Вам также может понравиться
- Introduction to Nursing Research Part 1: Significance and MethodologyДокумент22 страницыIntroduction to Nursing Research Part 1: Significance and MethodologyCiedelle Honey Lou DimaligОценок пока нет
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideОт EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuideОценок пока нет
- 3806NRS Nursing Assignment HelpДокумент5 страниц3806NRS Nursing Assignment HelpMarry WillsonОценок пока нет
- Ethical Dilemmas in Nursing PDFДокумент5 страницEthical Dilemmas in Nursing PDFtitiОценок пока нет
- Enabling Learning in Nursing and Midwifery Practice: A Guide for MentorsОт EverandEnabling Learning in Nursing and Midwifery Practice: A Guide for MentorsSue WestОценок пока нет
- Providing Culturally Appropriate Care: A Literature ReviewДокумент9 страницProviding Culturally Appropriate Care: A Literature ReviewLynette Pearce100% (1)
- The WHO Health Promotion Glossary PDFДокумент17 страницThe WHO Health Promotion Glossary PDFfirda FibrilaОценок пока нет
- Issue Analysis Paper Cultural Competence in Nursing ApplebachДокумент18 страницIssue Analysis Paper Cultural Competence in Nursing Applebachapi-283260051Оценок пока нет
- Management of Vacuum Assisted Closure TherapyДокумент14 страницManagement of Vacuum Assisted Closure TherapyVoiculescu MihaelaОценок пока нет
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideОт EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideОценок пока нет
- Concept Analysis VulnerabilityДокумент15 страницConcept Analysis Vulnerabilityapi-525425941Оценок пока нет
- Health Assessment Assignment 1 Nursing ProcessДокумент2 страницыHealth Assessment Assignment 1 Nursing ProcessDiana MuañaОценок пока нет
- The Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionОт EverandThe Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionОценок пока нет
- Writing for Publication in Nursing and Healthcare: Getting it RightОт EverandWriting for Publication in Nursing and Healthcare: Getting it RightОценок пока нет
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Vascular Responses to PathogensОт EverandVascular Responses to PathogensFelicity N.E. GavinsОценок пока нет
- CV BaranovaДокумент1 страницаCV Baranovaapi-252948975Оценок пока нет
- The Nurse Practitioner in UrologyОт EverandThe Nurse Practitioner in UrologyMichelle LajinessОценок пока нет
- Olivia Engle NP ResumeДокумент1 страницаOlivia Engle NP Resumeapi-654403621Оценок пока нет
- Strategies To Prevent Central Line Associated Bloodstream Infections in Acute Care Hospitals 2022 UpdateДокумент17 страницStrategies To Prevent Central Line Associated Bloodstream Infections in Acute Care Hospitals 2022 Updatealejandro montesОценок пока нет
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersОт EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersОценок пока нет
- ICN - APN Report - 2020Документ44 страницыICN - APN Report - 2020Daniela Silva100% (1)
- Morse Fall Scale AssessmentДокумент6 страницMorse Fall Scale AssessmentEka Febriani100% (1)
- Professional Accountability in NursingДокумент4 страницыProfessional Accountability in NursingJohn N MwangiОценок пока нет
- Medication Management - PaperДокумент12 страницMedication Management - PaperGinaОценок пока нет
- Collaborative Care Between Nurse Practitioners and Primary Care PhysiciansДокумент11 страницCollaborative Care Between Nurse Practitioners and Primary Care PhysiciansLeek AgoessОценок пока нет
- Pathophysiology 2Документ92 страницыPathophysiology 2Princess AgarwalОценок пока нет
