Вам также может понравиться
- Problem-based Approach to Gastroenterology and HepatologyОт EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisОценок пока нет
- Blood Specimen Collection and ProcessingДокумент6 страницBlood Specimen Collection and ProcessingIzkandar RitzzneyОценок пока нет
- Blood CollectionДокумент25 страницBlood Collectionطاهرة حربية AlcaldeОценок пока нет
- Blood Collection Procedure (Venipuncture) 07Документ6 страницBlood Collection Procedure (Venipuncture) 07ridafОценок пока нет
- Immediate Care of NewbornДокумент4 страницыImmediate Care of NewbornjvjohnОценок пока нет
- NUR 204 2019 Inserting A Nasogastric TubeДокумент56 страницNUR 204 2019 Inserting A Nasogastric TubeHanan DaghashОценок пока нет
- Blood Sample Collection in ChildrenДокумент21 страницаBlood Sample Collection in Childrenvoruganty_vvs100% (3)
- Blood CollectionДокумент42 страницыBlood CollectionArslan Arshad100% (1)
- Blood TranfusionДокумент3 страницыBlood Tranfusionkeenoxky100% (1)
- Collection of SpecimenДокумент4 страницыCollection of SpecimenHamss AhmedОценок пока нет
- Chest Tube InsertionДокумент4 страницыChest Tube Insertionreiche100% (1)
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Документ13 страницSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanОценок пока нет
- Types of ImmunityДокумент35 страницTypes of ImmunityKailash NagarОценок пока нет
- Assisting With Dilatation and Curettage ProcedureДокумент3 страницыAssisting With Dilatation and Curettage ProceduremanjuОценок пока нет
- Vital Signs Written ReportДокумент7 страницVital Signs Written Reportkarl montanoОценок пока нет
- Health Assessment of Bronchial Asthma PatientДокумент3 страницыHealth Assessment of Bronchial Asthma PatientShetal SharmaОценок пока нет
- Assisting For Endotracheal IntubationДокумент16 страницAssisting For Endotracheal IntubationSREEDEVI T SURESH100% (1)
- NG Tube, Lavage and Gavage Procedure ChecklistДокумент6 страницNG Tube, Lavage and Gavage Procedure ChecklistBitew Tefera ZewudieОценок пока нет
- Related Protocols / Related Links Include:: Lumbar Puncture in The NeonateДокумент7 страницRelated Protocols / Related Links Include:: Lumbar Puncture in The NeonateJairo Camilo Guevara FaríasОценок пока нет
- OxygenationДокумент30 страницOxygenationmelanie silvaОценок пока нет
- Erythroblastosis FetalisДокумент5 страницErythroblastosis FetalisfitriarpsОценок пока нет
- Infant BathingДокумент3 страницыInfant BathingPaul Mark Pilar100% (1)
- Pediatric Checklist EditedДокумент72 страницыPediatric Checklist EditedJun Man100% (2)
- Specimen Collection and ProcessingДокумент19 страницSpecimen Collection and ProcessingFirman Setiawan Moehan100% (2)
- Abdominal Paracentesis, AP, Abdominal TapДокумент32 страницыAbdominal Paracentesis, AP, Abdominal TapMeraflor BahonsuaОценок пока нет
- Obgyn SL1Документ39 страницObgyn SL1mustafe omarОценок пока нет
- Umbilical Artery CatheterizationДокумент11 страницUmbilical Artery CatheterizationRhaq Sheldon-CoelhoОценок пока нет
- NCM - 103Документ5 страницNCM - 103Delma SimbahanОценок пока нет
- of Baby IncubatorДокумент12 страницof Baby IncubatorSubodh Gupta100% (3)
- Sputum CollectionДокумент5 страницSputum CollectionChejsalm AlvarezОценок пока нет
- Case Presentation Hepatitis A LuluДокумент28 страницCase Presentation Hepatitis A LuluBrenda KarinaОценок пока нет
- ABG Sampling (10-15 SOLANO) .OdtДокумент4 страницыABG Sampling (10-15 SOLANO) .OdtDeomicah SolanoОценок пока нет
- Nursing Care of The NBДокумент37 страницNursing Care of The NBJan Oliver YaresОценок пока нет
