Light of Tumor Heterogeneity?-A Narrative ReviewДокумент9 страницCore Needle Biopsy For Screening Detected Lung Cancer-Does It Capture All in Light of Tumor Heterogeneity?-A Narrative Reviewrizki romadaniОценок пока нет
- Metaanaliza CT PDFДокумент17 страницMetaanaliza CT PDFm_manuela2002Оценок пока нет
- Screening and Early Diagnosis in Lung CancerДокумент46 страницScreening and Early Diagnosis in Lung CancerJuan J BretónОценок пока нет
- Non-Diagnostic CT-Guided Percutaneous Needle BiopsyДокумент12 страницNon-Diagnostic CT-Guided Percutaneous Needle BiopsyHeru SigitОценок пока нет
- Lymph Nodes Normal and MalignantДокумент12 страницLymph Nodes Normal and MalignantMagzОценок пока нет
- Bruce Lee Words of WisdomДокумент8 страницBruce Lee Words of WisdomVincent LivandyОценок пока нет
- The Exorcist: Directed byДокумент4 страницыThe Exorcist: Directed byVincent LivandyОценок пока нет
- GlutamatergicДокумент2 страницыGlutamatergicVincent LivandyОценок пока нет
- Breastfeeding, Also Known As Nursing, Is The Feeding ofДокумент1 страницаBreastfeeding, Also Known As Nursing, Is The Feeding ofVincent LivandyОценок пока нет
- Infectious Disease Bacteria Lungs Latent Tuberculosis Cough Blood-Containing Sputum Fever Night Sweats Weight Loss InfectionДокумент1 страницаInfectious Disease Bacteria Lungs Latent Tuberculosis Cough Blood-Containing Sputum Fever Night Sweats Weight Loss InfectionVincent LivandyОценок пока нет
- VomitingДокумент1 страницаVomitingVincent LivandyОценок пока нет
- 3.5. CPR & Electrical Therapies (Dr. Dian Ayu)Документ14 страниц3.5. CPR & Electrical Therapies (Dr. Dian Ayu)No NameeОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- OkjhgfgbnДокумент3 страницыOkjhgfgbnVincent LivandyОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- ZsxdcfvytybkjngДокумент3 страницыZsxdcfvytybkjngVincent LivandyОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- The Year in Cardiology 2013: Cardiovascular Disease PreventionДокумент6 страницThe Year in Cardiology 2013: Cardiovascular Disease PreventionVincent LivandyОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- ZSXDCFVGДокумент3 страницыZSXDCFVGVincent LivandyОценок пока нет
- Ijoes 2332 290X 02 202Документ8 страницIjoes 2332 290X 02 202Vincent LivandyОценок пока нет
- EIEEДокумент3 страницыEIEEVincent LivandyОценок пока нет
- ZSXDДокумент3 страницыZSXDVincent LivandyОценок пока нет
- Ijoes 2332 290X 02 202 PDFДокумент6 страницIjoes 2332 290X 02 202 PDFVincent LivandyОценок пока нет
- International Journal of Radiology and Imaging Technology Ijrit 3 026Документ4 страницыInternational Journal of Radiology and Imaging Technology Ijrit 3 026Vincent LivandyОценок пока нет
- Tips For Writing PapersДокумент32 страницыTips For Writing Papersssm_majeedОценок пока нет
- EarlyInfantileEpilepticEncephalopathy FRenPro889Документ7 страницEarlyInfantileEpilepticEncephalopathy FRenPro889Vincent LivandyОценок пока нет
- Antenatal CareДокумент12 страницAntenatal CarefiramnОценок пока нет
- Fluid and Electrolytes in Pediatrics - 978-1-60327-224-7Документ608 страницFluid and Electrolytes in Pediatrics - 978-1-60327-224-7Vincent Livandy100% (1)
- EIEEДокумент3 страницыEIEEVincent LivandyОценок пока нет
- Sympathetic Uveitis/ Ophthalmia: PG CornerДокумент4 страницыSympathetic Uveitis/ Ophthalmia: PG CornerVincent LivandyОценок пока нет
- Wheezing DisorderДокумент497 страницWheezing DisorderVincent LivandyОценок пока нет
