Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Pharmacovigilance NotesДокумент73 страницыPharmacovigilance Notesvikram kushwaha100% (3)
- Critical Care Calculations Study GuideДокумент6 страницCritical Care Calculations Study GuideAja Blue100% (2)
- Traditional African MedicineДокумент13 страницTraditional African MedicineCarey G.100% (3)
- Abstract:: Estimation of Alfuzosin Hydrochloride by Uv-SpectrosДокумент2 страницыAbstract:: Estimation of Alfuzosin Hydrochloride by Uv-SpectrosLohith EaОценок пока нет
- The Procurement Qualification and Calibration of Lab InstrumentsДокумент7 страницThe Procurement Qualification and Calibration of Lab InstrumentsMowaten MasryОценок пока нет
- Formulation and Evaluation of Orodispersive Tablets of "Ebastine" Using Natural Super Disintegrant by Molecular Dispersion TechniqueДокумент13 страницFormulation and Evaluation of Orodispersive Tablets of "Ebastine" Using Natural Super Disintegrant by Molecular Dispersion TechniqueInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Buspirone Hydrochloride (Drug Study)Документ2 страницыBuspirone Hydrochloride (Drug Study)Franz.thenurse6888100% (1)
- Roscacea JournalДокумент5 страницRoscacea JournalanwarОценок пока нет
- List of Narciotic DrugsДокумент8 страницList of Narciotic DrugsNAVNEET BAGGAОценок пока нет
- Pharmaceutical Industry in India: Presented byДокумент56 страницPharmaceutical Industry in India: Presented byMukesh LalaОценок пока нет
- Catapres (Clonidine)Документ2 страницыCatapres (Clonidine)Adrianne BazoОценок пока нет
- ClopidogrelДокумент2 страницыClopidogrelapi-3797941100% (2)
- PhenobarbitalДокумент3 страницыPhenobarbitalChristine Joy Pepito50% (2)
- Lasa 1Документ4 страницыLasa 1hesti widayaniОценок пока нет
- Standard Operating Procedure Cold Chain ManagementДокумент3 страницыStandard Operating Procedure Cold Chain ManagementDaniel Yves IV Paez100% (1)
- Daunorubicin: Drug NameДокумент7 страницDaunorubicin: Drug NameEdgar Ledesma-MartínezОценок пока нет
- Lawsuit - Tennessee AG Sues Food City For Unlawful Sale of OpioidsДокумент209 страницLawsuit - Tennessee AG Sues Food City For Unlawful Sale of OpioidsDan LehrОценок пока нет
- A Simple and Validated RP-HPLC Method For The Estimation of Methylcobalamin in Bulk and Capsule Dosage FormДокумент4 страницыA Simple and Validated RP-HPLC Method For The Estimation of Methylcobalamin in Bulk and Capsule Dosage FormLayli AmaliaОценок пока нет
- Chapter 1 PPT 2 (Container and Closures)Документ15 страницChapter 1 PPT 2 (Container and Closures)Shumaila Qadir100% (2)
- Valvulas Diafragma Asepticas BPEДокумент104 страницыValvulas Diafragma Asepticas BPEHumberto GonzálezОценок пока нет
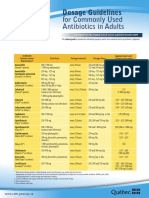
- CDM Antibio1 DosageGuidelines Adults enДокумент2 страницыCDM Antibio1 DosageGuidelines Adults endwiОценок пока нет
- Conffianz Announces New Board Member Albert DraaijerДокумент3 страницыConffianz Announces New Board Member Albert DraaijerPR.comОценок пока нет
- Heart Block and Their Best Treatment in Homeopathy - Bashir Mahmud ElliasДокумент13 страницHeart Block and Their Best Treatment in Homeopathy - Bashir Mahmud ElliasBashir Mahmud Ellias50% (2)
- Poster Upic4ir201986Документ1 страницаPoster Upic4ir201986Widayat WahyuОценок пока нет
- Cadila Pharmaceuticasls Limited: Sarvajanik College of Engineering & TechnologyДокумент15 страницCadila Pharmaceuticasls Limited: Sarvajanik College of Engineering & Technologypatel chintanОценок пока нет
- Pizer Practice QuestionДокумент2 страницыPizer Practice QuestionSmily IshaОценок пока нет
- Xylometazoline: A Tropical Nasal Decongestant and An Extensive Cause of Rhinitis Medicamentosa (RM)Документ5 страницXylometazoline: A Tropical Nasal Decongestant and An Extensive Cause of Rhinitis Medicamentosa (RM)Suci Triana PutriОценок пока нет
- Project About Clinical Drug Development: BY Bharatwajan M Student From Presidency College, ChennaiДокумент19 страницProject About Clinical Drug Development: BY Bharatwajan M Student From Presidency College, ChennaiDineshОценок пока нет
- Novartis 2012Документ284 страницыNovartis 2012Direct55Оценок пока нет
- Breast Cancer FinaleДокумент30 страницBreast Cancer Finaleخايزورا راهيمОценок пока нет