- Viral Hepatitis: Dr. Khaled JadallahДокумент24 страницыViral Hepatitis: Dr. Khaled JadallahRashed ShatnawiОценок пока нет
- Specimen Collection 2Документ70 страницSpecimen Collection 2Sakura Di Musim Semi100% (1)
- 'NicuДокумент12 страниц'NicuTopeshwar TpkОценок пока нет
- Central Venous Line CareДокумент13 страницCentral Venous Line CarePaul Henry RoxasОценок пока нет
- Phototherapy On The Postnatal WardДокумент5 страницPhototherapy On The Postnatal WardYwagar Ywagar100% (1)
- Phlebotomy - Lab Draws Final 09.17.2015Документ8 страницPhlebotomy - Lab Draws Final 09.17.2015ashanti wrightОценок пока нет
- Umbilical Artery CatheterizationДокумент9 страницUmbilical Artery CatheterizationrohitОценок пока нет
- Week 2 Electrolyte Imbalance Group Work INSTRUCTOR 1 PDFДокумент8 страницWeek 2 Electrolyte Imbalance Group Work INSTRUCTOR 1 PDFMaica LectanaОценок пока нет
- DehydrationДокумент14 страницDehydrationReimer LaquihuanacoОценок пока нет
- D.Y. Patil College of Nursing Kadamwadi, Kolhapur Subject: Child Health Nursing Case Presentation On Type 1 Diabetes MellitusДокумент18 страницD.Y. Patil College of Nursing Kadamwadi, Kolhapur Subject: Child Health Nursing Case Presentation On Type 1 Diabetes MellitusJuhi Johnson JadhavОценок пока нет
- Chest Tube InsertionДокумент2 страницыChest Tube InsertionmusicaBGОценок пока нет
- Oxygen AdministrationДокумент4 страницыOxygen Administrationss100% (1)
- LUMBERPUNCTURДокумент14 страницLUMBERPUNCTURRahul VasavaОценок пока нет
- Checklist For The VS Measurement (TPR and BP) A. Temperature A.1. Axillary Temperature (Digital Thermometer) Done Needs PracticeДокумент3 страницыChecklist For The VS Measurement (TPR and BP) A. Temperature A.1. Axillary Temperature (Digital Thermometer) Done Needs PracticeCyrillОценок пока нет
- Gloving and Degloving TechniqueДокумент23 страницыGloving and Degloving TechniqueRichard PidlaoanОценок пока нет
- Paediatric TracheostomyДокумент13 страницPaediatric TracheostomyYwagar YwagarОценок пока нет
- Cpms College of Nursing Procedure ON Performing An Intravenous InjectionДокумент5 страницCpms College of Nursing Procedure ON Performing An Intravenous InjectionAmy LalringhluaniОценок пока нет
- Newborn CareДокумент30 страницNewborn CareAlexandria P. OrcajadaОценок пока нет
- Pediatric DehydrationДокумент27 страницPediatric DehydrationAbraham ChiuОценок пока нет
- Blood Collection TubesДокумент1 страницаBlood Collection TubesMohammad Atiq100% (1)
- Lymphatic SystemДокумент5 страницLymphatic SystemCurex QAОценок пока нет
- Nasogastric Tube (Ryle)Документ1 страницаNasogastric Tube (Ryle)AAGKhatriОценок пока нет
- Abdominal AssessmentДокумент2 страницыAbdominal AssessmentJan Jamison ZuluetaОценок пока нет
- Immediate Newborn Care GuideДокумент8 страницImmediate Newborn Care GuideIsabelleОценок пока нет
- SalmonellaДокумент27 страницSalmonellaDayana PrasanthОценок пока нет
- PH Le BotomyДокумент27 страницPH Le BotomyAreesha ArifОценок пока нет
- Venipuncture Techniques:: MaterialsДокумент16 страницVenipuncture Techniques:: MaterialsNeal AllenОценок пока нет
- Skin Premalignant and TumorsДокумент95 страницSkin Premalignant and TumorsmedicoprakashОценок пока нет
- Hindu Marriage CertificateДокумент2 страницыHindu Marriage CertificatePankaj Batra80% (15)
- AnaemiaДокумент73 страницыAnaemiamedicoprakashОценок пока нет
- CSF AnalysisДокумент12 страницCSF AnalysismedicoprakashОценок пока нет
- HoningДокумент53 страницыHoningmedicoprakash89% (18)
- First Aid in Lab AccidentsДокумент2 страницыFirst Aid in Lab Accidentsmedicoprakash86% (7)
- Alternative ObligationsДокумент42 страницыAlternative ObligationsJanella Gail FerrerОценок пока нет
