Вам также может понравиться
- Why Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniaДокумент10 страницWhy Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniajlventiganОценок пока нет
- 2019 Article 1588Документ9 страниц2019 Article 1588RieWibawaОценок пока нет
- Factors Associated With Stunting Among Children of Age 24 To 59 Months in Meskan District, Gurage Zone, South Ethiopia: A Case-Control StudyДокумент7 страницFactors Associated With Stunting Among Children of Age 24 To 59 Months in Meskan District, Gurage Zone, South Ethiopia: A Case-Control Studyfio rentiniОценок пока нет
- Effectiveness of Integrated Nutrition Interventions On Childhood Stunting: A Quasi-Experimental Evaluation DesignДокумент15 страницEffectiveness of Integrated Nutrition Interventions On Childhood Stunting: A Quasi-Experimental Evaluation DesignMd UmerОценок пока нет
- FinalДокумент25 страницFinalabdu seidОценок пока нет
- Prevalence and Correlates of HIV Testing Among Adolescents 10 - 19 Years in A Post-Conflict Pastoralist Community of Karamoja Region, UgandaДокумент8 страницPrevalence and Correlates of HIV Testing Among Adolescents 10 - 19 Years in A Post-Conflict Pastoralist Community of Karamoja Region, UgandaFaisal HarisОценок пока нет
- Ijerph 09 03506 PDFДокумент13 страницIjerph 09 03506 PDFAdriana RojasОценок пока нет
- Trends in Prevalence and Determinants of Stunting in Tanzania: An Analysis of Tanzania Demographic Health Surveys (1991 - 2016)Документ13 страницTrends in Prevalence and Determinants of Stunting in Tanzania: An Analysis of Tanzania Demographic Health Surveys (1991 - 2016)assyifatuhaifa607Оценок пока нет
- 2020 Article 5485Документ8 страниц2020 Article 5485marikum74Оценок пока нет
- Research ArticleДокумент13 страницResearch ArticleDENNYОценок пока нет
- Cross Sectional Study On Wheezing Dis and Factors AssociatedДокумент9 страницCross Sectional Study On Wheezing Dis and Factors AssociatedTandin SonamОценок пока нет
- Factors Influencing Teenage Pregnancy Among Girls Attending Kampala International University Teaching Hospital, Bushenyi, UgandaДокумент12 страницFactors Influencing Teenage Pregnancy Among Girls Attending Kampala International University Teaching Hospital, Bushenyi, UgandaKIU PUBLICATION AND EXTENSIONОценок пока нет
- Diare Etyopia PDF - 2017Документ8 страницDiare Etyopia PDF - 2017Anonymous WkBXZB2UaОценок пока нет
- 2017 Article 2060Документ8 страниц2017 Article 2060Indira SellyОценок пока нет
- Determinants of Stunting in inДокумент3 страницыDeterminants of Stunting in inNur UfiyaОценок пока нет
- 2020 Article 5324Документ8 страниц2020 Article 5324Sorina ElenaОценок пока нет
- Association Between Maternal Depression and Child Stunting in Northern Ghana: A Cross-Sectional StudyДокумент7 страницAssociation Between Maternal Depression and Child Stunting in Northern Ghana: A Cross-Sectional StudySellymarlinaleeОценок пока нет
- Determinants of Stunting and Severe Stunting Among Under-Fives: Evidence From The 2011 Nepal Demographic and Health SurveyДокумент15 страницDeterminants of Stunting and Severe Stunting Among Under-Fives: Evidence From The 2011 Nepal Demographic and Health SurveyNIRMALAОценок пока нет
- 2018 Article 5561Документ8 страниц2018 Article 5561andinurzamzamОценок пока нет
- Taremwa 2017Документ8 страницTaremwa 2017GianОценок пока нет
- Essential Newborn Care Practice at Four Primary Health Facilities in Conflict Affected Areas of Bossaso Somalia A Cross Sectional StudyДокумент13 страницEssential Newborn Care Practice at Four Primary Health Facilities in Conflict Affected Areas of Bossaso Somalia A Cross Sectional StudyROBLE ABDIОценок пока нет
