Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Efficacy and Safety of Exogenous Melatonin For Sec Sleep DisorderДокумент10 страницEfficacy and Safety of Exogenous Melatonin For Sec Sleep DisorderGera AguilarОценок пока нет
- Efficacy and Safety of Exogenous Melatonin For Sec Sleep DisorderДокумент10 страницEfficacy and Safety of Exogenous Melatonin For Sec Sleep DisorderGera AguilarОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Actualización Retinopatía DiabéticaДокумент13 страницActualización Retinopatía DiabéticaGera AguilarОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
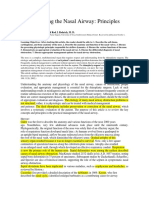
- Understanding The Nasal AirwayДокумент21 страницаUnderstanding The Nasal AirwayGera AguilarОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Schizophrenia PDFДокумент5 страницSchizophrenia PDFGera AguilarОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Mitochondrial Cytopathies in Children and AdultsДокумент28 страницMitochondrial Cytopathies in Children and AdultsmmaitehmdОценок пока нет
- Pre-Board Exam: September 2018Документ54 страницыPre-Board Exam: September 2018Jay Carlo Bagayas100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Willowbrook ExperimentsДокумент4 страницыThe Willowbrook ExperimentsVictoria AguilarОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Dhatupaushtik ChurnaДокумент6 страницDhatupaushtik ChurnaShoeb MirzaОценок пока нет
- 2018 Overview Digestive System HandoutДокумент11 страниц2018 Overview Digestive System HandoutdraganОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Classification and evolution of prokaryotic and eukaryotic cellsДокумент7 страницClassification and evolution of prokaryotic and eukaryotic cellsjodeoiraluis josonОценок пока нет
- Genetics of Mitochondrial Disease: Russell P. SanetoДокумент54 страницыGenetics of Mitochondrial Disease: Russell P. SanetoGréta BotyánszkiОценок пока нет
- Peritoneal DialysisДокумент9 страницPeritoneal Dialysispinkygurlz1990Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Alex Cox Death 911 Call TranscriptДокумент10 страницAlex Cox Death 911 Call Transcripttmiller696733% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Seminar On PRVNTV ObgДокумент43 страницыSeminar On PRVNTV Obgraghuram reddyОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- CRH Radiology Policies and ProceduresДокумент60 страницCRH Radiology Policies and ProceduresAbdul Saeed Shah100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Border Terrier Ukc StandardДокумент2 страницыBorder Terrier Ukc Standardapi-342444556Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Hypertensive Emergencies in The Emergency DepartmentДокумент13 страницHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesОценок пока нет
- Warehouse EssayДокумент8 страницWarehouse Essayafibojmbjifexj100% (2)
- First International congress on clinical Hypnosis & Related Sciences programДокумент91 страницаFirst International congress on clinical Hypnosis & Related Sciences programGolnaz BaghdadiОценок пока нет
- Module 2 - Community Health NursingДокумент9 страницModule 2 - Community Health NursingMarie Kelsey Acena Macaraig100% (1)
- Important Uses of Neem ExtractДокумент3 страницыImportant Uses of Neem ExtractAbdurrahman MustaphaОценок пока нет
- ZZZZZZZZZZZZZZДокумент8 страницZZZZZZZZZZZZZZchloramphenicolОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Kirit P. Mehta School of Law, Mumbai: A Project Submitted ONДокумент12 страницKirit P. Mehta School of Law, Mumbai: A Project Submitted ONNikit BaryaОценок пока нет
- Hipocrates - VOLUME 6Документ400 страницHipocrates - VOLUME 6Heitor Murillo CarnioОценок пока нет
- MidtermДокумент22 страницыMidtermEmvie Loyd Pagunsan-ItableОценок пока нет
- CDC's HIV Infection Through Oral Sex, Fact SheetДокумент2 страницыCDC's HIV Infection Through Oral Sex, Fact SheetCésar E. ConcepciónОценок пока нет
- Feasibility of Muntingia Calabura as WineДокумент19 страницFeasibility of Muntingia Calabura as WineKhen Raselle BaculioОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Routine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We SayДокумент6 страницRoutine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We Sayannisa edwarОценок пока нет
- Medication SafetyДокумент180 страницMedication SafetyAengus JoyceОценок пока нет
- Photosensitizing Agents and Their Applications in PhototherapyДокумент26 страницPhotosensitizing Agents and Their Applications in PhototherapyMagesh SОценок пока нет
- Yes, aside from the educational SMS intervention, the groups were treated equally as they both received routine trainingДокумент54 страницыYes, aside from the educational SMS intervention, the groups were treated equally as they both received routine trainingYogiОценок пока нет
- New Drugs 2014-2018Документ31 страницаNew Drugs 2014-2018Prem Goel0% (1)
- Case Analysis Tool (CAT) Worksheet: Student's NameДокумент7 страницCase Analysis Tool (CAT) Worksheet: Student's NameDina KristevaОценок пока нет
- ZoologyДокумент97 страницZoologyEnsОценок пока нет