Академический Документы
Профессиональный Документы
Культура Документы
Jama PDF
Загружено:
maria isabelОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Jama PDF
Загружено:
maria isabelАвторское право:
Доступные форматы
Clinical Review & Education
JAMA Surgery | Special Communication
Centers for Disease Control and Prevention Guideline
for the Prevention of Surgical Site Infection, 2017
Sandra I. Berríos-Torres, MD; Craig A. Umscheid, MD, MSCE; Dale W. Bratzler, DO, MPH; Brian Leas, MA, MS;
Erin C. Stone, MA; Rachel R. Kelz, MD, MSCE; Caroline E. Reinke, MD, MSHP; Sherry Morgan, RN, MLS, PhD;
Joseph S. Solomkin, MD; John E. Mazuski, MD, PhD; E. Patchen Dellinger, MD; Kamal M. F. Itani, MD;
Elie F. Berbari, MD; John Segreti, MD; Javad Parvizi, MD; Joan Blanchard, MSS, BSN, RN, CNOR, CIC;
George Allen, PhD, CIC, CNOR; Jan A. J. W. Kluytmans, MD; Rodney Donlan, PhD; William P. Schecter, MD;
for the Healthcare Infection Control Practices Advisory Committee
Invited Commentary page 791
IMPORTANCE The human and financial costs of treating surgical site infections (SSIs) are Supplemental content
increasing. The number of surgical procedures performed in the United States continues to
rise, and surgical patients are initially seen with increasingly complex comorbidities. It is CME Quiz at
jamanetwork.com/learning
estimated that approximately half of SSIs are deemed preventable using evidence-based
strategies.
OBJECTIVE To provide new and updated evidence-based recommendations for the
prevention of SSI.
EVIDENCE REVIEW A targeted systematic review of the literature was conducted in MEDLINE,
EMBASE, CINAHL, and the Cochrane Library from 1998 through April 2014. A modified
Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach
was used to assess the quality of evidence and the strength of the resulting recommendation
and to provide explicit links between them. Of 5759 titles and abstracts screened, 896
underwent full-text review by 2 independent reviewers. After exclusions, 170 studies were
extracted into evidence tables, appraised, and synthesized.
FINDINGS Before surgery, patients should shower or bathe (full body) with soap
(antimicrobial or nonantimicrobial) or an antiseptic agent on at least the night before the
operative day. Antimicrobial prophylaxis should be administered only when indicated based
on published clinical practice guidelines and timed such that a bactericidal concentration of
the agents is established in the serum and tissues when the incision is made. In cesarean
section procedures, antimicrobial prophylaxis should be administered before skin incision.
Skin preparation in the operating room should be performed using an alcohol-based agent
unless contraindicated. For clean and clean-contaminated procedures, additional
prophylactic antimicrobial agent doses should not be administered after the surgical incision
is closed in the operating room, even in the presence of a drain. Topical antimicrobial agents
should not be applied to the surgical incision. During surgery, glycemic control should be
implemented using blood glucose target levels less than 200 mg/dL, and normothermia
should be maintained in all patients. Increased fraction of inspired oxygen should be
administered during surgery and after extubation in the immediate postoperative period for
patients with normal pulmonary function undergoing general anesthesia with endotracheal
intubation. Transfusion of blood products should not be withheld from surgical patients as a
means to prevent SSI. Author Affiliations: Author
affiliations are listed at the end of this
article.
CONCLUSIONS AND RELEVANCE This guideline is intended to provide new and updated
Group Information: The Healthcare
evidence-based recommendations for the prevention of SSI and should be incorporated into
Infection Control Practices Advisory
comprehensive surgical quality improvement programs to improve patient safety. Committee members are listed at the
end of this article.
Corresponding Author: Erin C.
Stone, MA, Division of Healthcare
Quality Promotion, Centers for
Disease Control and Prevention,
1660 Clifton Rd NE, Mail Stop A07
JAMA Surg. 2017;152(8):784-791. doi:10.1001/jamasurg.2017.0904 Atlanta, GA 30329
Published online May 3, 2017. Corrected on June 21, 2017. (ecstone@cdc.gov).
784 (Reprinted) jamasurgery.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
CDC Guideline for the Prevention of Surgical Site Infection, 2017 Special Communication Clinical Review & Education
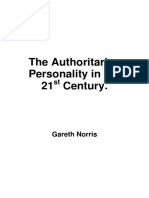
Figure. Results of the Study Selection Process
5487 Potentially relevant studies 104 Studies suggested by content 168 Studies cited in 1999 CDC
identified in literature searches experts SSI guideline
5759 Titles and abstracts screened
4863 Studies excluded
896 Full-text review
26 Clinical practice guidelines 719 Studies excluded
592 Not relevant to key questions
117 Study design
19 Additional clinical practice guidelines 6 Not available as full-text article
identified by writing group 4 Not in English
17 Clinical practice guidelines excluded
28 Clinical practice guidelines 44 RCTs identified from excluded SRs
cited in present guideline
25 Studies excluded, not relevant
to key questions
170 Studies extracted into evidence
and GRADE tables
CDC indicates Centers for Disease Control and Prevention; GRADE, Grading of Recommendations, Assessment, Development, and Evaluation; RCTs, randomized
controlled trials; SRs, systematic reviews; and SSI, surgical site infection.
S
urgical site infections (SSIs) are infections of the incision or This guideline’s recommendations were developed based on a
organ or space that occur after surgery.1 Surgical patients ini- targeted systematic review of the best available evidence on SSI pre-
tially seen with more complex comorbidities2 and the emer- vention conducted in MEDLINE, EMBASE, CINAHL, and the Coch-
gence of antimicrobial-resistant pathogens increase the cost and rane Library from 1998 through April 2014. To provide explicit links
challenge of treating SSIs.3-5 The prevention of SSI is increasingly im- between the evidence and recommendations, a modified Grading
portant as the number of surgical procedures performed in the of Recommendations, Assessment, Development, and Evaluation
United States continues to rise.6,7 Public reporting of process, out- (GRADE) approach was used for evaluating the quality of evidence
come, and other quality improvement measures is now required,8,9 and determining the strength of recommendations.12-15 The meth-
and reimbursements10 for treating SSIs are being reduced or de- ods and structure of this guideline were adopted in 2009 by CDC
nied. It has been estimated that approximately half of SSIs are pre- and HICPAC.16,17 The present guideline does not reevaluate several
ventable by application of evidence-based strategies.11 strong recommendations offered by CDC’s 1999 Guideline for Pre-
vention of Surgical Site Infection18 that are now considered to be ac-
cepted practice for the prevention of SSI. These recommendations
are found in eAppendix 1 of the Supplement. A detailed description
Methods
of the Guideline Questions, Scope and Purpose, and Methods, as well
This guideline focuses on select areas for the prevention of SSI as the Evidence Summaries supporting the evidence-based recom-
deemed important to undergo evidence assessment for the ad- mendations, can also be found in eAppendix 1 of the Supplement.
