Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- 0806 3001 PDFДокумент9 страниц0806 3001 PDFBen Duncan Málaga EspichánОценок пока нет
- Filtros MRCДокумент25 страницFiltros MRCBen Duncan Málaga EspichánОценок пока нет
- Large Scale Synthesis of N-Doped Multi-Layered Graphene Sheets by Simple Arc-Discharge MethodДокумент5 страницLarge Scale Synthesis of N-Doped Multi-Layered Graphene Sheets by Simple Arc-Discharge MethodBen Duncan Málaga EspichánОценок пока нет
- Harry Fevold: Proteins BYДокумент66 страницHarry Fevold: Proteins BYBen Duncan Málaga EspichánОценок пока нет
- Surface Chemistry Involved in Epitaxy of Graphene On 3C-Sic (111) /siДокумент4 страницыSurface Chemistry Involved in Epitaxy of Graphene On 3C-Sic (111) /siBen Duncan Málaga EspichánОценок пока нет
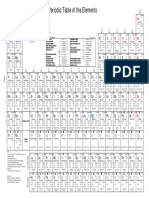
- Periodic Table of The Elements: Be B C LiДокумент1 страницаPeriodic Table of The Elements: Be B C LiBen Duncan Málaga EspichánОценок пока нет
- Wei 2017Документ15 страницWei 2017Ben Duncan Málaga EspichánОценок пока нет
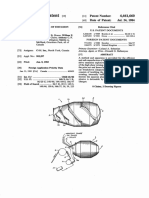
- United States Patent (19) : 11 Patent Number: 4,461,660 45) Date of Patent: Jul. 24, 1984Документ5 страницUnited States Patent (19) : 11 Patent Number: 4,461,660 45) Date of Patent: Jul. 24, 1984Ben Duncan Málaga EspichánОценок пока нет
- EPA FluorideДокумент8 страницEPA FluoridelaboratoriopcmОценок пока нет
- 5828 Fathy Abd Elhafez: Studies in Stereochemistry. Asymmetric Induction" The Syntheses Acyclic SystemsДокумент8 страниц5828 Fathy Abd Elhafez: Studies in Stereochemistry. Asymmetric Induction" The Syntheses Acyclic SystemsBen Duncan Málaga EspichánОценок пока нет
- Polk 2004Документ49 страницPolk 2004Ben Duncan Málaga EspichánОценок пока нет
- Evolutionary Mechanism of EukaryotesДокумент8 страницEvolutionary Mechanism of Eukaryoteswendy ArandaОценок пока нет
- Zhou 2018Документ10 страницZhou 2018Ben Duncan Málaga EspichánОценок пока нет
- Tissue and Cell: Sujune Tsai, Yating Jhuang, Emma Spikings, Ping-Jyun Sung, Chiahsin LinДокумент8 страницTissue and Cell: Sujune Tsai, Yating Jhuang, Emma Spikings, Ping-Jyun Sung, Chiahsin LinBen Duncan Málaga EspichánОценок пока нет
- Awad 2007Документ7 страницAwad 2007Ben Duncan Málaga EspichánОценок пока нет
- Reduccion Catalitica de Co2 en Electrodos de NanoparticulasДокумент6 страницReduccion Catalitica de Co2 en Electrodos de NanoparticulasBen Duncan Málaga EspichánОценок пока нет
- Engine Fuel Derived From Waste Plastics by Thermal TreatmentДокумент9 страницEngine Fuel Derived From Waste Plastics by Thermal TreatmentSiddharth SaxenaОценок пока нет
- Dengue-La Epidemiologia Del DengueДокумент8 страницDengue-La Epidemiologia Del DengueRaul KimОценок пока нет
- Parametric Study of Waste Chicken Fat Catalytic Chemical Vapour Deposition For Controlled Synthesis of Vertically Aligned Carbon NanotubesДокумент18 страницParametric Study of Waste Chicken Fat Catalytic Chemical Vapour Deposition For Controlled Synthesis of Vertically Aligned Carbon NanotubesBen Duncan Málaga EspichánОценок пока нет
- Graphene Based Electrode Materials For Microbial Fuel CellsДокумент14 страницGraphene Based Electrode Materials For Microbial Fuel CellsBen Duncan Málaga EspichánОценок пока нет
- Author's Accepted Manuscript: Ceramics InternationalДокумент25 страницAuthor's Accepted Manuscript: Ceramics InternationalBen Duncan Málaga EspichánОценок пока нет
- Enhanced Biological Nitrogen Removal Via Dissolved Oxygen Partitioning and Step Feeding in A Simulated River Bioreactor For Contaminated Source Water RemediationДокумент8 страницEnhanced Biological Nitrogen Removal Via Dissolved Oxygen Partitioning and Step Feeding in A Simulated River Bioreactor For Contaminated Source Water RemediationBen Duncan Málaga EspichánОценок пока нет
- Electrochemical Reduction of CO 2 at CuAu Nanoparticles: Size and Alloy EffectsДокумент7 страницElectrochemical Reduction of CO 2 at CuAu Nanoparticles: Size and Alloy EffectsBen Duncan Málaga EspichánОценок пока нет
- Dos Nuevas Clases de CopepodosДокумент14 страницDos Nuevas Clases de CopepodosBen Duncan Málaga EspichánОценок пока нет
- Latest Development in Viral Vectors For Gene TherapyДокумент6 страницLatest Development in Viral Vectors For Gene TherapyBen Duncan Málaga EspichánОценок пока нет
