Вам также может понравиться
- Car Accidents Handbook: Why Car Accident Victims Deserve a Book to Protect Their RightsОт EverandCar Accidents Handbook: Why Car Accident Victims Deserve a Book to Protect Their RightsРейтинг: 2 из 5 звезд2/5 (1)
- Myths & Facts About Low Speed Collisions and Occupant InjuryОт EverandMyths & Facts About Low Speed Collisions and Occupant InjuryОценок пока нет
- Primary Impact Injuries Are Caused by The First Impact of The Vehicle With TheДокумент4 страницыPrimary Impact Injuries Are Caused by The First Impact of The Vehicle With TheJohn Winchester PalmonesОценок пока нет
- Age Estimation & Bone Ossification: DR Singh D.,MD, DNBДокумент23 страницыAge Estimation & Bone Ossification: DR Singh D.,MD, DNBHarish AgarwalОценок пока нет
- Road Traffic Accidents: Injuries To PedestriansДокумент5 страницRoad Traffic Accidents: Injuries To PedestriansZuhair Mohammed FadlalbariОценок пока нет
- Transportation Injuries (Review of Forensic Medicine and Toxicology, 2nd Edition)Документ14 страницTransportation Injuries (Review of Forensic Medicine and Toxicology, 2nd Edition)Antonio jose Garrido carvajalinoОценок пока нет
- Item 10 Part 2 Road Traffic AccidentДокумент32 страницыItem 10 Part 2 Road Traffic AccidentAkash KumarОценок пока нет
- Crash Injuries and DeathsДокумент98 страницCrash Injuries and DeathsPaul SalazarОценок пока нет
- EvanДокумент37 страницEvanVanz EstradaОценок пока нет
- Referat Transporation InjuriesДокумент6 страницReferat Transporation Injurieskoas jiwa ragaОценок пока нет
- Transport Accident InjuriesДокумент34 страницыTransport Accident InjuriesKaleem KhanОценок пока нет
- JullyДокумент21 страницаJullyJully Ann DumpitОценок пока нет
- Collision ModelДокумент14 страницCollision ModelIňñøcêñt Bøý AmanОценок пока нет
- Analysis of Vehicle CollisionsДокумент13 страницAnalysis of Vehicle CollisionsWestley SantiagoОценок пока нет
- Kinematics - Trauma Lesson PlanДокумент11 страницKinematics - Trauma Lesson PlanBethuel AliwaОценок пока нет
- Legal Med - Vehicular AccidentДокумент13 страницLegal Med - Vehicular Accidentralna_florano1467Оценок пока нет
- Material 2Документ5 страницMaterial 2tejuasha26Оценок пока нет
- 4 - MVA For DistributionДокумент65 страниц4 - MVA For DistributionCarl Christian V. DonaireОценок пока нет
- Motor Vehicle CollisionДокумент37 страницMotor Vehicle CollisionLouisse Angeli AbucejoОценок пока нет
- Legal Medicine-Chapter XI & XIXДокумент8 страницLegal Medicine-Chapter XI & XIXwichupinunoОценок пока нет
- Road Traffic Accident: Purpose of Medico-Legal InvestigationДокумент33 страницыRoad Traffic Accident: Purpose of Medico-Legal InvestigationAmirul AminОценок пока нет
- What Causes Traffic Accidents?: There Are Unsafe FactorsДокумент19 страницWhat Causes Traffic Accidents?: There Are Unsafe FactorsKelompok 9Оценок пока нет
- Blunt Trauma: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryДокумент87 страницBlunt Trauma: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryBarry JenkinsОценок пока нет
- Final Cdi4 13-14Документ9 страницFinal Cdi4 13-14Maria Frances MadrilejosОценок пока нет
- Death Due To Motor Vehicles: By: Ferryal BasbethДокумент19 страницDeath Due To Motor Vehicles: By: Ferryal BasbethodellistaОценок пока нет
- Pneumothorax & TBI Care After MVAДокумент36 страницPneumothorax & TBI Care After MVAdustin_camposОценок пока нет
- Week 11Документ7 страницWeek 11Ashley CastroОценок пока нет
- Types Of Accidents- Are In PlentyДокумент6 страницTypes Of Accidents- Are In PlentyRahul YadavОценок пока нет
- Man Made DisastersДокумент5 страницMan Made DisastersAbhishekОценок пока нет
- Encyclopedia of Forensic e Bookand Legal MedicineДокумент396 страницEncyclopedia of Forensic e Bookand Legal MedicineOla Dwi NandaОценок пока нет
