Вам также может понравиться
- Pharmacology for Student and Pupil Nurses and Students in Associated ProfessionsОт EverandPharmacology for Student and Pupil Nurses and Students in Associated ProfessionsОценок пока нет
- Drug Study AtorvastatinДокумент2 страницыDrug Study AtorvastatinReyes MarinellaОценок пока нет
- DRUG STUDY (Preeclampsia)Документ11 страницDRUG STUDY (Preeclampsia)Jobelle AcenaОценок пока нет
- Hipertensi UrgensiДокумент26 страницHipertensi UrgensidiegoОценок пока нет
- Tolleno Drug Study LONGДокумент9 страницTolleno Drug Study LONGHannah TollenoОценок пока нет
- Hypertensive Crises - Current ApproachДокумент35 страницHypertensive Crises - Current ApproachShre RanjithamОценок пока нет
- Haloperidol: College of Health SciencesДокумент2 страницыHaloperidol: College of Health SciencesKervy JuntillaОценок пока нет
- Medical - Surgical Nursing: College of Nursing - Phinma University of PangasinanДокумент2 страницыMedical - Surgical Nursing: College of Nursing - Phinma University of PangasinanRosalinda PerigoОценок пока нет
- Medsurg Careplan 3Документ12 страницMedsurg Careplan 3api-520841770Оценок пока нет
- AmlodipineДокумент2 страницыAmlodipineCj LowryОценок пока нет
- AmlodipineДокумент2 страницыAmlodipineVina Jane P Laurel92% (12)
- Patient & Family EducationДокумент3 страницыPatient & Family EducationJenjendeuk kimОценок пока нет
- (Per System Preferably) : AntihypertensiveДокумент4 страницы(Per System Preferably) : AntihypertensiveGwyn RosalesОценок пока нет
- Pre Eclampsia Drug StufyДокумент3 страницыPre Eclampsia Drug StufyFrances Reina TabaderoОценок пока нет
- Risperdone and Lithium CarbonateДокумент4 страницыRisperdone and Lithium CarbonateFionah RetuyaОценок пока нет
- Menpin Drug StudyPenthidineДокумент2 страницыMenpin Drug StudyPenthidineVine CastroОценок пока нет
- Drug StudyДокумент5 страницDrug StudyNhadzmae Asmadul IsnainОценок пока нет
- Drug StudyДокумент27 страницDrug StudyChan SorianoОценок пока нет
- Anaphylaxis: Emergency Department TreatmentДокумент14 страницAnaphylaxis: Emergency Department TreatmentTom BiusoОценок пока нет
- Amlo, Simvastatin, TamsulosinДокумент7 страницAmlo, Simvastatin, TamsulosinGwyn RosalesОценок пока нет
- DroperidolДокумент1 страницаDroperidolIvanne HisolerОценок пока нет
- Haloperidol DRUG STUDYДокумент2 страницыHaloperidol DRUG STUDYaaron tabernaОценок пока нет
- OB Care Plan: Assessment DataДокумент10 страницOB Care Plan: Assessment Dataapi-520858833Оценок пока нет
- Pharmacists Clinical Round Report: Faculty of Pharmacy & Alternative Medicine The Islamia University of BahawalpurДокумент9 страницPharmacists Clinical Round Report: Faculty of Pharmacy & Alternative Medicine The Islamia University of BahawalpurNoman ZakiОценок пока нет
- Conns Syndrome Gonzales NickaДокумент10 страницConns Syndrome Gonzales Nickamafeehney feehilyОценок пока нет
- QTC Flow Diagram With Medications Final Dec 17 A3 With LogosДокумент1 страницаQTC Flow Diagram With Medications Final Dec 17 A3 With LogosMelissa MurilloОценок пока нет
- DRUG STUDY-1st BatchДокумент27 страницDRUG STUDY-1st BatchCanny CańasОценок пока нет
- HypertensionДокумент18 страницHypertensionLeoОценок пока нет
- PropanolДокумент8 страницPropanolStacey CamilleОценок пока нет
- Drug Study Divine1Документ5 страницDrug Study Divine1Lhea Marie TrinidadОценок пока нет
- Drug Study MCL or TechДокумент7 страницDrug Study MCL or TechKyra Lalaine Angub CervantesОценок пока нет
- Synergy DrugДокумент4 страницыSynergy DrugUDDE-E MARISABELОценок пока нет
- Nursing Care Plan: Priority #1 Decreased Cardiac OutputДокумент2 страницыNursing Care Plan: Priority #1 Decreased Cardiac Output1S - LASTIMOSA ATHENA IRISH D.Оценок пока нет
- Drug DilantinДокумент1 страницаDrug DilantinSrkocherОценок пока нет
- Chronic Conditions Hospitalized PatientsДокумент10 страницChronic Conditions Hospitalized Patientsrezaferidooni00Оценок пока нет
- AdenosineДокумент2 страницыAdenosinegovind_soni_150% (1)