- Women and International Human Rights Law PDFДокумент67 страницWomen and International Human Rights Law PDFakilasriОценок пока нет
- Logiq e r7 SMДокумент435 страницLogiq e r7 SMAroОценок пока нет
- B737-800 Air ConditioningДокумент7 страницB737-800 Air ConditioningReynaldoОценок пока нет
- Dermatology Mini-OSCEДокумент322 страницыDermatology Mini-OSCEMarrkОценок пока нет
- Material Rate PWD 2014...........Документ70 страницMaterial Rate PWD 2014...........Shamsul IslamОценок пока нет
- NT PotentialMiningDevelopmentsДокумент13 страницNT PotentialMiningDevelopmentsho100hoОценок пока нет
- PMEGP Revised Projects (Mfg. & Service) Vol 1Документ260 страницPMEGP Revised Projects (Mfg. & Service) Vol 1Santosh BasnetОценок пока нет
- Planificare Săptămânală - Clasa A II-a (Fairyland 2)Документ6 страницPlanificare Săptămânală - Clasa A II-a (Fairyland 2)Oxy Oxy100% (1)
- Foundation Engineering. 02 Soil CompressibilityДокумент63 страницыFoundation Engineering. 02 Soil Compressibilitysammy lopezОценок пока нет
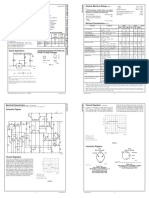
- LM 337Документ4 страницыLM 337matias robertОценок пока нет
- Sithpat006ccc019 A - 2021.1Документ34 страницыSithpat006ccc019 A - 2021.1Mark Andrew Clarete100% (2)
- 2008 03 20 BДокумент8 страниц2008 03 20 BSouthern Maryland OnlineОценок пока нет
- BDC 6566Документ6 страницBDC 6566jack.simpson.changОценок пока нет
- Medical Nutrition Therapy For DiabetesДокумент27 страницMedical Nutrition Therapy For Diabetesdr.Uci BaharОценок пока нет
- Exam Questions: Exam Title: Chapter MEK 8Документ4 страницыExam Questions: Exam Title: Chapter MEK 8vishnu sharmaОценок пока нет
- Recommended Practice For Corrosion Management of Pipelines in Oil & Gas Production and TransportationДокумент123 страницыRecommended Practice For Corrosion Management of Pipelines in Oil & Gas Production and Transportationsaifoa100% (2)
- RCMaДокумент18 страницRCMaAnonymous ffje1rpaОценок пока нет
- Starbucks Reconciliation Template & Instructions v20231 - tcm137-84960Документ3 страницыStarbucks Reconciliation Template & Instructions v20231 - tcm137-84960spaljeni1411Оценок пока нет
- FiltrationДокумент22 страницыFiltrationYeabsira WorkagegnehuОценок пока нет
- NASA ISS Expedition 2 Press KitДокумент27 страницNASA ISS Expedition 2 Press KitOrion2015Оценок пока нет
- Study of Behavior of Bacterial ConcreteДокумент20 страницStudy of Behavior of Bacterial ConcreteGodwin KopelliОценок пока нет
- 1 PolarographyДокумент20 страниц1 PolarographyRiya Das100% (1)
- Injection Analyzer Electronic Unit enДокумент67 страницInjection Analyzer Electronic Unit enmayralizbethbustosОценок пока нет
- Class 7 Work Book Answers Acid Bases and SaltsДокумент2 страницыClass 7 Work Book Answers Acid Bases and SaltsGaurav SethiОценок пока нет
- We Find The Way: Shipping InstructionsДокумент10 страницWe Find The Way: Shipping InstructionsLuke WangОценок пока нет
- Learning Activity Sheet MAPEH 10 (P.E.) : First Quarter/Week 1Документ4 страницыLearning Activity Sheet MAPEH 10 (P.E.) : First Quarter/Week 1Catherine DubalОценок пока нет
- ATR4518R6v07: Antenna SpecificationsДокумент2 страницыATR4518R6v07: Antenna Specificationsanna.bОценок пока нет
- 03 Secondary School Student's Academic Performance Self Esteem and School Environment An Empirical Assessment From NigeriaДокумент10 страниц03 Secondary School Student's Academic Performance Self Esteem and School Environment An Empirical Assessment From NigeriaKienstel GigantoОценок пока нет
- ESR 2538 ChemofastДокумент14 страницESR 2538 ChemofastEduardo Antonio Duran SepulvedaОценок пока нет