- Wheezing DisorderДокумент497 страницWheezing DisorderVincent LivandyОценок пока нет
- Completing The Square PDFДокумент10 страницCompleting The Square PDFgreg heffleyОценок пока нет
- Chapter 7 Analysis of Stress and StrainДокумент20 страницChapter 7 Analysis of Stress and StrainLong Nguyễn HoàngОценок пока нет
- 1995 S320 S420 S500 Owner's Manual Edition C PDFДокумент153 страницы1995 S320 S420 S500 Owner's Manual Edition C PDFnpachecorecabarrenОценок пока нет
- Gen-Math11 - Q1 - Mod10 - Solving-Real-Life-Problems-Involving-Rational (EJBOY)Документ13 страницGen-Math11 - Q1 - Mod10 - Solving-Real-Life-Problems-Involving-Rational (EJBOY)Angeline TumananОценок пока нет
- Angular AccuracyДокумент4 страницыAngular AccuracySwatilekha ChowdhuryОценок пока нет
- DC Power Supply and Voltage RegulatorsДокумент73 страницыDC Power Supply and Voltage RegulatorsRalph Justine NevadoОценок пока нет
- DocuДокумент77 страницDocuDon'tAsK TheStupidOnesОценок пока нет
- Corner ReflectorДокумент1 страницаCorner ReflectorYashОценок пока нет
- Stability Analysis of Steel Storage Rack Structures PDFДокумент7 страницStability Analysis of Steel Storage Rack Structures PDFFabian Flemin BahamondeОценок пока нет
- T0000598REFTRGiDX 33RevG01052017 PDFДокумент286 страницT0000598REFTRGiDX 33RevG01052017 PDFThanhОценок пока нет
- Fongs ProgrammerДокумент5 страницFongs ProgrammerPankaj PolaraОценок пока нет
- Narayana Xii Pass Ir Iit (2023 24) PDFДокумент16 страницNarayana Xii Pass Ir Iit (2023 24) PDFRaghav ChaudharyОценок пока нет
- ADO NET Tutorial - 16Документ18 страницADO NET Tutorial - 16Fenil Desai100% (1)
- Acuvim II Profibus Modules Users Manual v1.10Документ36 страницAcuvim II Profibus Modules Users Manual v1.10kamran719Оценок пока нет
- L4 Subdivision of PlotsДокумент20 страницL4 Subdivision of PlotsKenny BoatОценок пока нет
- 002 Ac Yoke B100-ParkerДокумент2 страницы002 Ac Yoke B100-ParkerNubia BarreraОценок пока нет
- Body Deassembly 9 Interior TrimДокумент7 страницBody Deassembly 9 Interior TrimCarlos TecnicОценок пока нет
- Ampla's Technology ArchitectureДокумент4 страницыAmpla's Technology ArchitecturesyeadtalhaaliОценок пока нет
- ATR4518R2Документ2 страницыATR4518R2estebanarca50% (4)
- Bhagwat Gita in by EB KarkiДокумент97 страницBhagwat Gita in by EB KarkiYogaguru Mohan100% (1)
- CSS Lab ManualДокумент32 страницыCSS Lab ManualQaif AmzОценок пока нет
- Mathematics in The Modern World ReviewerДокумент2 страницыMathematics in The Modern World ReviewerVince Luigi ZepedaОценок пока нет
- Aluminum: DR 900 Analytical ProcedureДокумент4 страницыAluminum: DR 900 Analytical Procedurewulalan wulanОценок пока нет
- Translating Trig Graphs PDFДокумент4 страницыTranslating Trig Graphs PDFMark Abion ValladolidОценок пока нет
- Serie W11 PDFДокумент2 страницыSerie W11 PDFOrlandoОценок пока нет
- Crack Width Design - IS456-2000Документ1 страницаCrack Width Design - IS456-2000Nitesh SinghОценок пока нет
- Appraisal Assistant User ManualДокумент55 страницAppraisal Assistant User ManualDamian Padilla100% (3)
- Experiment No. 2 Rockwell Hardness Test IntroductionДокумент3 страницыExperiment No. 2 Rockwell Hardness Test IntroductionAhmad Abd100% (1)
- Practical Report Guideline EEE250Документ8 страницPractical Report Guideline EEE250MOHD ASYRAAF BIN SAIDINОценок пока нет
- Iot Lab RecordДокумент33 страницыIot Lab RecordMadhavan Jayarama MohanОценок пока нет