- Lab or Diagnostic Test Patient's Value Normal ValueДокумент9 страницLab or Diagnostic Test Patient's Value Normal ValueJormarie NogueОценок пока нет
- Pharmacologic Class: Therapeutic Class: Atypical: Dibenzothiazepine Derivative AntipsychoticДокумент2 страницыPharmacologic Class: Therapeutic Class: Atypical: Dibenzothiazepine Derivative AntipsychoticBianca Nicole Gacad Fernandez100% (1)
- Drug StudyДокумент1 страницаDrug StudyPRINCESS MARIZHAR OMARОценок пока нет
- Epo DrugstudyДокумент3 страницыEpo DrugstudyKhatlen BagaresОценок пока нет
- Angiotensin-Converting Enzyme (ACE)Документ5 страницAngiotensin-Converting Enzyme (ACE)Isabella SamsonОценок пока нет
- Injections: 2.5mg/ml in CNS: Drowsiness,: DroperidolДокумент3 страницыInjections: 2.5mg/ml in CNS: Drowsiness,: DroperidolthesarayoОценок пока нет
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmДокумент11 страницHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuОценок пока нет
- Drug Study...Документ6 страницDrug Study...Johanz PacrisОценок пока нет
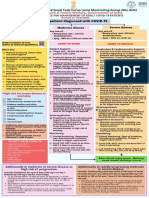
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaДокумент1 страницаAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845Оценок пока нет
- Metoprolol Drug StudyДокумент4 страницыMetoprolol Drug StudyCrisha Ann Billones BacutaОценок пока нет
- Careplan 2Документ10 страницCareplan 2api-520843051Оценок пока нет
- Drug StudyДокумент8 страницDrug StudySheryhan Tahir BayleОценок пока нет
- Anaphylaxis Emergency Department TreatmentДокумент14 страницAnaphylaxis Emergency Department Treatmentel.perjurio.onlineОценок пока нет
- DG2 KetorolacДокумент1 страницаDG2 KetorolacEkusu Yu ShunОценок пока нет
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaДокумент1 страницаAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaОценок пока нет
- Drug Study: Vomiting, GIДокумент5 страницDrug Study: Vomiting, GIJoyzelle CagandahanОценок пока нет
- EpinephrineДокумент4 страницыEpinephrinegovind_soni_15Оценок пока нет
- HPN Drug StudyДокумент4 страницыHPN Drug StudyJohn Haider Colorado GamolОценок пока нет
- Drug StudyДокумент2 страницыDrug Studyunkown userОценок пока нет
- AIIMS COVID Algorithm 1.5-1 PDFДокумент1 страницаAIIMS COVID Algorithm 1.5-1 PDFAnutosh BhaskarОценок пока нет
- Amlodipine Drug StudyДокумент2 страницыAmlodipine Drug StudyAbigail Basco100% (3)
- Name of Drug Dosage/ Frequency / Timing/ Route Mechanism of Action Indication Contraindic Ation Adverse Effect Nursing ResponsibilitiesДокумент3 страницыName of Drug Dosage/ Frequency / Timing/ Route Mechanism of Action Indication Contraindic Ation Adverse Effect Nursing ResponsibilitiesphoebeОценок пока нет
- Rogers2019 Article RiskOverdiagnosisAndEthicalJusДокумент18 страницRogers2019 Article RiskOverdiagnosisAndEthicalJusizzati94Оценок пока нет
- Antibiotic Cross-Sensitivity Chart PDFДокумент1 страницаAntibiotic Cross-Sensitivity Chart PDFanareadsОценок пока нет
- Evaluation and Treatment of Urinary Incontinence in WomenДокумент1 страницаEvaluation and Treatment of Urinary Incontinence in Womenizzati94Оценок пока нет
- DonotcrushДокумент16 страницDonotcrushapi-278913876Оценок пока нет
- Altered Mental StateДокумент2 страницыAltered Mental Stateizzati94Оценок пока нет
- 2012 Guía para El Manejo de HipotiroidismoДокумент36 страниц2012 Guía para El Manejo de Hipotiroidismomod_naiveОценок пока нет
- Suspected Stroke: Clinical Management Guideline ForДокумент1 страницаSuspected Stroke: Clinical Management Guideline Forizzati94Оценок пока нет
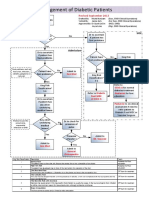
- Management of Diabetic Foot PatientsДокумент1 страницаManagement of Diabetic Foot Patientsizzati94Оценок пока нет
- EE1108 Exercise 2 AnswersДокумент8 страницEE1108 Exercise 2 Answersizzati94Оценок пока нет
- Appendix A: Review of Complex NumbersДокумент10 страницAppendix A: Review of Complex Numbersizzati94Оценок пока нет
- EggsДокумент1 страницаEggsizzati94Оценок пока нет
- URTI (Objectives and Readings)Документ1 страницаURTI (Objectives and Readings)izzati94Оценок пока нет