- Repair 3Документ34 страницыRepair 3gobenashuguta180Оценок пока нет
- The Seven Most Common, High Cost Injuries: in Washington State 1998-2002Документ21 страницаThe Seven Most Common, High Cost Injuries: in Washington State 1998-2002Abi Walid Ibn SaatОценок пока нет
- Ea News Road Toll Presentation by Allyson and EmmaДокумент56 страницEa News Road Toll Presentation by Allyson and Emmaapi-331601417Оценок пока нет
- Common Injuries in Rear-End AccidentsДокумент4 страницыCommon Injuries in Rear-End AccidentsDuveen Mark ViernesОценок пока нет
- Dunlop Side Wall Bulge ExplanationДокумент1 страницаDunlop Side Wall Bulge ExplanationTarkeshwar RaoОценок пока нет
- Man Made DisasterДокумент31 страницаMan Made Disastersam 1Оценок пока нет
- Blunt Trauma: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryДокумент87 страницBlunt Trauma: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryGersonito SobreiraОценок пока нет
- Western Mindanao State University Traffic Accident Investigation ReportДокумент3 страницыWestern Mindanao State University Traffic Accident Investigation ReportNivla GenesisОценок пока нет
- Risk Management PlansДокумент3 страницыRisk Management Plansapi-272744607Оценок пока нет
- LP Trauma WajahДокумент24 страницыLP Trauma WajahDessy LestaryОценок пока нет
- April: Why Safety Belts?Документ1 страницаApril: Why Safety Belts?eastОценок пока нет
- Teenage Cyclist Injury Evaluation Using Multibody SimulationДокумент15 страницTeenage Cyclist Injury Evaluation Using Multibody SimulationSilvana BogićevićОценок пока нет
- Types of AccidentsДокумент2 страницыTypes of AccidentsWilliam CaleroОценок пока нет
- SF CAr Accident LawyersДокумент5 страницSF CAr Accident LawyersMona DeldarОценок пока нет
- Lesson 17Документ32 страницыLesson 17Bijendra SharmaОценок пока нет
- Forensic Assessment of Trauma Injuries in The Interior of A Moving Passenger Car Equipped With Modern Safety FeaturesДокумент5 страницForensic Assessment of Trauma Injuries in The Interior of A Moving Passenger Car Equipped With Modern Safety FeaturesCentral Asian StudiesОценок пока нет
- Vehicle rescue techniquesДокумент20 страницVehicle rescue techniquesSteve TalbotОценок пока нет
- What Are Common Causes of Injuries On Public Transportation?Документ2 страницыWhat Are Common Causes of Injuries On Public Transportation?GayFleur Cabatit RamosОценок пока нет
- Construction Project Management: Unit 8: SafetyДокумент9 страницConstruction Project Management: Unit 8: SafetyGirman ranaОценок пока нет
- International Journal of Health Sciences and ResearchДокумент6 страницInternational Journal of Health Sciences and ResearchMARINAОценок пока нет
- Physics Assessment 3 Year 11 - Vehicle Safety BeltsДокумент5 страницPhysics Assessment 3 Year 11 - Vehicle Safety Beltsparacin8131Оценок пока нет
- Causes of Car AccidentsДокумент4 страницыCauses of Car AccidentsfebbarbieОценок пока нет
- Motorcycle Accident ClaimsДокумент6 страницMotorcycle Accident ClaimsGary E. Rosenberg100% (2)
- 5 - Blunt Trauma WoundsДокумент141 страница5 - Blunt Trauma WoundsWala AbdeljawadОценок пока нет
- Construction Project Management: Unit 8: Safety 4hrsДокумент9 страницConstruction Project Management: Unit 8: Safety 4hrsGirman RanaОценок пока нет
- Fraudulent Vehicle Damages ClaimsДокумент13 страницFraudulent Vehicle Damages ClaimsJosé sergio M costaОценок пока нет
- Crash CourseДокумент10 страницCrash Coursenagarjun_singhОценок пока нет
- Head Injury Rupani3Документ203 страницыHead Injury Rupani3Anonymous udSI3fQ5Оценок пока нет
- Facial Trauma: Episode OverviewДокумент6 страницFacial Trauma: Episode OverviewJoko SantosoОценок пока нет
- Masonry, Tile, Terrazzo, and Allied Trades: Health & Safety GuideДокумент48 страницMasonry, Tile, Terrazzo, and Allied Trades: Health & Safety GuideSonu KrishnaОценок пока нет