vancement of the field. These areas of focus were informed by feed- The detailed literature search strategies, GRADE Tables, and Evi-
back received from clinical experts and input from the Healthcare dence Tables supporting each section can be found in eAppendix 2
Infection Control Practices Advisory Committee (HICPAC), a fed- of the Supplement. Results of the entire study selection process are
eral advisory committee to the Centers for Disease Control and Pre- shown in the Figure. Of 5759 titles and abstracts screened, 896 un-
vention (CDC). This guideline was a systematic review of the litera- derwent full-text review by 2 independent reviewers. Full-text ar-
ture. No institutional review board approval or participant informed ticles were excluded if: 1) SSI was not reported as an outcome; 2) all
consent was necessary. patients included had “dirty” surgical procedures (except for Q2
jamasurgery.com (Reprinted) JAMA Surgery August 2017 Volume 152, Number 8 785
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
Clinical Review & Education Special Communication CDC Guideline for the Prevention of Surgical Site Infection, 2017
addressing the use of aqueous iodophor irrigation); 3) the study only 2005 US dollars to $25 546 in 2002 US dollars per infection.3-5,11
included oral or dental health procedures; 4) the surgical proce- Costs can exceed $90 000 per infection when the SSI involves a
dures did not include primary closure of the incision in the operat- prosthetic joint implant 21,22 or an antimicrobial-resistant
ing room (eg, orthopedic pin sites, thoracotomies, or percutane- organism.23 The Core Section of this guideline (eAppendix 1 of the
ous endoscopic gastrostomy [PEG] procedures, or wounds healing Supplement) includes recommendations for the prevention of SSI
by secondary intention); or 5) the study evaluated wound protec- that are generalizable across surgical procedures, with some
tors used postincision. Evidence-based recommendations in this exceptions as mentioned below.
guideline were cross-checked with those from other guidelines iden-
tified in a systematic search. Parenteral Antimicrobial Prophylaxis
CDC completed a draft of the guideline and shared it with the
expert panel for in-depth review and then with HICPAC and mem- 1A.1. Administer preoperative antimicrobial agents only when indi-
bers of the public at committee meetings (June 2010 to July cated based on published clinical practice guidelines and timed such
2015). CDC posted notice in the Federal Register for the following that a bactericidal concentration of the agents is established in the
2 periods of public comment: from January 29 to February 28, serum and tissues when the incision is made. (Category IB–strong
2014, and from April 8 to May 8, 2014. Comments were aggre- recommendation; accepted practice.)
gated and reviewed with the writing group and at another 1A.2. No further refinement of timing can be made for preoperative
HICPAC meeting. Based on the comments received, the literature antimicrobialagentsbasedonclinicaloutcomes.(Norecommendation/
search was updated, and new data were incorporated into a unresolved issue.)
revised draft. Further input was provided by HICPAC during a 1B. Administer the appropriate parenteral prophylactic antimicro-
public teleconference in May 2015. Final HICPAC input was pro- bial agents before skin incision in all cesarean section procedures.
vided via a vote by majority rule in July 2015. After final HICPAC (Category IA–strong recommendation; high-quality evidence.)
input, CDC updated the draft document and obtained final CDC
1C. The literature search did not identify randomized controlled trials
clearance and coauthor approval.
that evaluated the benefits and harms of weight-adjusted paren-
teral antimicrobial prophylaxis dosing and its effect on the risk of
SSI. Other organizations have made recommendations based on
Recommendation Categories observational and pharmacokinetic data, and a summary of these
recommendations can be found in the Other Guidelines section of
Recommendations were categorized using the following standard sys-
the narrative summary for this question (eAppendix 1 of the Supple-
tem that reflects the level of supporting evidence or regulations:
ment). (No recommendation/unresolved issue.)
• Category IA: A strong recommendation supported by high to mod-
erate–quality evidence suggesting net clinical benefits or harms. 1D. The search did not identify sufficient randomized controlled trial
• Category IB: A strong recommendation supported by low-quality evidence to evaluate the benefits and harms of intraoperative re-
evidence suggesting net clinical benefits or harms or an accepted dosing of parenteral prophylactic antimicrobial agents for the pre-
practice (eg, aseptic technique) supported by low to very vention of SSI. Other organizations have made recommendations
low–quality evidence. based on observational and pharmacokinetic data, and a summary
• Category IC: A strong recommendation required by state or fed- of these recommendations can be found in the Other Guidelines sec-
eral regulation. tion of the narrative summary for this question (eAppendix 1 of the
• Category II: A weak recommendation supported by any quality Supplement). (No recommendation/unresolved issue.)
evidence suggesting a trade-off between clinical benefits and 1E. In clean and clean-contaminated procedures, do not administer
harms. additional prophylactic antimicrobial agent doses after the surgical
• No recommendation/unresolved issue: An issue for which there is incision is closed in the operating room, even in the presence of
low to very low–quality evidence with uncertain trade-offs be- a drain. (Category IA–strong recommendation; high-quality
tween the benefits and harms or no published evidence on out- evidence.)
comes deemed critical to weighing the risks and benefits of a given
intervention. Nonparenteral Antimicrobial Prophylaxis
2A.1. Randomized controlled trial evidence suggested uncertain
trade-offs between the benefits and harms regarding intraopera-
Recommendations tive antimicrobial irrigation (eg, intra-abdominal, deep, or subcuta-
Core Section neous tissues) for the prevention of SSI. Other organizations have
In 2006, approximately 80 million surgical procedures were per- made recommendations based on the existing evidence, and a sum-
formed in the United States at inpatient hospitals (46 million)7 mary of these recommendations can be found in the Other Guide-
and ambulatory hospital–affiliated or freestanding (32 million) lines section of the narrative summary for this question (eAppen-
settings.6 Between 2006 and 2009, SSIs complicated approxi- dix 1 of the Supplement). (No recommendation/unresolved issue.)
mately 1.9% of surgical procedures in the United States.19 How- 2A.2. The search did not identify randomized controlled trials that
ever, the number of SSIs is likely to be underestimated given that evaluated soaking prosthetic devices in antimicrobial solutions be-
approximately 50% of SSIs become evident after discharge.20 fore implantation for the prevention of SSI. (No recommendation/
Estimated mean attributable costs of SSIs range from $10 443 in unresolved issue.)
