Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Rabbi Shneur Zalman of Liadi - Lessons in Tanya Vol-1Документ474 страницыRabbi Shneur Zalman of Liadi - Lessons in Tanya Vol-1Exequiel Medina83% (6)
- Autoridad Myles Munroe Poder de La El Proposito y PDF Autoridad Myles MunroeДокумент5 страницAutoridad Myles Munroe Poder de La El Proposito y PDF Autoridad Myles MunroeMaricarmen MorenoОценок пока нет
- Introduction To Wireless Communication - Radio CommunicationДокумент21 страницаIntroduction To Wireless Communication - Radio CommunicationYas773Оценок пока нет
- C27 and C32 Generator With EMCP4.2 Electrical SystemДокумент2 страницыC27 and C32 Generator With EMCP4.2 Electrical SystemAngel BernacheaОценок пока нет
- Theories & Models of LearningДокумент33 страницыTheories & Models of LearningAna Paulina Suárez CervantesОценок пока нет
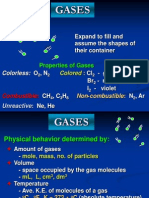
- Properties and Behavior of GasesДокумент34 страницыProperties and Behavior of GasesPaul Jeremiah Serrano NarvaezОценок пока нет
- D5092 - Design and Installation of Ground Water Monitoring Wells in AquifersДокумент14 страницD5092 - Design and Installation of Ground Water Monitoring Wells in Aquifersmaxuelbestete100% (1)
- Social AuditДокумент7 страницSocial AuditShofiq100% (2)
- Financial Modeling Interview Questions AnsweredДокумент6 страницFinancial Modeling Interview Questions AnsweredBHAVEN ASHOK SINGHОценок пока нет
- Adjectives For A Businessman 2023Документ2 страницыAdjectives For A Businessman 2023elyvuujavierОценок пока нет
- Dada and Buddhist Thought - Sung-Won Ko PDFДокумент24 страницыDada and Buddhist Thought - Sung-Won Ko PDFJuan Manuel Gomez GarcíaОценок пока нет
- Deepali Bhartiya: TCI Express Limited Gurgaon Assistant Manager Prateek Group Noida Senior ExecutiveДокумент3 страницыDeepali Bhartiya: TCI Express Limited Gurgaon Assistant Manager Prateek Group Noida Senior ExecutiveThe Cultural CommitteeОценок пока нет
- Right to Personal Liberty and Judicial Process in IndiaДокумент636 страницRight to Personal Liberty and Judicial Process in IndiaDrDiana PremОценок пока нет
- Justification: Justification: Doctrine of Council of TrentДокумент4 страницыJustification: Justification: Doctrine of Council of TrentMihai SarbuОценок пока нет
- Spiral Curve - Surveying and Transportation Engineering ReviewДокумент3 страницыSpiral Curve - Surveying and Transportation Engineering ReviewGphone100% (2)
- Entrepreneurship Starting and Operating A Small Business 4th Edition Mariotti Test Bank Full Chapter PDFДокумент33 страницыEntrepreneurship Starting and Operating A Small Business 4th Edition Mariotti Test Bank Full Chapter PDFmelrosecontrastbtjv1w100% (14)
- Academic StyleДокумент4 страницыAcademic StyleHa ToОценок пока нет
- Gram Negative Rods NonStool Pathogens FlowchartДокумент1 страницаGram Negative Rods NonStool Pathogens FlowchartKeithОценок пока нет
- Image/Data Encryption-Decryption Using Neural Network: Shweta R. Bhamare, Dr. S.D.SawarkarДокумент7 страницImage/Data Encryption-Decryption Using Neural Network: Shweta R. Bhamare, Dr. S.D.SawarkarPavan MasaniОценок пока нет
- The Photoconductive CellДокумент4 страницыThe Photoconductive Cellfasdasd123Оценок пока нет
- IT Department - JdsДокумент2 страницыIT Department - JdsShahid NadeemОценок пока нет
- Performance of Filler Material in GabionsДокумент4 страницыPerformance of Filler Material in GabionsPreetham N KumarОценок пока нет
- WHIRLPOOL AWE 2214 User ManualДокумент19 страницWHIRLPOOL AWE 2214 User ManualSilvestru NemorovОценок пока нет
- SPXДокумент6 страницSPXapi-3700460Оценок пока нет
- Brief History of Gifted and Talented EducationДокумент4 страницыBrief History of Gifted and Talented Educationapi-336040000Оценок пока нет
- 2015 StoneAge - LowresДокумент51 страница2015 StoneAge - LowresAZLAN ABDULLAIОценок пока нет
- The Biologic Width: - A Concept in Periodontics and Restorative DentistryДокумент8 страницThe Biologic Width: - A Concept in Periodontics and Restorative DentistryDrKrishna DasОценок пока нет
- Mr. Sanjeev Nanda - Devoted Son and GrandsonДокумент1 страницаMr. Sanjeev Nanda - Devoted Son and GrandsonSanjeev NandaОценок пока нет
- Vision CSP22 Abhyaas Test 3SДокумент44 страницыVision CSP22 Abhyaas Test 3SManasa DevarakondaОценок пока нет
- GHB FactsheetДокумент2 страницыGHB FactsheetABC Action NewsОценок пока нет