- Preparacion de Nanoparticulas de PaladioДокумент16 страницPreparacion de Nanoparticulas de PaladioBen Duncan Málaga EspichánОценок пока нет
- Pao Lesse 2003Документ6 страницPao Lesse 2003Ben Duncan Málaga EspichánОценок пока нет
- Analysis and Description of The Evolution of Alginate Immobilised Cells SystemsДокумент13 страницAnalysis and Description of The Evolution of Alginate Immobilised Cells SystemsBen Duncan Málaga EspichánОценок пока нет
- Magic Number and Quasi-Melting Temperature Discovered in Crystal Growth and Surface Phase TransitionsДокумент18 страницMagic Number and Quasi-Melting Temperature Discovered in Crystal Growth and Surface Phase TransitionsBen Duncan Málaga EspichánОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Clinical Avian Medicine - 2 Volume Set PDFДокумент1 057 страницClinical Avian Medicine - 2 Volume Set PDFSilvana Martinez100% (3)
- ResearchДокумент19 страницResearchKeVongPugehОценок пока нет
- Atlas 4 دائرة معارف طبية Reduced PDFДокумент316 страницAtlas 4 دائرة معارف طبية Reduced PDFMohammadSAL-RawashdehОценок пока нет
- Panic AttacksДокумент7 страницPanic Attacksapi-333422332Оценок пока нет
- Ano Rectal ExaminationДокумент12 страницAno Rectal ExaminationSnehal SinghОценок пока нет
- NCP AppendicitisДокумент8 страницNCP AppendicitisAaron_Kim_Vela_4636Оценок пока нет
- Health 8 Poster MakingДокумент9 страницHealth 8 Poster MakingDe Leon, Aaron MarcusОценок пока нет
- 17 - CIR V Philippine Health Care ProvidersДокумент2 страницы17 - CIR V Philippine Health Care ProvidersCamille AngelicaОценок пока нет
- Vertigo and Dizziness in The ElderlyДокумент6 страницVertigo and Dizziness in The ElderlyCarmen DélanoОценок пока нет
- Toxoigg ArcДокумент8 страницToxoigg Arctesteste testeОценок пока нет
- Pfizer Drug R&D Pipeline As of July 31, 2007Документ19 страницPfizer Drug R&D Pipeline As of July 31, 2007anon-843904100% (1)
- General Principles of Fracture ManagementДокумент60 страницGeneral Principles of Fracture ManagementAdrian Joel Quispe AlataОценок пока нет
- Conversion Disorder-1Документ11 страницConversion Disorder-1zainiОценок пока нет
- Sme Product Brochure PDFДокумент37 страницSme Product Brochure PDFNoor Azman YaacobОценок пока нет
- Jurnal Remifentanyl For Pain LaborДокумент11 страницJurnal Remifentanyl For Pain LaborAshadi CahyadiОценок пока нет
- Passenger/Traveler Details: Undertaking and Acknowledgement Form Related To COVID-19 Health MeasuresДокумент1 страницаPassenger/Traveler Details: Undertaking and Acknowledgement Form Related To COVID-19 Health MeasuresLabli BicОценок пока нет
- Insan Anatomisi Atlasi Mcminn 1515167549Документ18 страницInsan Anatomisi Atlasi Mcminn 1515167549Müslüm ŞahinОценок пока нет
- Zyrtec: Tablet Core: Tablet CoatingДокумент5 страницZyrtec: Tablet Core: Tablet CoatingDwi WirastomoОценок пока нет
- Jon Zonderman, Laurel, M.D. Shader Birth Control Pills Drugs The Straight FactsДокумент96 страницJon Zonderman, Laurel, M.D. Shader Birth Control Pills Drugs The Straight FactsPaola Felippi CoelhoОценок пока нет
- Drug Calculations For Nurses A Step-by-Step Approa... - (Chapter 8 Infusion Rate Calculations)Документ22 страницыDrug Calculations For Nurses A Step-by-Step Approa... - (Chapter 8 Infusion Rate Calculations)HarjotBrarОценок пока нет
- Evaluation of The Brief Adjustment Scale-6 (BASE-6) : A Measure of General Psychological Adjustment For Measurement-Based CareДокумент13 страницEvaluation of The Brief Adjustment Scale-6 (BASE-6) : A Measure of General Psychological Adjustment For Measurement-Based CareRowena Malabanan Maraquilla100% (1)
- TivaДокумент6 страницTivapaulina7escandar100% (1)
- 295 QsДокумент3 страницы295 Qsujangketul62Оценок пока нет
- Skyline Medical Trauma Center Site Visit ReportДокумент8 страницSkyline Medical Trauma Center Site Visit ReportUSA TODAY NetworkОценок пока нет
- Characterization of Renal Stones Using Gsi: Patient HistoryДокумент2 страницыCharacterization of Renal Stones Using Gsi: Patient HistoryAlreem AlhajryОценок пока нет
- Disseminated Intravascular Coagulation (DIC)Документ24 страницыDisseminated Intravascular Coagulation (DIC)Atiya HajjajОценок пока нет
- Atracurium BesylateДокумент3 страницыAtracurium BesylateAP TOROBXОценок пока нет
- You Are Dangerous To Your Health CRAWFORDДокумент18 страницYou Are Dangerous To Your Health CRAWFORDGonzalo PaezОценок пока нет
- Nausea and VomitingДокумент6 страницNausea and VomitingRavinderОценок пока нет