786 JAMA Surgery August 2017 Volume 152, Number 8 (Reprinted) jamasurgery.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
CDC Guideline for the Prevention of Surgical Site Infection, 2017 Special Communication Clinical Review & Education
2B.1. Do not apply antimicrobial agents (ie, ointments, solutions, or 6B. For patients with normal pulmonary function undergoing gen-
powders) to the surgical incision for the prevention of SSI. (Cat- eral anesthesia with endotracheal intubation, administer increased
egory IB–strong recommendation; low-quality evidence.) FIO2 during surgery and after extubation in the immediate postop-
2B.2. Application of autologous platelet-rich plasma is not neces- erative period. To optimize tissue oxygen delivery, maintain peri-
sary for the prevention of SSI. (Category II–weak recommendation; operative normothermia and adequate volume replacement. (Cat-
moderate-quality evidence suggesting a trade-off between clinical egory IA–strong recommendation; moderate-quality evidence.)
benefits and harms.) 6C. Randomized controlled trial evidence suggested uncertain trade-
2C. Consider the use of triclosan-coated sutures for the prevention offs between the benefits and harms regarding the administration
of SSI. (Category II–weak recommendation; moderate-quality evi- of increased FIO2 via face mask during the perioperative period in
dence suggesting a trade-off between clinical benefits and harms.) patients with normal pulmonary function undergoing general an-
esthesia without endotracheal intubation or neuraxial anesthesia (ie,
2D. Randomized controlled trial evidence suggested uncertain trade-
spinal, epidural, or local nerve blocks) for the prevention of SSI. (No
offs between the benefits and harms regarding antimicrobial
recommendation/unresolved issue.)
dressings applied to surgical incisions after primary closure in the
operating room for the prevention of SSI. (No recommendation/ 6D. Randomized controlled trial evidence suggested uncertain
unresolved issue.) trade-offs between the benefits and harms regarding the admin-
istration of increased FIO2 via face mask or nasal cannula during
Glycemic Control only the postoperative period in patients with normal pulmonary
function for the prevention of SSI. (No recommendation/
3A.1. Implement perioperative glycemic control and use blood glu- unresolved issue.)
cose target levels less than 200 mg/dL in patients with and with-
7. The search did not identify randomized controlled trials that evalu-
out diabetes. (Category IA–strong recommendation; high to mod-
ated the optimal target level, duration, and delivery method of FIO2
erate–quality evidence.)
for the prevention of SSI. Other organizations have made recom-
3A.2. The search did not identify randomized controlled trials that mendations based on observational studies, and a summary of these
evaluated lower (<200 mg/dL) or narrower blood glucose target lev- recommendations can be found in the Other Guidelines section of
els than recommended in this guideline nor the optimal timing, du- the narrative summary for this question (eAppendix 1 of the Supple-
ration, or delivery method of perioperative glycemic control for the ment). (No recommendation/unresolved issue.)
prevention of SSI. Other organizations have made recommenda-
tions based on observational evidence, and a summary of these rec-
ommendations can be found in the Other Guidelines section of the Antiseptic Prophylaxis
narrative summary for this question (eAppendix 1 of the Supple- 8A.1. Advise patients to shower or bathe (full body) with soap (an-
ment). (No recommendation/unresolved issue.) timicrobial or nonantimicrobial) or an antiseptic agent on at least the
3B. The search did not identify randomized controlled trials that night before the operative day. (Category IB–strong recommenda-
evaluated the optimal hemoglobin A1C target levels for the preven- tion; accepted practice.)
tion of SSI in patients with and without diabetes. (No recommen- 8A.2. Randomized controlled trial evidence suggested uncertain
dation/unresolved issue.) trade-offs between the benefits and harms regarding the optimal
timing of the preoperative shower or bath, the total number of soap
Normothermia or antiseptic agent applications, or the use of chlorhexidine glu-
4. Maintain perioperative normothermia. (Category IA–strong conate washcloths for the prevention of SSI. (No recommendation/
recommendation; high to moderate–quality evidence.) unresolved issue.)
5. The search did not identify randomized controlled trials that evalu- 8B. Perform intraoperative skin preparation with an alcohol-based
ated strategies to achieve and maintain normothermia, the lower antiseptic agent unless contraindicated. (Category IA–strong rec-
limit of normothermia, or the optimal timing and duration of nor- ommendation; high-quality evidence.)
mothermia for the prevention of SSI. Other organizations have 8C. Application of a microbial sealant immediately after intraopera-
made recommendations based on observational evidence, and a tive skin preparation is not necessary for the prevention of SSI. (Cat-
summary of these recommendations can be found in the Other egory II–weak recommendation; low-quality evidence suggesting a
Guidelines section of the narrative summary for this question trade-off between clinical benefits and harms.)
(eAppendix 1 of the Supplement). (No recommendation/ 8D. The use of plastic adhesive drapes with or without antimicro-
unresolved issue.) bial properties is not necessary for the prevention of SSI. (Category
II–weak recommendation; high to moderate–quality evidence sug-
Oxygenation gesting a trade-off between clinical benefits and harms.)
6A. Randomized controlled trial evidence suggested uncertain trade- 9A. Consider intraoperative irrigation of deep or subcutaneous
offs between the benefits and harms regarding the administration tissues with aqueous iodophor solution for the prevention of SSI. In-
of increased fraction of inspired oxygen (FIO2) via endotracheal in- traperitoneal lavage with aqueous iodophor solution in contami-
tubation during only the intraoperative period in patients with nor- nated or dirty abdominal procedures is not necessary. (Category
mal pulmonary function undergoing general anesthesia for the pre- II–weak recommendation; moderate-quality evidence suggesting a
vention of SSI. (No recommendation/unresolved issue.) trade-off between clinical benefits and harms.)
jamasurgery.com (Reprinted) JAMA Surgery August 2017 Volume 152, Number 8 787
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
Clinical Review & Education Special Communication CDC Guideline for the Prevention of Surgical Site Infection, 2017
9B. The search did not identify randomized controlled trials that 14. For prosthetic joint arthroplasty patients receiving systemic
evaluated soaking prosthetic devices in antiseptic solutions before corticosteroid or other immunosuppressive therapy, recommen-
implantation for the prevention of SSI. (No recommendation/ dation 1E applies: in clean and clean-contaminated procedures,
unresolved issue.) do not administer additional antimicrobial prophylaxis doses after
10. Randomized controlled trial evidence was insufficient to evalu- thesurgical incision is closed in the operating room, even in the
ate the trade-offs between the benefits and harms of repeat appli- presence of a drain. (Category IA–strong recommendation; high-
cation of antiseptic agents to the patient’s skin immediately before quality evidence.)
closing the surgical incision for the prevention of SSI. (No recom-
mendation/unresolved issue.) Intra-articular Corticosteroid Injection
15 and 16. Available evidence suggested uncertain trade-offs
Prosthetic Joint Arthroplasty Section between the benefits and harms of the use and timing of preop-
Prevention efforts should target all surgical procedures but espe- erative intra-articular corticosteroid injection on the incidence of
cially those in which the human and financial burden is greatest. SSI in prosthetic joint arthroplasty. Other organizations have
In 2011, primary total knee arthroplasty accounted for more than made recommendations based on observational studies, and a
half of the 1.2 million prosthetic joint arthroplasty procedures (pri- summary of these recommendations can be found in the Other
mary and revision) performed in the United States, followed by Guidelines section of the narrative summary for this question
total hip arthroplasty and hip hemiarthroplasty.24 Primary shoul- (eAppendix 1 of the Supplement). (No recommendation/
der, elbow, and ankle arthroplasties are much less common. By unresolved issue.)