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyДокумент10 страницDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaОценок пока нет
- Midwives' Intrapartum Monitoring Process and Management Resulting in Emergency Referrals in TanzaniaДокумент11 страницMidwives' Intrapartum Monitoring Process and Management Resulting in Emergency Referrals in TanzaniaAdhiw AmanОценок пока нет
- ResearchДокумент11 страницResearchPaulОценок пока нет
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoДокумент20 страницMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriОценок пока нет
- Chapter One 1.1 Background To The StudyДокумент59 страницChapter One 1.1 Background To The StudyOpeyemi Abdulmojeed OmotoshoОценок пока нет
- JURNAL Adolescent Pregnancy 13Документ8 страницJURNAL Adolescent Pregnancy 13elisabethОценок пока нет
- Neonatal Mortality and Associated FactorsДокумент9 страницNeonatal Mortality and Associated FactorsmeryОценок пока нет
- IMCIДокумент131 страницаIMCIRhod Bernaldez EstaОценок пока нет
- Research Article: Prevalence and Predictors of Stunting Among Primary School Children in Northeast EthiopiaДокумент8 страницResearch Article: Prevalence and Predictors of Stunting Among Primary School Children in Northeast Ethiopiarezky_tdОценок пока нет
- 2022 Article 1347Документ10 страниц2022 Article 1347alifa9393Оценок пока нет
- Vitamin-A Deficiency and Its Determinants Among PRДокумент9 страницVitamin-A Deficiency and Its Determinants Among PRaizah afifaturОценок пока нет
- 2018 Article 260Документ8 страниц2018 Article 260yanuartip87Оценок пока нет
- Factors Influencing The Use of Antenatal Care in Rural West Sumatra, IndonesiaДокумент8 страницFactors Influencing The Use of Antenatal Care in Rural West Sumatra, IndonesiapebripulunganОценок пока нет
- 01RE-Manuscript Elonge Halle Adolescent Pregnancy - Manuscript-04 O6-2020Документ18 страниц01RE-Manuscript Elonge Halle Adolescent Pregnancy - Manuscript-04 O6-2020Cretze IsahОценок пока нет
- Exploring Women Knowledge of Newborn Danger Signs: A Case of Mothers With Under Five ChildrenДокумент8 страницExploring Women Knowledge of Newborn Danger Signs: A Case of Mothers With Under Five ChildrenJohnjohn MateoОценок пока нет
- Prevalence and Factors Associated With Intestinal Parasites Among Children of Age 6 To 59 Months In, Boricha District, South Ethiopia, in 2018Документ7 страницPrevalence and Factors Associated With Intestinal Parasites Among Children of Age 6 To 59 Months In, Boricha District, South Ethiopia, in 2018Mirtha AnggraeniОценок пока нет
- Breastfeeding Counseling and SupportДокумент8 страницBreastfeeding Counseling and SupportJohanna MoralesОценок пока нет
- Essential Newborn Care Practices and Associated Factors Among Home Delivered Mothers in Damot Pulasa Woreda, Southern EthiopiaДокумент11 страницEssential Newborn Care Practices and Associated Factors Among Home Delivered Mothers in Damot Pulasa Woreda, Southern EthiopiaalchmistОценок пока нет
- National Health Insurance Subscription and Maternal Healthcare Utilization Across Mothers' Wealth Status in Ghana. Health Economics ReviewДокумент16 страницNational Health Insurance Subscription and Maternal Healthcare Utilization Across Mothers' Wealth Status in Ghana. Health Economics ReviewRaymond ElikplimОценок пока нет
- Tropical Med Int Health - 2019 - Finlay - Sexual and Reproductive Health Knowledge Among Adolescents in Eight Sites AcrossДокумент10 страницTropical Med Int Health - 2019 - Finlay - Sexual and Reproductive Health Knowledge Among Adolescents in Eight Sites AcrossAhmed AbbasОценок пока нет
- Jurnal INT 5Документ10 страницJurnal INT 5Ratu Delima PuspitaОценок пока нет