- Problem-based Approach to Gastroenterology and HepatologyОт EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisОценок пока нет
- The COAT & Review Approach: How to recognise and manage unwell patientsОт EverandThe COAT & Review Approach: How to recognise and manage unwell patientsРейтинг: 5 из 5 звезд5/5 (1)
- History and Evolution of NursingДокумент45 страницHistory and Evolution of NursingStephany Zamoras100% (1)
- NMBA Case Studies Code of Conduct For Nurses and Code of Conduct For MidwivesДокумент7 страницNMBA Case Studies Code of Conduct For Nurses and Code of Conduct For Midwivestom doyleОценок пока нет
- Rheumatology Nursing: A Creative ApproachОт EverandRheumatology Nursing: A Creative ApproachJackie HillОценок пока нет
- Nursing 660 - PresentationДокумент12 страницNursing 660 - Presentationapi-282992446Оценок пока нет
- Nurse Practitioner Resume 1Документ2 страницыNurse Practitioner Resume 1api-596656815Оценок пока нет
- Nursing Process Paper: 72-Year-Old Male with Multiple Medical DiagnosesДокумент13 страницNursing Process Paper: 72-Year-Old Male with Multiple Medical Diagnoseshepina100% (1)
- NURSING CARE OF ADULTS II: Passbooks Study GuideОт EverandNURSING CARE OF ADULTS II: Passbooks Study GuideОценок пока нет
- Appendicitis: The Etiology, Hygenic and Dietetic TreatmentОт EverandAppendicitis: The Etiology, Hygenic and Dietetic TreatmentРейтинг: 3 из 5 звезд3/5 (2)
- Spirituality in Healthcare: Perspectives for Innovative PracticeОт EverandSpirituality in Healthcare: Perspectives for Innovative PracticeОценок пока нет
- Emergency Department Evaluation Back PainДокумент29 страницEmergency Department Evaluation Back PainRodolfo GorveñaОценок пока нет
- ABCDE Medical Student Session 10th May 2011Документ42 страницыABCDE Medical Student Session 10th May 2011gedepambudi0% (1)
- Ethical Decision MakingДокумент5 страницEthical Decision Makingapi-520453750100% (1)
- How Nurses Can Effectively Delegate TasksДокумент28 страницHow Nurses Can Effectively Delegate Tasksahmad rizalОценок пока нет
- Nursing Code of EthicsДокумент2 страницыNursing Code of EthicsClarissa HeatonОценок пока нет
- Running Head: QSEN 1Документ11 страницRunning Head: QSEN 1Mariam AbedОценок пока нет
- Rapid Response Team Whitepaper With Intro UPDATEDДокумент24 страницыRapid Response Team Whitepaper With Intro UPDATEDHari Mas KuncoroОценок пока нет
- Ethical Problems in Nursing ManagementДокумент4 страницыEthical Problems in Nursing ManagementJen Rhae LimОценок пока нет
- Module 1 REVIEW OF THE NURSING PROCESS 1Документ3 страницыModule 1 REVIEW OF THE NURSING PROCESS 1hamisi100% (2)
- PERITONITISДокумент27 страницPERITONITISTiffany Adrias100% (1)
- 1 s2.0 S0260691718301795 Main PDFДокумент5 страниц1 s2.0 S0260691718301795 Main PDFNovita SuryaОценок пока нет
- Analisis Faktor Risiko Glomerulonefritis Akut Pasca Streptokokus Pada Anak Di RSUP Prof. Dr. R. D. Kandou ManadoДокумент7 страницAnalisis Faktor Risiko Glomerulonefritis Akut Pasca Streptokokus Pada Anak Di RSUP Prof. Dr. R. D. Kandou ManadoLu Jordy LuhurОценок пока нет
- 438 1738 1 PBДокумент7 страниц438 1738 1 PBrahmat ramadaniОценок пока нет
- Adherence OATДокумент11 страницAdherence OATNovita SuryaОценок пока нет
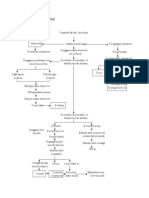
- Pathway GGKДокумент1 страницаPathway GGKNovita Surya100% (1)
- Komunikasi Keluarga Dalam Perkembangan Anak: Keywords: Family Communication, CДокумент128 страницKomunikasi Keluarga Dalam Perkembangan Anak: Keywords: Family Communication, CNovita SuryaОценок пока нет
- Pathways HepatitisДокумент2 страницыPathways HepatitisNovita SuryaОценок пока нет