2030, prosthetic joint arthroplasties are projected to increase to
3.8 million procedures per year.25-27
Anticoagulation
Infection is the most common indication for revision in total
knee arthroplasty28 and the third most common indication in 17. Available evidence suggested uncertain trade-offs between
total hip arthroplasty. 28 By 2030, the infection risk for hip the benefits and harms of venous thromboembolism prophylaxis
and knee arthroplasty is expected to increase from 2.18%22 to on the incidence of SSI in prosthetic joint arthroplasty. Other
6.5% and 6.8%, respectively.25 In addition, owing to increasing organizations have made recommendations based on the existing
risk and the number of individuals undergoing prosthetic joint evidence, and these references can be found in the Other Guide-
arthroplasty procedures, the total number of hip and knee pros- lines section of the narrative summary for this question (eAppen-
thetic joint infections is projected to increase to 221 500 cases dix 1 of the Supplement). (No recommendation/unresolved
per year by 2030, at a cost of more than $1.62 billion.22,25 The issue.)
Prosthetic Joint Arthroplasty section contains recommendations
that are applicable to these procedures (eAppendix 1 of the Orthopedic Surgical Space Suit
Supplement).
18. Available evidence suggested uncertain trade-offs between the
benefits and harms of orthopedic space suits or the health care per-
Blood Transfusion
sonnel who should wear them for the prevention of SSI in pros-
11A. Available evidence suggested uncertain trade-offs between thetic joint arthroplasty. (No recommendation/unresolved issue.)
the benefits and harms of blood transfusions on the risk of
SSI in prosthetic joint arthroplasty. Other organizations
Postoperative Antimicrobial Prophylaxis
have made recommendations on this topic, and a reference
Duration With Drain Use
to these recommendations can be found in the Other Guide-
lines section of the narrative summary for this question (eAppen- 19. In prosthetic joint arthroplasty, recommendation 1E applies: in
dix 1 of the Supplement). (No recommendation/unresolved clean and clean-contaminated procedures, do not administer addi-
issue.) tional antimicrobial prophylaxis doses after the surgical incision is
11B. Do not withhold transfusion of necessary blood products from closed in the operating room, even in the presence of a drain. (Cat-
surgical patients as a means to prevent SSI. (Category IB–strong rec- egory IA–strong recommendation; high-quality evidence.)
ommendation; accepted practice.)
Biofilm
Systemic Immunosuppressive Therapy 20A. Available evidence suggested uncertain trade-offs between the
benefits and harms regarding cement modifications and the pre-
12 and 13. Available evidence suggested uncertain trade-offs
vention of biofilm formation or SSI in prosthetic joint arthroplasty.
between the benefits and harms of systemic corticosteroid
(No recommendation/unresolved issue.)
or other immunosuppressive therapies on the risk of SSI in
prosthetic joint arthroplasty. Other organizations have made 20B. The search did not identify studies evaluating prosthesis modi-
recommendations based on the existing evidence, and a sum- fications for the prevention of biofilm formation or SSI in pros-
mary of these recommendations can be found in the Other thetic joint arthroplasty. (No recommendation/unresolved issue.)
Guidelines section of the narrative summary for this question 20C. The search did not identify studies evaluating vaccines for the
(eAppendix 1 of the Supplement). (No recommendation/ prevention of biofilm formation or SSI in prosthetic joint arthro-
unresolved issue.) plasty. (No recommendation/unresolved issue.)
788 JAMA Surgery August 2017 Volume 152, Number 8 (Reprinted) jamasurgery.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
CDC Guideline for the Prevention of Surgical Site Infection, 2017 Special Communication Clinical Review & Education
20D. The search did not identify studies evaluating biofilm control new and updated recommendations are not only useful for health
agents, such as biofilm dispersants, quorum sensing inhibitors, or care professionals but also can be used as a resource for profes-
novel antimicrobial agents, for the prevention of biofilm formation sional societies or organizations to develop more detailed imple-
or SSI in prosthetic joint arthroplasty. (No recommendation/ mentation guidance or to identify future research priorities. The pau-
unresolved issue.) city of robust evidence across the entire guideline created challenges
in formulating recommendations for the prevention of SSI. None-
theless, the thoroughness and transparency achieved using a sys-
tematic review and the GRADE approach to address clinical ques-
Conclusions
tions of interest to stakeholders are critical to the validity of the clinical
Surgical site infections are persistent and preventable health care– recommendations.
associated infections. There is increasing demand for evidence- The number of unresolved issues in this guideline reveals sub-
based interventions for the prevention of SSI. The last version of the stantial gaps that warrant future research. A select list of these un-
CDC Guideline for Prevention of Surgical Site Infection18 was pub- resolved issues may be prioritized to formulate a research agenda
lished in 1999. While the guideline was evidence informed, most rec- to advance the field. Adequately powered, well-designed studies that
ommendations were based on expert opinion, in the era before evi- assess the effect of specific interventions on the incidence of SSI are
dence-based guideline methods. CDC updated that version of the needed to address these evidence gaps. Subsequent revisions to this
guideline using GRADE as the evidence-based method that pro- guideline will be guided by new research and technological advance-
vides the foundation of the recommendations in this guideline. These ments for preventing SSIs.
ARTICLE INFORMATION Author Contributions: Dr Umscheid and Ms Stone reported receiving lecture fees from Forest
Accepted for Publication: March 1, 2017. had full access to all of the data in the study and Laboratories, Merck/Merck Sharp and Dohme, and
take responsibility for the integrity of the data and Pfizer; and reported that his institution received
Correction: This article was corrected on June 21, the accuracy of the data analysis. funding for his consultancy to AstraZeneca and
2017, to fix corrupted numbering and update Study concept and design: Berríos-Torres, grants from AstraZeneca, Bayer, Merck/MSD, and
abstract and methods. Umscheid, Bratzler, Leas, Stone, Kelz, Morgan, Tetraphase. Dr Dellinger reported receiving grants
Published Online: May 3, 2017. Mazuski, Dellinger, Itani, Berbari, Parvizi, Blanchard, for clinical research from, serving on an advisory
doi:10.1001/jamasurg.2017.0904 Kluytmans. board for, or lecturing for honoraria from the
Author Affiliations: Division of Healthcare Quality Acquisition, analysis, or interpretation of data: following: Merck, Baxter, Ortho-McNeil, Targanta,
Promotion, Centers for Disease Control and Berríos-Torres, Umscheid, Bratzler, Leas, Stone, Schering-Plough, WebEx, Astellas, Care Fusion,
Prevention, Atlanta, Georgia (Berríos-Torres, Stone, Kelz, Reinke, Morgan, Solomkin, Mazuski, Dellinger, Durata, Pfizer, Applied Medical, Rib-X, Affinium,