- Lencho 3Документ41 страницаLencho 3mohammed abdellaОценок пока нет
- Lyellu2020 Article PrevalenceAndFactorsAssociatedДокумент10 страницLyellu2020 Article PrevalenceAndFactorsAssociatedyossy ramadhaniОценок пока нет
- Healthcare-Seeking Behavior For Children Aged 0-59Документ17 страницHealthcare-Seeking Behavior For Children Aged 0-59stevy ariskaОценок пока нет
- Strengthening Integrated Primary Health Care in Sofala, MozambiqueДокумент12 страницStrengthening Integrated Primary Health Care in Sofala, MozambiqueRoger langaОценок пока нет
- Jurnal 08Документ9 страницJurnal 08Jojo McalisterОценок пока нет
- Abera2017 Prevalence of Malnutrition and Associated Factors in EthiopiaДокумент8 страницAbera2017 Prevalence of Malnutrition and Associated Factors in EthiopiaSHILPA PATILОценок пока нет
- 2013 Article 326Документ8 страниц2013 Article 326Ariyati MandiriОценок пока нет
- Utilisation of Health Services and The Poor: Deconstructing Wealth-Based Differences in Facility-Based Delivery in The PhilippinesДокумент12 страницUtilisation of Health Services and The Poor: Deconstructing Wealth-Based Differences in Facility-Based Delivery in The PhilippinesBrix ValdrizОценок пока нет
- Malnutrition-Journal WДокумент11 страницMalnutrition-Journal Wgeng gengОценок пока нет
- Health Policy Plan. 2009 Kruk 279 88Документ10 страницHealth Policy Plan. 2009 Kruk 279 88jlventiganОценок пока нет
- Final Copy (Tipdas) 111Документ80 страницFinal Copy (Tipdas) 111Zachary Bañez100% (1)
- Assessment of The Incidence and Contributing Factors of Diarrheal Episodes in Children Under Five Years Admitted To Hoima Regional Referral HospiДокумент13 страницAssessment of The Incidence and Contributing Factors of Diarrheal Episodes in Children Under Five Years Admitted To Hoima Regional Referral HospiKIU PUBLICATION AND EXTENSIONОценок пока нет
- Journal Pre-Proof: Clinical Epidemiology and Global HealthДокумент22 страницыJournal Pre-Proof: Clinical Epidemiology and Global HealthClaudia BuheliОценок пока нет
- Evaluation of Male Partner Participation in Prevention of Mother To Child Transmission of HIVAIDs at Hoima Referral HospitalДокумент14 страницEvaluation of Male Partner Participation in Prevention of Mother To Child Transmission of HIVAIDs at Hoima Referral HospitalKIU PUBLICATION AND EXTENSIONОценок пока нет
- 2017 Article 2184Документ11 страниц2017 Article 2184diana sulistianОценок пока нет
- Out 17Документ10 страницOut 17laodesyuhadarОценок пока нет
- Related-LitДокумент4 страницыRelated-LitBianca Alexy MataОценок пока нет
- Child Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsОт EverandChild Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsОценок пока нет
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyДокумент10 страницDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaОценок пока нет
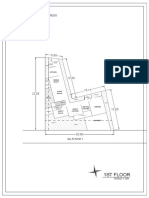
- 1St Floor: House On Paus Schematic Plan ProgressДокумент2 страницы1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaОценок пока нет
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyДокумент11 страницSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaОценок пока нет
- 2015 Conference 10Документ11 страниц2015 Conference 10fiora.ladesvitaОценок пока нет
- Medicalscience: EcancerДокумент7 страницMedicalscience: Ecancerfiora.ladesvitaОценок пока нет
- Gibson 2010Документ19 страницGibson 2010fiora.ladesvitaОценок пока нет
- Ambulatory Care Nursing: Coming Soon!Документ16 страницAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaОценок пока нет
- Sistematic Review HoneyДокумент159 страницSistematic Review Honeyfiora.ladesvitaОценок пока нет