- Quarterly Report On Case FindingДокумент2 страницыQuarterly Report On Case FindingTrishenth FonsekaОценок пока нет
- Quarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseДокумент1 страницаQuarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseTrishenth FonsekaОценок пока нет
- National TB Control ManualДокумент223 страницыNational TB Control ManualTrishenth FonsekaОценок пока нет
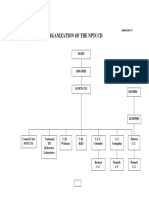
- Organization of NPTCCD PDFДокумент2 страницыOrganization of NPTCCD PDFTrishenth FonsekaОценок пока нет
- Quarterly Report On TB and non-TB WardsДокумент3 страницыQuarterly Report On TB and non-TB WardsTrishenth FonsekaОценок пока нет
- Duties of MOHДокумент3 страницыDuties of MOHTrishenth FonsekaОценок пока нет
- Register of TB SuspectsДокумент1 страницаRegister of TB SuspectsTrishenth FonsekaОценок пока нет
- Quarterly Report On Microscopic Activities and LogisticsДокумент2 страницыQuarterly Report On Microscopic Activities and LogisticsTrishenth FonsekaОценок пока нет
- Quarterly Report On Program ManagementДокумент7 страницQuarterly Report On Program ManagementTrishenth FonsekaОценок пока нет
- Quarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierДокумент2 страницыQuarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierTrishenth FonsekaОценок пока нет
- National TB RegisterДокумент2 страницыNational TB RegisterTrishenth FonsekaОценок пока нет
- Laborotory Manual For Tuberculosis ControlДокумент5 страницLaborotory Manual For Tuberculosis ControlTrishenth FonsekaОценок пока нет
- Living With AFib Patient GuideДокумент73 страницыLiving With AFib Patient GuideTrishenth FonsekaОценок пока нет
- Lab Form For Sputum Examination PDFДокумент1 страницаLab Form For Sputum Examination PDFTrishenth FonsekaОценок пока нет
- The Premature BabyДокумент92 страницыThe Premature BabyTrishenth Fonseka100% (1)
- 29 - Heart Disease Complicating PregnancyДокумент18 страниц29 - Heart Disease Complicating PregnancyTrishenth FonsekaОценок пока нет
- SLEДокумент42 страницыSLETrishenth FonsekaОценок пока нет
- QuotesДокумент1 страницаQuotesTrishenth FonsekaОценок пока нет
- Paediatric UrologyДокумент194 страницыPaediatric UrologyTrishenth FonsekaОценок пока нет
- Neck Pain and Pain Down The ArmДокумент27 страницNeck Pain and Pain Down The ArmTrishenth FonsekaОценок пока нет
- 12 - Medical NegligenceДокумент34 страницы12 - Medical NegligenceTrishenth FonsekaОценок пока нет
- 15 - CN Poisoning 2Документ2 страницы15 - CN Poisoning 2Trishenth FonsekaОценок пока нет
- Medical Ethics Code ExplainedДокумент23 страницыMedical Ethics Code ExplainedTrishenth FonsekaОценок пока нет
- Gas Poisoning (Irrespirable Gases) : Asphyxial DeathДокумент5 страницGas Poisoning (Irrespirable Gases) : Asphyxial DeathTrishenth FonsekaОценок пока нет
- 11 - Professional SecrecyДокумент10 страниц11 - Professional SecrecyTrishenth Fonseka100% (1)
- 08 - Post Mortem InstrumentsДокумент6 страниц08 - Post Mortem InstrumentsTrishenth FonsekaОценок пока нет
- 13 - Medicolegal Duties of A DoctorДокумент13 страниц13 - Medicolegal Duties of A DoctorTrishenth FonsekaОценок пока нет
- SLMC - Regulating Sri Lanka's Medical ProfessionДокумент27 страницSLMC - Regulating Sri Lanka's Medical ProfessionTrishenth FonsekaОценок пока нет
- 10 - Introduction To Legal System in SLДокумент6 страниц10 - Introduction To Legal System in SLTrishenth FonsekaОценок пока нет
- 09 - Changes After Death and Time Since DeathДокумент9 страниц09 - Changes After Death and Time Since DeathTrishenth FonsekaОценок пока нет
- Improving Public Transportation Safety and Security in Developing NationsДокумент15 страницImproving Public Transportation Safety and Security in Developing NationsAslamia RosaОценок пока нет