Donlan); Center for Evidence-Based Practice, Segreti, Allen, Kluytmans, Donlan, Schecter. and 3M. Dr Itani reported that his institution
University of Pennsylvania Health System, Drafting of the manuscript: Berríos-Torres, received grants from Merck, Cubist, Dr Reddy’s,
Philadelphia (Umscheid, Leas, Kelz, Morgan); Umscheid, Leas, Stone, Kelz, Reinke, Morgan, Itani, Sanofi Pasteur, and Trius for research trials;
College of Public Health, The University of Berbari, Segreti, Blanchard. reported clinical advisory board membership at
Oklahoma Health Sciences Center, Oklahoma City Critical revision of the manuscript for important Forrest Pharmaceuticals; and reported payment for
(Bratzler); Carolinas Healthcare System, Charlotte, intellectual content: Berríos-Torres, Umscheid, development of educational presentations for Med
North Carolina (Reinke); Department of Surgery, Bratzler, Leas, Stone, Kelz, Reinke, Solomkin, Direct and Avid Education. Dr Berbari reported that
University of Cincinnati College of Medicine, Mazuski, Dellinger, Itani, Berbari, Segreti, Parvizi, his institution received a grant from Pfizer for a
Cincinnati, Ohio (Solomkin); Section of Acute and Allen, Kluytmans, Donlan, Schecter. research trial for which he serves as the principal
Critical Care Surgery, Washington University School Statistical analysis: Berríos-Torres, Umscheid, Leas. investigator. Dr Segreti reported receiving lecture
of Medicine in St Louis, Saint Louis, Missouri Administrative, technical, or material support: fees from Pfizer, Merck, and Forest Laboratories
(Mazuski); American College of Surgeons Berríos-Torres, Bratzler, Leas, Stone, Morgan, Itani, and reported owning stocks in or having stock
Representative, University of Washington Medical Parvizi. options from Pfizer. Dr Parvizi reported being a paid
Center, Seattle (Dellinger); Surgical Infection Study supervision: Berríos-Torres, Umscheid, consultant for Zimmer, Smith and Nephew,
Society Representative, Veterans Affairs Boston Bratzler, Stone, Itani, Berbari, Parvizi. ConvaTec, TissueGene, CeramTech, and Medtronic;
Healthcare System, Boston University and Harvard Conflict of Interest Disclosures: Drs Umscheid, reported receiving royalties from Elsevier, Wolters
Medical School, Boston, Massachusetts (Itani); Kelz, and Morgan and Mr Leas reported receiving Kluwer, Slack Incorporated, Data Trace Publishing,
Musculoskeletal Infection Society Representative, funding from the Centers for Disease Control and and Jaypee Brothers Medical Publishers; and
Mayo Clinic College of Medicine, Rochester, Prevention to support the guideline development reported having stock options with Hip Innovation
Minnesota (Berbari); American Academy of process. Dr Bratzler reported being a consultant for Technologies, CD Diagnostics, and PRN. Dr Allen
Orthopaedic Surgeons Representative, Rush the Oklahoma Foundation for Medical Quality and reported receiving lecture fees from Ethicon and
University Medical Center, Chicago, Illinois for Telligen (a nonprofit Medicaid external quality royalties from Wolters Kluwer as an author for
(Segreti); American Academy of Orthopaedic review organization) and reported that his Infection Control: A Practical Guide for Healthcare
Surgeons Representative, Rothman Institute, institution received payment for his lectures, Facilities. Dr Kluytmans reported being a paid
Philadelphia, Pennsylvania (Parvizi); Quality including service on speakers’ bureaus from consultant for 3M, Johnson & Johnson, and Pfizer.
Department, Littleton Adventist Hospital, Denver, Premier and Janssen Pharmaceuticals. Dr Reinke No other disclosures were reported.
Colorado (Blanchard); Association of Perioperative reported receiving lecture fees from Covidien and Funding/Support: The Centers for Disease Control
Registered Nurses Representative, New York reported being a paid consultant for Teleflex. Dr and Prevention (CDC) supported the development
Methodist Hospital, Brooklyn (Allen); Laboratory Solomkin reported receiving grants for clinical of the guideline. The activities of Drs Umscheid,
for Microbiology and Infection Control, Amphia research from, receiving consulting fees regarding Kelz, and Morgan and Mr Leas were supported
Hospital, Breda, the Netherlands (Kluytmans); clinical trial data, serving on an advisory board for, through a short-term detail under contract at CDC
Julius Center for Health Sciences and Primary Care, or lecturing for honoraria from the following: (10IPA1004117, 10IPA1004133, 11IPA1106551,
University Medical Center, Utrecht, the Netherlands Merck, Actavis, AstraZeneca, PPD, Tetraphase, 11IPA1106555, and 11IPA1106565).
(Kluytmans); Department of Surgery, San Francisco Johnson & Johnson, and 3M. Dr Mazuski reported Role of the Funder/Sponsor: Centers for Disease
General Hospital, University of California, San being a paid consultant for Bayer, Cubist Control and Prevention conducted the full guideline
Francisco (Schecter). Pharmaceuticals, Forest Laboratories, MedImmune, development process, directing the design and
Merck/Merck Sharp and Dohme, and Pfizer; conduct of the systematic reviews; collection,
jamasurgery.com (Reprinted) JAMA Surgery August 2017 Volume 152, Number 8 789
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
Clinical Review & Education Special Communication CDC Guideline for the Prevention of Surgical Site Infection, 2017
management, analysis, and interpretation of the National Association of County and City Health Pathogenesis, University of Maryland, Baltimore).
data; and preparation, review, and approval for Officials; Holly Harmon, RN, MBA, American Health None received compensation outside of their usual
submission of the manuscript for publication. Care Association; Patrick Horine, MHA, DNV salary.
Centers for Disease Control and Prevention staff Healthcare, Inc; Michael D. Howell, MD, MPH,
members were responsible for the overall design Society of Critical Care Medicine; W. Charles REFERENCES
and conduct of the guideline and preparation, Huskins, MD, MSC, Infectious Diseases Society of 1. National Healthcare Safety Network, Centers for
review, and approval of the manuscript. America; Marion Kainer, MD, MPH, Council of State Disease Control and Prevention. Surgical site
Group Information: The Healthcare Infection and Territorial Epidemiologists; Emily Lutterloh, infection (SSI) event. http://www.cdc.gov/nhsn
Control Practices Advisory Committee (HICPAC) MD, MPH, Association of State and Territorial /pdfs/pscmanual/9pscssicurrent.pdf. Published
members are as follows: Hilary M. Babcock, MD, Health Officials; Lisa Maragakis, MD, Society for January 2017. Accessed January 25, 2017.
MPH, Washington University School of Medicine in Healthcare Epidemiology of America; Michael
McElroy, MPH, CIC, America’s Essential Hospitals; 2. Fry DE. Fifty ways to cause surgical site
St Louis; Dale W. Bratzler, DO, MPH, The University infections. Surg Infect (Larchmt). 2011;12(6):497-500.
of Oklahoma Health Sciences Center; Patrick J. Lisa McGiffert, Consumers Union; Silvia
Brennan, MD, University of Pennsylvania Health Muñoz-Price, MD, America’s Essential Hospitals; 3. Anderson DJ, Kirkland KB, Kaye KS, et al.
System; Vickie M. Brown, RN, MPH, WakeMed Shirley Paton, RN, MN, Public Health Agency of Underresourced hospital infection control and
Health & Hospitals; Lillian A. Burns, MT, MPH, Canada; Michael Anne Preas, RN, CIC, Association prevention programs: penny wise, pound foolish?
