Вам также может понравиться
- Ranula Management: Suggested Modifications in The Micro-Marsupialization TechniqueДокумент3 страницыRanula Management: Suggested Modifications in The Micro-Marsupialization Techniquemehak malhotraОценок пока нет
- Management Surgery of The Oral and Maxillofacial Patient With End-Stage Renal DiseaseДокумент6 страницManagement Surgery of The Oral and Maxillofacial Patient With End-Stage Renal Diseasemehak malhotraОценок пока нет
- Letter To The Editor: Int. J. Oral Maxillofac. Surg. 2018 XXX: XXX-XXXДокумент2 страницыLetter To The Editor: Int. J. Oral Maxillofac. Surg. 2018 XXX: XXX-XXXmehak malhotraОценок пока нет
- Surgical Options in Oroantral Fistula Management: A Narrative ReviewДокумент13 страницSurgical Options in Oroantral Fistula Management: A Narrative Reviewmehak malhotraОценок пока нет
- Meniscopexy For Internal Derangement of Temporomandibular JointДокумент5 страницMeniscopexy For Internal Derangement of Temporomandibular Jointmehak malhotraОценок пока нет
- Comparative Evaluation of Various Miniplate Systems For The Repair of Mandibular Corpus FracturesДокумент5 страницComparative Evaluation of Various Miniplate Systems For The Repair of Mandibular Corpus Fracturesmehak malhotraОценок пока нет
- Controversiesin Dentoalveolarand Preprostheticsurgery: Deepak G. KrishnanДокумент8 страницControversiesin Dentoalveolarand Preprostheticsurgery: Deepak G. Krishnanmehak malhotraОценок пока нет
- 10 1016@j Coms 2018 06 003 PDFДокумент10 страниц10 1016@j Coms 2018 06 003 PDFmehak malhotraОценок пока нет
- Commentary: Distraction Osteogenesis Versus Orthognathic SurgeryДокумент3 страницыCommentary: Distraction Osteogenesis Versus Orthognathic Surgerymehak malhotraОценок пока нет
- Guidelines For Single-Stage Correction of TMJ Ankylosis, Facial Asymmetry and OSA in AdultsДокумент9 страницGuidelines For Single-Stage Correction of TMJ Ankylosis, Facial Asymmetry and OSA in Adultsmehak malhotraОценок пока нет
- Ranula Decompression Using Stitch and Stab Method: The Aluko TechniqueДокумент5 страницRanula Decompression Using Stitch and Stab Method: The Aluko Techniquemehak malhotraОценок пока нет
- New Protocol To Prevent TMJ Reankylosis and Potentially Life Threatening Complications in Triad PatientsДокумент6 страницNew Protocol To Prevent TMJ Reankylosis and Potentially Life Threatening Complications in Triad Patientsmehak malhotraОценок пока нет
- Al Moraissi2016Документ32 страницыAl Moraissi2016mehak malhotraОценок пока нет
- Pernambuco Index: Predictability of The Complexity of Surgery For Impacted Lower Third MolarsДокумент7 страницPernambuco Index: Predictability of The Complexity of Surgery For Impacted Lower Third Molarsmehak malhotraОценок пока нет
- Maxillomandibular Advancement: The Canadian ExperienceДокумент6 страницMaxillomandibular Advancement: The Canadian Experiencemehak malhotraОценок пока нет
- Kumari 2017Документ34 страницыKumari 2017mehak malhotraОценок пока нет
- 10 1016@j Cxom 2018 11 006Документ10 страниц10 1016@j Cxom 2018 11 006mehak malhotraОценок пока нет
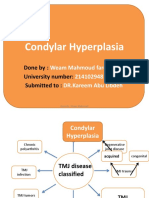
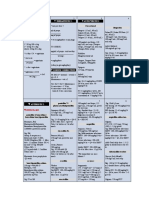
- Condylar Hyperplasia: Done By: University Number: Submitted ToДокумент69 страницCondylar Hyperplasia: Done By: University Number: Submitted Tomehak malhotraОценок пока нет
- What Is Suturing?: - The Primary Objective Is To Position andДокумент16 страницWhat Is Suturing?: - The Primary Objective Is To Position andmehak malhotraОценок пока нет
- Abdulmajeed Al Mogbel : Teaching Assistant, College of Dentistry, Qassim UniversityДокумент75 страницAbdulmajeed Al Mogbel : Teaching Assistant, College of Dentistry, Qassim Universitymehak malhotraОценок пока нет
- Pillai2016 PDFДокумент35 страницPillai2016 PDFmehak malhotraОценок пока нет
- The Use of The Buccal Fat Pad Flap For Oral Reconstruction: Review Open AccessДокумент9 страницThe Use of The Buccal Fat Pad Flap For Oral Reconstruction: Review Open Accessmehak malhotraОценок пока нет
- Maxillofacial Prosthetics Part-1 A Revie PDFДокумент10 страницMaxillofacial Prosthetics Part-1 A Revie PDFmehak malhotraОценок пока нет
- Injectableagentsversus Surgeryforrecurrent Temporomandibularjoint DislocationДокумент7 страницInjectableagentsversus Surgeryforrecurrent Temporomandibularjoint Dislocationmehak malhotraОценок пока нет
- Fibrinogen - A Practical and Cost Efficient BiomarДокумент6 страницFibrinogen - A Practical and Cost Efficient Biomarmehak malhotraОценок пока нет