- EG1108 Handout 3-03 (Stored Energy in Capacitor)Документ1 страницаEG1108 Handout 3-03 (Stored Energy in Capacitor)izzati94Оценок пока нет
- Global AphasiaДокумент5 страницGlobal AphasiaMuhammad Agus NurОценок пока нет
- 10 1097@DSS 0000000000001281Документ11 страниц10 1097@DSS 0000000000001281plastic guardiansОценок пока нет
- Kinesio Tape Courses Presents: Fundamentals and Advanced Kinesio Taping (KT1 and KT2)Документ2 страницыKinesio Tape Courses Presents: Fundamentals and Advanced Kinesio Taping (KT1 and KT2)Mirelle_73Оценок пока нет
- Coding Handbook - Doc 6-16-09 Revised 8 14 09 AddДокумент52 страницыCoding Handbook - Doc 6-16-09 Revised 8 14 09 AddcindybevОценок пока нет
- Introduction of The ResearchДокумент3 страницыIntroduction of The Researchcristine baldazoОценок пока нет
- GRK Extrospection Excerpt PDFДокумент7 страницGRK Extrospection Excerpt PDFChrysoula GkaniОценок пока нет
- Gynae & Obstetrics Monitoring - IoMT - PhilipsДокумент10 страницGynae & Obstetrics Monitoring - IoMT - PhilipsAnuj MehrotraОценок пока нет
- Guidelines For APE 2021 With Drug Testing ROYCE HOTELДокумент3 страницыGuidelines For APE 2021 With Drug Testing ROYCE HOTELJm CayabyabОценок пока нет
- Answers For Ebn PicotДокумент7 страницAnswers For Ebn Picotapi-302499446Оценок пока нет
- Dance TherapyДокумент2 страницыDance TherapyXimena OrdonezОценок пока нет
- Indian Healthcare IndustryДокумент41 страницаIndian Healthcare Industrydmathur1234Оценок пока нет
- Thermal BurnsДокумент50 страницThermal BurnsPooya WindyОценок пока нет
- Article - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFДокумент32 страницыArticle - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFAnonymous g8zT2sPtjW100% (1)
- Blood Transfusion NotesДокумент1 страницаBlood Transfusion NotesShreyas WalvekarОценок пока нет
- Modified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2Документ9 страницModified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2indirinoor5Оценок пока нет
- Espondilolisis Revision 2010Документ9 страницEspondilolisis Revision 2010Giostin MosqueraОценок пока нет
- 1978 Caramazza Berndt PBДокумент21 страница1978 Caramazza Berndt PBEddiesvoiceОценок пока нет
- Mentored by Nature: Bradley L. JonesДокумент5 страницMentored by Nature: Bradley L. JonesAlfredo RamzОценок пока нет
- Medical Tourism in IndiaДокумент2 страницыMedical Tourism in IndiaDipak Rana0% (1)
- Post - Mortem CareДокумент15 страницPost - Mortem CareLoi Ocampo CrespoОценок пока нет
- Diagnostic TestsДокумент5 страницDiagnostic TestsAastha jainОценок пока нет
- PAEMS BLS Non-Transport Supply List: Peoria Area Ems System Prehospital Care ManualДокумент13 страницPAEMS BLS Non-Transport Supply List: Peoria Area Ems System Prehospital Care ManualnyfmedicОценок пока нет
- Bronchial Asthma SeminarДокумент64 страницыBronchial Asthma SeminarShidevОценок пока нет
- Course Specs Nurs104ly 2nd Semester 4th YearДокумент6 страницCourse Specs Nurs104ly 2nd Semester 4th YearEfren Plaza MolinaОценок пока нет
- Ozone Therapy in DentistryДокумент16 страницOzone Therapy in Dentistryshreya das100% (1)
- Associate Director of Pharmacovigilance in Newtown Square PA Resume Michael BlohДокумент6 страницAssociate Director of Pharmacovigilance in Newtown Square PA Resume Michael BlohMichaelBlohОценок пока нет
- Strides in IR: DR Vikram Shende. Mbbs (Gold Medalist), Md-Radiodiagnosis, Fvir-Kemh Mumbai, Foir-Hcg Bengaluru, Frcr-2AДокумент38 страницStrides in IR: DR Vikram Shende. Mbbs (Gold Medalist), Md-Radiodiagnosis, Fvir-Kemh Mumbai, Foir-Hcg Bengaluru, Frcr-2AShreyans KariaОценок пока нет
- Stress Management PPT FinalДокумент7 страницStress Management PPT FinalAdarsh Meher100% (1)
- Pediatric DosaPediatric Dosages Based On Body Weightges Based On Body WeightДокумент7 страницPediatric DosaPediatric Dosages Based On Body Weightges Based On Body WeightdjbhetaОценок пока нет
- Not GlaucomaДокумент5 страницNot GlaucomaFabio LuccheseОценок пока нет