Greenwich Hospital; Ruth M. Carrico, PhD, RN, CIC, of Professionals of Infection Control and Infect Control Hosp Epidemiol. 2007;28(7):767-773.
University of Louisville School of Medicine; Sheri Epidemiology, Inc; Mark E. Rupp, MD, Society for 4. Centers for Disease Control and Prevention. The
Chernetsky Tejedor, MD, Emory University School Healthcare Epidemiology of America; Mark Russi, direct medical costs of healthcare-associated
of Medicine; Daniel J. Diekema, MD, University of MD, MPH, American College of Occupational and infections in U.S. hospitals and the benefits of
Iowa Carver College of Medicine; Alexis Elward, MD, Environmental Medicine; Sanjay Saint, MD, MPH, prevention. http://www.cdc.gov/hai/pdfs/hai/scott
Washington University School of Medicine in St Society of Hospital Medicine; Robert G. Sawyer, _costpaper.pdf. Published 2009. Accessed January
Louis; Neil O. Fishman, MD, University of MD, Surgical Infection Society; Roslyne Schulman, 25, 2017.
Pennsylvania Health System; Ralph Gonzales, MD, MHA, MBA, American Hospital Association; Rachel
Stricof, MPH, Advisory Council for the Elimination 5. Stone PW, Braccia D, Larson E. Systematic
MSPH, University of California, San Francisco; Mary review of economic analyses of health
K. Hayden, MD, Rush University Medical Center; of Tuberculosis; Donna Tiberi, RN, MHA, Healthcare
Facilities Accreditation Program; Margaret care–associated infections. Am J Infect Control.
Susan Huang, MD, MPH, University of California 2005;33(9):501-509.
Irvine School of Medicine; W. Charles Huskins, MD, VanAmringe, MHS, The Joint Commission; Stephen
MSc, Mayo Clinic College of Medicine; Lynn Weber, MD, Infectious Diseases Society of America; 6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory
Janssen, MS, CIC, CPHQ, California Department of Elizabeth Wick, MD, American College of Surgeons; surgery in the United States, 2006. National Health
Public Health; Tammy Lundstrom, MD, JD, Robert Wise, MD, The Joint Commission; and Statistics Reports 11. http://www.cdc.gov/nchs/data
Providence Hospital; Lisa Maragakis, MD, MPH, The Amber Wood, MSN, RN, CNOR, CIC, CPN, /nhsr/nhsr011.pdf. Revised September 4, 2009.
Johns Hopkins Hospital; Yvette S. McCarter, PhD, Association of Perioperative Registered Nurses. Accessed January 25, 2017.
University of Florida Health Science Center; Denise Disclaimer: The opinions of the reviewers might 7. DeFrances CJ, Podgornik MN. 2004 National
M. Murphy, MPH, RN, CIC, Main Line Health not be reflected in all of the recommendations Hospital Discharge Survey. Adv Data. 2006;(371):1-
System; Russell N. Olmsted, MPH, St Joseph Mercy contained in this document. 19.
Health System; Stephen Ostroff, MD, US Food and Additional Information: Before July 2014, Dr 8. US Department of Health and Human Services.
Drug Administration; Jan Patterson, MD, University Berríos-Torres was employed at Centers for Disease National action plan to prevent health
of Texas Health Science Center, San Antonio; David Control and Prevention. She has no affiliation since care–associated infections: road map to
A. Pegues, MD, David Geffen School of Medicine at July 2014. Authors recused themselves from elimination. https://health.gov/hcq/prevent
UCLA; Peter J. Pronovost, MD, PhD, The Johns discussions if they had competing interests related -hai-action-plan.asp. Published 2013. Accessed
Hopkins University; Gina Pugliese, RN, MS, Premier to recommendations under discussion. For January 25, 2017.
Healthcare Alliance; Selwyn O. Rogers Jr, MD, MPH, product-specific recommendation discussions (eg,
The University of Texas Medical Branch; William P. 9. Centers for Medicare and Medicaid Services
triclosan-coated sutures), a new declaration of (CMS), HHS. Medicare Program; hospital inpatient
Schecter, MD, University of California, San conflicts specific to that topic was requested from
Francisco; Barbara M. Soule, RN, MPA, CIC, The prospective payment systems for acute care
each author before his or her input was considered hospitals and the long-term care hospital
Joint Commission; Tom Talbot, MD, MPH, in the formulation of the recommendation.
Vanderbilt University Medical Center; Michael L. prospective payment system changes and FY2011
Tapper, MD, Lenox Hill Hospital; and Deborah S. Additional Contributions: The Centers for Disease rates; provider agreements and supplier approvals;
Yokoe, MD, MPH, Brigham & Women’s Hospital. Control and Prevention thanks the many individuals and hospital conditions of participation for
and organizations who provided valuable feedback rehabilitation and respiratory care services;
Ex Officio Members: William B. Baine, MD, Agency on the guideline during the development process, Medicaid program: accreditation for providers of
for Healthcare Research and Quality; Elizabeth especially the following experts for their input inpatient psychiatric services. Final rules and
Claverie-Williams, MS, US Food and Drug throughout the process: Rajender Agarwal, MD, interim final rule with comment period. Fed Regist.
Administration; David Henderson, MD, National MPH (Center for Evidence-Based Practice, 2010;75(157):50041-50681.
Institutes of Health; Jeannie Miller, RN, MPH, University of Pennsylvania Health System,
Centers for Medicare & Medicaid Services; Paul D. 10. US Government Printing Office. The Deficit
Philadelphia); J. William Costerton, PhD (Center for Reduction Act of 2005. http://www.gpo.gov/fdsys
Moore, PhD, Health Resources and Services Genomic Sciences, Allegheny-Singer Research
Administration; Sheila Murphey, MD, US Food and /pkg/BILLS-109s1932enr/pdf/BILLS-109s1932enr
Institute, Pittsburgh, Pennsylvania); Jeffrey C. .pdf. Published 2006. Accessed January 25, 2017.
Drug Administration; and Daniel Schwartz, MD, Hageman, MHS (Division of Healthcare Quality
MBA, Centers for Medicare & Medicaid Services. Promotion, Centers for Disease Control and 11. Umscheid CA, Mitchell MD, Doshi JA, Agarwal R,
Liaisons: Joan Blanchard, RN, BSN, Association of Prevention, Atlanta, Georgia); Thomas Hunt, MD Williams K, Brennan PJ. Estimating the proportion
Perioperative Registered Nurses; William A. Brock, (Department of Surgery, University of California at of healthcare-associated infections that are
MD, Society of Critical Care Medicine; Barbara San Francisco); Bernard Morrey, MD (Department reasonably preventable and the related mortality
DeBaun, MSN, RN, CIC, Association of Professionals of Orthopedic Surgery, Mayo Clinic, Rochester, and costs. Infect Control Hosp Epidemiol. 2011;32
of Infection Control and Epidemiology, Inc; Minnesota); Lena M. Napolitano, MD (Division of (2):101-114.