- Road Accident Analysis and Prediction of Accident Severity by Using Machine Learning in BangladeshДокумент6 страницRoad Accident Analysis and Prediction of Accident Severity by Using Machine Learning in Bangladeshprabhu chand alluriОценок пока нет
- Safe Operation of ForkliftsДокумент71 страницаSafe Operation of Forkliftsashishmechengg31100% (1)
- (Cranes)Документ60 страниц(Cranes)Th NattapongОценок пока нет
- Important Judgements Under MV Act PDFДокумент125 страницImportant Judgements Under MV Act PDFAnonymous W6nTqJg4Оценок пока нет
- Forensic Examination of VehiclesДокумент3 страницыForensic Examination of VehicleskrishnaОценок пока нет
- Vehicle Pre Purchase Inspection Checklist TemplateДокумент13 страницVehicle Pre Purchase Inspection Checklist TemplateManish KumarОценок пока нет
- CDIДокумент59 страницCDIDioner RayОценок пока нет
- American National Standard Ansi - D.16-2017Документ84 страницыAmerican National Standard Ansi - D.16-2017aymen ismailОценок пока нет
- English For Non-Commissioned Security Officers Words ListДокумент7 страницEnglish For Non-Commissioned Security Officers Words ListIbrahim KurdiОценок пока нет
- 121212baseline Risk Assessment - Matla 2 School Rev00Документ34 страницы121212baseline Risk Assessment - Matla 2 School Rev00Vepxvia NadiradzeОценок пока нет
- ECall Type-Approval - TRL Client Project Report CPR1868Документ206 страницECall Type-Approval - TRL Client Project Report CPR1868Mutually Exclusive, Collectively ExhaustiveОценок пока нет
- RISK ASSESSMENT FORM FOR POTABLE WATER WORKSДокумент44 страницыRISK ASSESSMENT FORM FOR POTABLE WATER WORKSloveson709Оценок пока нет
- OSHA ChecklistДокумент2 страницыOSHA ChecklistCésar Augusto Quiroga MontenegroОценок пока нет
- Motor Vehicle StandardДокумент16 страницMotor Vehicle StandardAnonymous cligbBAXОценок пока нет
- Level 10 Passage 4Документ3 страницыLevel 10 Passage 4JefaradocsОценок пока нет
- Apron Safety ProceduresДокумент20 страницApron Safety ProceduresSankar CdmОценок пока нет
- Project Report On National Highways: Dhanavath Seva, Bhukya Chandrashekar, Faria AseemДокумент10 страницProject Report On National Highways: Dhanavath Seva, Bhukya Chandrashekar, Faria Aseemआशीष खोखरОценок пока нет
- MLA Format Research Paper Outline (Example 2)Документ8 страницMLA Format Research Paper Outline (Example 2)Jonathan BrantleyОценок пока нет
- Progress Report Proactive Safety Culture in ConstructionДокумент7 страницProgress Report Proactive Safety Culture in ConstructionIcizacky Ishaq100% (1)
- Road Accident Prediction Model Using Data Mining TechniquesДокумент6 страницRoad Accident Prediction Model Using Data Mining Techniquesranjan100% (1)
- An Exploratory Multinomial Logit Analysis of Single-Vehicle Motorcycle Accident SeverityДокумент12 страницAn Exploratory Multinomial Logit Analysis of Single-Vehicle Motorcycle Accident SeverityRidwan Bin AlamОценок пока нет
- Yamaha FZ6S1 Owners ManualДокумент90 страницYamaha FZ6S1 Owners ManualmateinicoletaОценок пока нет
- Road Safety in the PhilippinesДокумент6 страницRoad Safety in the PhilippinesTrang QuỳnhОценок пока нет
- IoT Applications in HealthcareДокумент63 страницыIoT Applications in Healthcarezankhana vaishnavОценок пока нет
- Cambridge Ordinary LevelДокумент4 страницыCambridge Ordinary LevelHaziq AfzalОценок пока нет
- Construction Health and Safety in South Africa PDFДокумент48 страницConstruction Health and Safety in South Africa PDFAndile Ntuli100% (2)
- Safety and Security HRMДокумент12 страницSafety and Security HRMHasrizam86Оценок пока нет
- Can Gun Control WorkДокумент304 страницыCan Gun Control WorkMiroslav MaksimovićОценок пока нет
- Discussion TextДокумент3 страницыDiscussion TextJefri Lumban GaolОценок пока нет