- A2 Unit of WorkДокумент18 страницA2 Unit of Workapi-486612781Оценок пока нет
- Concept of EconomicsДокумент22 страницыConcept of EconomicsAnuska ThapaОценок пока нет
- Competing Risks and Multistate Models With RДокумент249 страницCompeting Risks and Multistate Models With RJuanCarlosAguilarCastro100% (1)
- DOO OBR Usage v3Документ73 страницыDOO OBR Usage v3Kirti ThakurОценок пока нет
- Munsat, S. - ProcessДокумент6 страницMunsat, S. - ProcessBen FortisОценок пока нет
- Standard Operation Procedures.06 - Potentially Hazardous Foods - Date MarkingДокумент3 страницыStandard Operation Procedures.06 - Potentially Hazardous Foods - Date MarkingJumadi SuburОценок пока нет
- VMware Virtual SANДокумент24 страницыVMware Virtual SANUjjwal LanjewarОценок пока нет
- SP Racing F3 FC Board(Deluxe) internal OSD Specification and SetupДокумент5 страницSP Racing F3 FC Board(Deluxe) internal OSD Specification and SetupibyselfОценок пока нет
- Centre For Political Studies: End-Semester Examination Time-Table Monsoon Semester 2019 ExaminationДокумент2 страницыCentre For Political Studies: End-Semester Examination Time-Table Monsoon Semester 2019 ExaminationAbhijeet JhaОценок пока нет
- Ap Art CrashcourseДокумент19 страницAp Art Crashcourseapi-298825724Оценок пока нет
- Aneka Cloud IntroductionДокумент36 страницAneka Cloud IntroductionPradeep Kumar Reddy ReddyОценок пока нет
- APMA 3100 Chapter 1-HandoutДокумент10 страницAPMA 3100 Chapter 1-HandoutMichael ChangОценок пока нет
- Action Research InsetДокумент2 страницыAction Research InsetKenОценок пока нет
- BoilerДокумент7 страницBoilerXie ShjОценок пока нет
- Spitler McQuiston Lindsey 93 2Документ11 страницSpitler McQuiston Lindsey 93 2Shafawati ShahneelОценок пока нет
- ASTM C 1260 Expansion LimitsДокумент12 страницASTM C 1260 Expansion Limitsheisin1865Оценок пока нет
- Inventor of 4G OFDM Technology Inspired by Dragon BallДокумент7 страницInventor of 4G OFDM Technology Inspired by Dragon BallTria RahmawatiОценок пока нет
- (Hawley) - The Practice of Silviculture (1946)Документ380 страниц(Hawley) - The Practice of Silviculture (1946)Karpincho30% (1)
- Integrating Information About The Cost of Carbon Through Activity Based Costing 2012 Journal of Cleaner ProductionДокумент10 страницIntegrating Information About The Cost of Carbon Through Activity Based Costing 2012 Journal of Cleaner ProductionLilian BrodescoОценок пока нет
- Indonesian Pangasius BrochureДокумент6 страницIndonesian Pangasius BrochurerobiyullahОценок пока нет
- Activity Rules - Calling A Sub-ActivityДокумент7 страницActivity Rules - Calling A Sub-Activityvineela05Оценок пока нет
- DBMS Lab - Practical FileДокумент21 страницаDBMS Lab - Practical Fileakhileshprasad1Оценок пока нет
- Kajo 5 PDFДокумент3 страницыKajo 5 PDFJonathan ChauОценок пока нет
- FY2010 DSM-IV-TR Summary: Division of Juvenile Justice State of Alaska, DHSSДокумент15 страницFY2010 DSM-IV-TR Summary: Division of Juvenile Justice State of Alaska, DHSSGnostic43Оценок пока нет
- Quality Concepts in DesignДокумент2 страницыQuality Concepts in DesignThulasi Raman KowsiganОценок пока нет
- Use of IT in ControllingДокумент19 страницUse of IT in ControllingSameer Sawant50% (2)
- Đề 1Документ9 страницĐề 1trung anОценок пока нет
- TheImpactofEmployeeEngagementonOrganizationsProductivity PDFДокумент10 страницTheImpactofEmployeeEngagementonOrganizationsProductivity PDFSapna SharmaОценок пока нет
- Chapter 07 4th Ed Gender&AgeДокумент18 страницChapter 07 4th Ed Gender&AgeCahaya Santi SianturiОценок пока нет
- Types of AssessmentДокумент7 страницTypes of AssessmentAisa karatuanОценок пока нет