- Assessment Rating ScaleДокумент8 страницAssessment Rating Scalefiora.ladesvitaОценок пока нет
- Anderson2004 PDFДокумент7 страницAnderson2004 PDFfiora.ladesvitaОценок пока нет
- Living With Kidney DiseaseДокумент96 страницLiving With Kidney Diseasefiora.ladesvitaОценок пока нет
- Caring: Prof. Dr. Budi Anna Keliat, MappscДокумент59 страницCaring: Prof. Dr. Budi Anna Keliat, Mappscfiora.ladesvitaОценок пока нет
- Idiom Meaning Examples: Toefl PreparationДокумент4 страницыIdiom Meaning Examples: Toefl Preparationfiora.ladesvitaОценок пока нет
- AH1N1 PPT PresentationДокумент28 страницAH1N1 PPT PresentationIna Isabela CostiboloОценок пока нет
- Cot q2 w5 HEALTH (New Normal CO)Документ4 страницыCot q2 w5 HEALTH (New Normal CO)lizaОценок пока нет
- Shape Up BusyBee CarysДокумент16 страницShape Up BusyBee CarysElena HorodincaОценок пока нет
- Core CompetencyДокумент9 страницCore CompetencyCharm BarinosОценок пока нет
- Sutured Wound Care InstructionsДокумент2 страницыSutured Wound Care InstructionsPreet Inder SinghОценок пока нет
- Nitroimidazole Wps OfficeДокумент10 страницNitroimidazole Wps OfficeCamelle DiniayОценок пока нет
- MSDS PDFДокумент5 страницMSDS PDFdang2172014Оценок пока нет
- Ahimajournal 2015 04 DLДокумент93 страницыAhimajournal 2015 04 DLDarrin OpdyckeОценок пока нет
- 21.JMM Promotion and Management, Inc. vs. Court of AppealsДокумент3 страницы21.JMM Promotion and Management, Inc. vs. Court of AppealsnathОценок пока нет
- Health 8 Q3 Week 7-8 Module 1-6Документ22 страницыHealth 8 Q3 Week 7-8 Module 1-6Richard CoderiasОценок пока нет
- Infant Tub RationaleДокумент4 страницыInfant Tub RationaleAllen Kenneth PacisОценок пока нет
- Agility For FootballДокумент42 страницыAgility For Footballpflucho100% (2)
- Labor and Delivery OB Concept MapДокумент2 страницыLabor and Delivery OB Concept MapMissy Johnson75% (4)
- 2005 Proverbs TOM SchizophreniaДокумент7 страниц2005 Proverbs TOM SchizophreniaKatsiaryna HurbikОценок пока нет
- Discursive StudiesДокумент11 страницDiscursive StudiesSohag LTCОценок пока нет
- An Atlas of Radiology of The Traumatized Dog and CatДокумент566 страницAn Atlas of Radiology of The Traumatized Dog and CatDenise Gomes de MeloОценок пока нет
- Fitness JournalДокумент68 страницFitness JournalKrisztinaVágvölgyiОценок пока нет
- Week 4.1 The Law of ResonanceДокумент12 страницWeek 4.1 The Law of ResonanceWim Massop100% (1)
- HCM 239Документ199 страницHCM 239Mohit VermaОценок пока нет
- Answers To Questions: Earl John E. CañoneroДокумент2 страницыAnswers To Questions: Earl John E. CañoneroEarl CañoneroОценок пока нет
- NIH Heat Stress ProgramДокумент10 страницNIH Heat Stress ProgramHarthwell CapistranoОценок пока нет
- Official ResumeДокумент1 страницаOfficial ResumeBrianna DallalОценок пока нет
- SR.# Weight (KG) Height (FT) Age (Yrz) Others RecommendationsДокумент2 страницыSR.# Weight (KG) Height (FT) Age (Yrz) Others RecommendationsshaniОценок пока нет
- ETW-2013 Amma PDFДокумент100 страницETW-2013 Amma PDFRosalete LimaОценок пока нет
- Craniofacial SyndromesДокумент101 страницаCraniofacial SyndromesSaranya MohanОценок пока нет
- Written Assignment Unit 2 - HS 2212Документ5 страницWritten Assignment Unit 2 - HS 2212bnvjОценок пока нет
- Experiment 9 - Hydrolysis of CarbohydratesДокумент2 страницыExperiment 9 - Hydrolysis of CarbohydratesJuren LasagaОценок пока нет
- BLS Provider: Ma. Carmela C. VasquezДокумент2 страницыBLS Provider: Ma. Carmela C. VasquezPatricia VasquezОценок пока нет
- Nutritional Interventions PDFДокумент17 страницNutritional Interventions PDFLalit MittalОценок пока нет
- Human Resource ManagementДокумент8 страницHuman Resource ManagementSyed HoqueОценок пока нет