- Malamed Local Anesthesia - 1Документ100 страницMalamed Local Anesthesia - 1Ines delacroix33% (3)
- Management of HIVHepatitis Patients in Oral and Maxillofacial SurgeryДокумент6 страницManagement of HIVHepatitis Patients in Oral and Maxillofacial Surgerymehak malhotraОценок пока нет
- Aramentarium For Minor Oral Surgical Procedure: Deepthi P.R. Intern Dept. of Oral SurgeryДокумент80 страницAramentarium For Minor Oral Surgical Procedure: Deepthi P.R. Intern Dept. of Oral Surgerymehak malhotraОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Jurnal Reading OsteomyelitisДокумент11 страницJurnal Reading Osteomyelitisfidela_ffОценок пока нет
- Synthesis of Silver Nanoparticles Using Probiotic BacteriaДокумент9 страницSynthesis of Silver Nanoparticles Using Probiotic BacteriaDr R.NithyaОценок пока нет
- BACTERIOCIN in Hurdle TechnologyДокумент31 страницаBACTERIOCIN in Hurdle TechnologyAjidhaslin Dhass0% (1)
- Drug StudyДокумент5 страницDrug StudyLara GatbontonОценок пока нет
- Antimicrobial Activity and Phytochemicalanalysis of CitrusДокумент8 страницAntimicrobial Activity and Phytochemicalanalysis of CitrusJasdeep KaurОценок пока нет
- Salinan Dari Jadwal KF Kedung CowekДокумент47 страницSalinan Dari Jadwal KF Kedung Cowekdwikamaliyatissholehah94Оценок пока нет
- Antimicrobial Activity of Carica Papaya (Pawpaw Leaf) On Some PatДокумент13 страницAntimicrobial Activity of Carica Papaya (Pawpaw Leaf) On Some PatMargaretha RennyОценок пока нет
- NCM 106 AntibacterialДокумент11 страницNCM 106 AntibacterialBruno, Kurt Andrei V.Оценок пока нет
- Pharmacology - Antibiotics - Cell Wall & Membrane Inhibit...Документ2 страницыPharmacology - Antibiotics - Cell Wall & Membrane Inhibit...Saurabh Singh RajputОценок пока нет
- Ampicillin Sodium - Sulbactam Sodium Drug StudyДокумент1 страницаAmpicillin Sodium - Sulbactam Sodium Drug StudyMelissa Marie Custodio100% (3)
- Chapter 22 The Organic Chemistry of Drugs: Discovery and DesignДокумент18 страницChapter 22 The Organic Chemistry of Drugs: Discovery and Designtyron9520Оценок пока нет
- Hidradenitis SuppurativaДокумент12 страницHidradenitis SuppurativamikezОценок пока нет
- Propolis - The Natural Antibiotic For MRSA, Candida, and MoreДокумент2 страницыPropolis - The Natural Antibiotic For MRSA, Candida, and MoreTheVitaminStore.com100% (1)
- Perencanaan Pembelian Obat Dan BHPДокумент11 страницPerencanaan Pembelian Obat Dan BHPmayarita dilucaselОценок пока нет
- Synthesis of ComplexesДокумент15 страницSynthesis of Complexes77chimОценок пока нет
- Microbial Keratitis Royal College of OphthalmologistДокумент2 страницыMicrobial Keratitis Royal College of OphthalmologistmahadianОценок пока нет
- Aus Pi TargocidДокумент5 страницAus Pi TargocidAsto Ata InteristiОценок пока нет
- Major Antibiotics With Their Microbial SourcesДокумент1 страницаMajor Antibiotics With Their Microbial SourcesSHRIKANTОценок пока нет
- Burkholderia CepaciaДокумент11 страницBurkholderia Cepaciaportner6873Оценок пока нет
- HD MicrobaДокумент5 страницHD MicrobaDian ApriantoОценок пока нет
- DSP 16 - 08 - 23Документ34 страницыDSP 16 - 08 - 23Iffa FelasyifaОценок пока нет
- Ivf: Therapeutics: Anti-Pyretics: PenicillinsДокумент6 страницIvf: Therapeutics: Anti-Pyretics: PenicillinsJenny CiОценок пока нет
- Daftar Obat Antibiotik Yang Tersedia Di Rsia Khalishah Palimanan NO Nama Obat Satuan NO Nama ObatДокумент4 страницыDaftar Obat Antibiotik Yang Tersedia Di Rsia Khalishah Palimanan NO Nama Obat Satuan NO Nama ObatsilviaОценок пока нет
- Delvotest Antibiotic Test BrochureДокумент2 страницыDelvotest Antibiotic Test BrochureDavidОценок пока нет
- Form Stock ObatДокумент7 страницForm Stock ObatSyarifahUniqueОценок пока нет
- Microbiology, Infections, and Antibiotic Therapy: Elizabeth J. Rosen, MD Francis B. Quinn, MD March 22, 2000Документ86 страницMicrobiology, Infections, and Antibiotic Therapy: Elizabeth J. Rosen, MD Francis B. Quinn, MD March 22, 2000skmvicky1483Оценок пока нет
- Generic Menu CardДокумент7 страницGeneric Menu CardDee BelarminoОценок пока нет
- UTD FosfomycinДокумент5 страницUTD FosfomycinfededelveliОценок пока нет
- B.Sc. TY Biotechnology PDFДокумент26 страницB.Sc. TY Biotechnology PDFHanumant Suryawanshi0% (1)
- Pharmacological and Biological Activities of Mirabilis Jalapa LДокумент9 страницPharmacological and Biological Activities of Mirabilis Jalapa Linggrianti wiratamaОценок пока нет