Kathleen Dunn, BScN, MN, RN, Public Health Acute Care Surgery, University of Michigan Health 12. Guyatt GH, Oxman AD, Kunz R, et al; GRADE
Agency of Canada; Sandra Fitzler, RN, American Systems, Ann Arbor); Douglas Osmon, MD Working Group. Going from evidence to
Health Care Association; Nancy Foster, American (Department of Infectious Diseases, Mayo Clinic, recommendations. BMJ. 2008;336(7652):1049-1051.
Hospital Association; Janet Franck, RN, MBA, CIC, Rochester, Minnesota); Robin Patel, MD(CM), 13. Guyatt GH, Oxman AD, Kunz R, Vist GE,
DNV Healthcare, Inc; Diana Gaviria, MD, MPH, FRCP(C), D(ABMM) (Infectious Diseases Research Falck-Ytter Y, Schünemann HJ; GRADE Working
National Association of County and City Health Laboratory, Mayo Clinic, Rochester, Minnesota);
Officials; Jennifer Gutowski, MPH, BSN, RN, CIC, and Mark Shirtliff, PhD (Department of Microbial
790 JAMA Surgery August 2017 Volume 152, Number 8 (Reprinted) jamasurgery.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
CDC Guideline for the Prevention of Surgical Site Infection, 2017 Special Communication Clinical Review & Education
Group. What is “quality of evidence” and why is it Prevention (CDC) Hospital Infection Control patients with Staphylococcus aureus surgical site
important to clinicians? BMJ. 2008;336(7651):995- Practices Advisory Committee. Guideline for infection. Clin Infect Dis. 2003;36(5):592-598.
998. prevention of surgical site infection, 1999. Am J 24. HCUPnet. Healthcare Cost and Utilization
14. Guyatt GH, Oxman AD, Vist GE, et al; GRADE Infect Control. 1999;27(2):97-132. Project, Agency for Healthcare Research and
Working Group. GRADE: an emerging consensus on 19. Mu Y, Edwards JR, Horan TC, Berríos-Torres SI, Quality. 2011 Nationwide Inpatient Sample (NIS).
rating quality of evidence and strength of Fridkin SK. Improving risk-adjusted measures of https://www.hcup-us.ahrq.gov/nisoverview.jsp.
recommendations. BMJ. 2008;336(7650):924-926. surgical site infection for the National Healthcare Published 2011. Accessed January 25, 2017.
15. Schünemann HJ, Oxman AD, Brozek J, et al; Safety Network. Infect Control Hosp Epidemiol. 25. Kurtz S, Ong K, Lau E, Mowat F, Halpern M.
GRADE Working Group. Grading quality of evidence 2011;32(10):970-986. Projections of primary and revision hip and knee
and strength of recommendations for diagnostic 20. McKibben L, Horan T, Tokars JI, et al; arthroplasty in the United States from 2005 to
tests and strategies. BMJ. 2008;336(7653):1106-1110. Heathcare Infection Control Practices Advisory 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
16. Umscheid CA, Agarwal RK, Brennan PJ; Committee. Guidance on public reporting of 26. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K,
Healthcare Infection Control Practices Advisory healthcare-associated infections: Parvizi J. Infection burden for hip and knee
Committee, Centers for Disease Control and recommendations of the Healthcare Infection arthroplasty in the United States. J Arthroplasty.
Prevention. Updating the guideline methodology of Control Practices Advisory Committee. Am J Infect 2008;23(7):984-991.
the Healthcare Infection Control Practices Advisory Control. 2005;33(4):217-226.
27. Kurtz SM, Ong KL, Schmier J, Zhao K, Mowat F,
Committee (HICPAC). http://www.cdc.gov/hicpac 21. Bozic KJ, Ries MD. The impact of infection after Lau E. Primary and revision arthroplasty surgery
/pdf/guidelines/2009-10-29HICPAC total hip arthroplasty on hospital and surgeon caseloads in the United States from 1990 to 2004.
_GuidelineMethodsFINAL.pdf. Published 2010. resource utilization. J Bone Joint Surg Am. 2005;87 J Arthroplasty. 2009;24(2):195-203.
Accessed January 25, 2017. (8):1746-1751.
28. Bozic KJ, Kurtz SM, Lau E, et al. The
17. Umscheid CA, Agarwal RK, Brennan PJ; 22. Kurtz SM, Lau E, Watson H, Schmier JK, Parvizi epidemiology of revision total knee arthroplasty in
Healthcare Infection Control Practices Advisory J. Economic burden of periprosthetic joint infection the United States. Clin Orthop Relat Res. 2010;468
Committee. Updating the guideline development in the United States. J Arthroplasty. 2012;27(8) (1):45-51.
methodology of the Healthcare Infection Control (suppl):61-5.e1.
Practices Advisory Committee (HICPAC). Am J 23. Engemann JJ, Carmeli Y, Cosgrove SE, et al.
Infect Control. 2010;38(4):264-273. Adverse clinical and economic outcomes
18. Mangram AJ, Horan TC, Pearson ML, Silver LC, attributable to methicillin resistance among
Jarvis WR; Centers for Disease Control and
Invited Commentary
Surgical Site Infection Prevention—
What We Know and What We Do Not Know
Pamela A. Lipsett, MD, MHPE, MCCM
Surgical site infections remain among remain the most com- of the proposed intervention because of lack of outcomes. The
mon preventable infections today. Recently, the World Health authors ultimately provide 42 statements, including 8 Cat-
Organization1,2 and the American College of Surgeons and Sur- egory 1A, 4 Category 1B, 5 Category II, and 25 areas for which
gical Infection Society3 published their guidelines for the they made no recommendation or considered the area unre-
prevention of surgical site in- solved. The fact that most statements were unresolved, espe-
fections. In this journal, the cially regarding prosthetic joint surgery, shows our investiga-
Related article page 784 long-awaited update to the tors where we should be putting forth our efforts in clinical
1999 guidelines from the Cen- trials. There is a lot of opportunity to learn how we can pro-
ters for Disease Control and Prevention (CDC) have now been vide more effective care to our patients.
published.4,5 With the publication of guidelines from 3 repu- The 12 Category 1A and Category 1B recommendations are
table sources, where should the surgeon turn for guidance? based on moderate or high–quality evidence, and we should be
What are the major controversies? What is new and where do using these recommendations in our practice. These key areas
we need to perform new research? The CDC guidelines use a include (but are not limited to) the use of antimicrobial prophy-
strict process for literature review, development of consen- laxis to achieve bactericidal concentrations in serum and
sus, public reporting, and refinement of their final recommen- tissues, including before cesarean section, and are limited to dur-
dations. The article from the CDC by Berríos-Torres et al5 in this ing the operation. Furthermore, we should not be using anti-
issue of JAMA Surgery is useful to every surgeon because it is biotics because the patient has a drain, whether or not a pros-
brief and summarizes the recommendations, with their level thetic joint is in place. These recommendations are likely to be
of support. It tells us what we should do and what we do not the most difficult to operationalize because some surgeons and
know. The supplementary material is inclusive and recom- practices have had difficulty confining antibiotic use to just 24
mended for anyone with a thirst for the evidence supporting hours after a clean or clean-contaminated procedure, let alone
these recommendations. Unfortunately, in many cases the au- when a drain is in place. Glycemic control should be achieved
thors make no recommendation with respect to support or in all patients, with a glucose target less than 200 mg/dL.
harm if the level of the evidence was low or very low or if they Normothermia should be maintained, and a higher fraction
were unable to judge trade-offs between harms and benefits of inspired oxygen should be used in patients with normal
jamasurgery.com (Reprinted) JAMA Surgery August 2017 Volume 152, Number 8 791
© 2017 American Medical Association. All rights reserved.
Downloaded From: on 04/02/2018
Вам также может понравиться
- Criterios de Tokio 2018Документ14 страницCriterios de Tokio 2018Luis CoraspeОценок пока нет
- Guia de TokioДокумент14 страницGuia de TokioMiguel Alonso Pérez MoreОценок пока нет
- Mayumi Et Al-2018-Journal of Hepato-Biliary-Pancreatic SciencesДокумент5 страницMayumi Et Al-2018-Journal of Hepato-Biliary-Pancreatic SciencesAndres RiveraОценок пока нет
- Pelvic Inflammatory Disease and Risk of Cancer: A Nationwide Cohort StudyДокумент3 страницыPelvic Inflammatory Disease and Risk of Cancer: A Nationwide Cohort Studymaria isabelОценок пока нет
- Gynecologic Oncology: Jinlan Piao, Eun Ji Lee, Maria LeeДокумент7 страницGynecologic Oncology: Jinlan Piao, Eun Ji Lee, Maria Leemaria isabelОценок пока нет
- Placas de Aparato Reproductor MasculinoДокумент2 страницыPlacas de Aparato Reproductor Masculinomaria isabelОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Using Statistical Techniq Ues in Analyzing DataДокумент40 страницUsing Statistical Techniq Ues in Analyzing Datadanielyn aradillos100% (1)
- Business Analysis Book of Knowledge Version Three PDFДокумент3 страницыBusiness Analysis Book of Knowledge Version Three PDFiloveshms100% (1)
- Statistics for Business - Understanding Sampling DistributionsДокумент24 страницыStatistics for Business - Understanding Sampling DistributionsUsmanОценок пока нет
- Adorno Authoritarian Personality PDFДокумент314 страницAdorno Authoritarian Personality PDFAlbiHellsing100% (1)
- Review Notes In: Rkmfiles Center For Comprehensive StudiesДокумент165 страницReview Notes In: Rkmfiles Center For Comprehensive StudiesGenela RiblezaОценок пока нет
- Objectives of Managerial EconomicsДокумент5 страницObjectives of Managerial Economicssukul756Оценок пока нет
- Sales MGMT Course OutlineДокумент7 страницSales MGMT Course OutlineRaza AliОценок пока нет
- 01 - Capstone B+ Cap Submission - Paras ChauhanДокумент23 страницы01 - Capstone B+ Cap Submission - Paras ChauhanParas ChauhanОценок пока нет
- Article WritingДокумент10 страницArticle WritingMosteroidОценок пока нет
- PTA School of Excellence Action PlanДокумент4 страницыPTA School of Excellence Action PlanCarl DominiqueОценок пока нет
- Theoretical Framework: Kinds of ResearchДокумент4 страницыTheoretical Framework: Kinds of ResearchMiyang100% (1)
- Investigation of Performance Metrics in Regression Analysis and Machine Learning-Based Prediction ModelsДокумент26 страницInvestigation of Performance Metrics in Regression Analysis and Machine Learning-Based Prediction Modelsalisha.neeri1792Оценок пока нет
- Forensic Comm Ibnu HamadДокумент13 страницForensic Comm Ibnu HamadRessa PatrissiaОценок пока нет
- Sport Management Review: Jessie Brouwers, Popi Sotiriadou, Veerle de BosscherДокумент16 страницSport Management Review: Jessie Brouwers, Popi Sotiriadou, Veerle de BosscherGabriela Ioana IonitaОценок пока нет
- The 2015 ICNDT Guide On: Education and Training in NDTДокумент18 страницThe 2015 ICNDT Guide On: Education and Training in NDTNdt ElearningОценок пока нет
- 10 - Chapter 1Документ22 страницы10 - Chapter 1SowntharieaОценок пока нет
- Practical Research 1: Quarter 3 - Module 14: Literature Review: Elements and EthicsДокумент24 страницыPractical Research 1: Quarter 3 - Module 14: Literature Review: Elements and EthicsRemar Jhon Paine100% (2)
- IB DP Chemistry HL IA: Free-range Eggs Have Higher Calcium CarbonateДокумент8 страницIB DP Chemistry HL IA: Free-range Eggs Have Higher Calcium CarbonateWalter Chung Yin LeungОценок пока нет
- Community Engagement Intern Job DescriptionДокумент2 страницыCommunity Engagement Intern Job DescriptionPlanned Parenthood Association of UtahОценок пока нет
- Python CodeTantra Unit-5 & Unit-6Документ4 страницыPython CodeTantra Unit-5 & Unit-6sainiranjan2005Оценок пока нет
- Clinical Appraisal of Journals On Therapy: Joy Grace G. Jerusalem MD, FPCS, FPSGSДокумент71 страницаClinical Appraisal of Journals On Therapy: Joy Grace G. Jerusalem MD, FPCS, FPSGSKeith GarciaОценок пока нет
- Readings in Philippine History: Midterm Exam: Prepared By: Allyssa Mae B. Biron Bsce - 1BДокумент6 страницReadings in Philippine History: Midterm Exam: Prepared By: Allyssa Mae B. Biron Bsce - 1BArt Cabby SarzaОценок пока нет
- Personality and Consumer BehaviorДокумент5 страницPersonality and Consumer BehaviorAbu BakarОценок пока нет
- Coping strategies of ICU nurses in overcoming work stressДокумент8 страницCoping strategies of ICU nurses in overcoming work stressRirin Muthia ZukhraОценок пока нет
- Chi-Squared Test Worked ExampleДокумент2 страницыChi-Squared Test Worked ExampleAbhijit MandalОценок пока нет
- OBrien 2018 A New Model For Injury Prevention in Team SportsДокумент5 страницOBrien 2018 A New Model For Injury Prevention in Team SportsBОценок пока нет
- Research Paper On Emotional Intelligence and Academic AchievementДокумент5 страницResearch Paper On Emotional Intelligence and Academic Achievementefjddr4z100% (1)
- PERIN FCT WP2023 2024 ConcursosДокумент11 страницPERIN FCT WP2023 2024 ConcursoszeОценок пока нет
- The Relationship Between Reward System, Employee Motivation and Employees Performance in Car Dealers Located in Kingdom of BahrainДокумент6 страницThe Relationship Between Reward System, Employee Motivation and Employees Performance in Car Dealers Located in Kingdom of BahrainInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- IECB Cie Pie Application Form 1022007Документ2 страницыIECB Cie Pie Application Form 1022007Anonymous d6EtxrtbОценок пока нет