Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Anesthesiology Resident Survival Guide 2014-2015Документ32 страницыAnesthesiology Resident Survival Guide 2014-2015Karla Matos100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Meridians and Points PDFДокумент35 страницMeridians and Points PDFHamdon Hamad100% (9)
- MRCP 2 Nephrology NOTESДокумент74 страницыMRCP 2 Nephrology NOTESMuhammad HaneefОценок пока нет
- Levels of Academic Stress Among Senior High School Scholar Students of The Mabini AcademyДокумент18 страницLevels of Academic Stress Among Senior High School Scholar Students of The Mabini AcademyRaymond Lomerio100% (1)
- Lesson 6 - Musculoskeletal and Nervous SystemsДокумент20 страницLesson 6 - Musculoskeletal and Nervous Systemsapi-307592530Оценок пока нет
- Nursing Care Plan for CVA Bleeding PatientДокумент3 страницыNursing Care Plan for CVA Bleeding PatientpaulaОценок пока нет
- H2S Training Slides ENGLISHДокумент46 страницH2S Training Slides ENGLISHf.B100% (1)
- Megalourethra: A Rare Clinical Entity: ReferencesДокумент1 страницаMegalourethra: A Rare Clinical Entity: Referencesdella psОценок пока нет
- Congenital scaphoid megalourethra: Report of two rare casesДокумент3 страницыCongenital scaphoid megalourethra: Report of two rare casesdella psОценок пока нет
- Di Bianco 1989Документ7 страницDi Bianco 1989della psОценок пока нет
- Loftus 2016Документ8 страницLoftus 2016della psОценок пока нет
- Cranberry EditorialДокумент2 страницыCranberry EditorialKorina LimnioudiОценок пока нет
- Epidemiology of Asthma: ReviewДокумент5 страницEpidemiology of Asthma: Reviewdella psОценок пока нет
- Guay 2009Документ33 страницыGuay 2009della psОценок пока нет
- Long-Term Outcomes and Risk Factors Associated With Acute Encephalitis in ChildrenДокумент8 страницLong-Term Outcomes and Risk Factors Associated With Acute Encephalitis in ChildrenNovia RambakОценок пока нет
- Yokoyama 2000Документ5 страницYokoyama 2000della psОценок пока нет
- An Investigation of Dentists' Knowledge, Attitudes and Practices Towards HIV and Patients With Other Blood-Borne Viruses in South Cheshire, UKДокумент6 страницAn Investigation of Dentists' Knowledge, Attitudes and Practices Towards HIV and Patients With Other Blood-Borne Viruses in South Cheshire, UKdella psОценок пока нет
- Patfis AsmaДокумент14 страницPatfis Asmadella psОценок пока нет
- Patfis Asma 2Документ10 страницPatfis Asma 2della psОценок пока нет
- Review ArticleДокумент8 страницReview Articledella psОценок пока нет
- JAMA. 2016 : in ReplyДокумент3 страницыJAMA. 2016 : in Replydella psОценок пока нет
- Paradigms of Oxygen Therapy in Critically Ill PatientsДокумент6 страницParadigms of Oxygen Therapy in Critically Ill Patientsdella psОценок пока нет
- Girard Is 2016Документ7 страницGirard Is 2016della psОценок пока нет
- Oxygen: Breath of Life or Kiss of DeathДокумент2 страницыOxygen: Breath of Life or Kiss of Deathdella psОценок пока нет
- Oxygen in The ICU Too Much of A Good Thing?: EditorialДокумент2 страницыOxygen in The ICU Too Much of A Good Thing?: Editorialdella psОценок пока нет
- Suzuki 2014Документ9 страницSuzuki 2014della psОценок пока нет
- Pan War 2016Документ51 страницаPan War 2016della psОценок пока нет
- Caumes Et Al-2004-Journal of Travel Medicine PDFДокумент3 страницыCaumes Et Al-2004-Journal of Travel Medicine PDFdella psОценок пока нет
- Kal Let 2016Документ17 страницKal Let 2016della psОценок пока нет
- Placental Disease and The Maternal Syndrome of Preeclampsia: Missing Links?Документ10 страницPlacental Disease and The Maternal Syndrome of Preeclampsia: Missing Links?della psОценок пока нет
- Oxygen in The Critically Ill: Friend or Foe?: ReviewДокумент7 страницOxygen in The Critically Ill: Friend or Foe?: Reviewdella psОценок пока нет
- Epidemiology of Asthma: ReviewДокумент5 страницEpidemiology of Asthma: Reviewdella psОценок пока нет
- Low-Dose Digoxin May Benefit Heart Failure Patients on DialysisДокумент6 страницLow-Dose Digoxin May Benefit Heart Failure Patients on Dialysisdella psОценок пока нет
- PNPK PreEklampsia 2016Документ7 страницPNPK PreEklampsia 2016della psОценок пока нет
- Placental Origins of Preeclampsia: Challenging The Current HypothesisДокумент7 страницPlacental Origins of Preeclampsia: Challenging The Current Hypothesisdella psОценок пока нет
- Renal Hemodynamics During Carbon Dioxide Pneumoperitoneum: An Experimental Study in PigsДокумент5 страницRenal Hemodynamics During Carbon Dioxide Pneumoperitoneum: An Experimental Study in Pigsdella psОценок пока нет
- Biology: Revised Syllabus For Higher Secondary First Year CourseДокумент4 страницыBiology: Revised Syllabus For Higher Secondary First Year CourseamitumikoibОценок пока нет
- Vit CДокумент10 страницVit C3/2 no.34 สรัญญากร สีหาราชОценок пока нет
- Electrolyte Imbalance 1Документ3 страницыElectrolyte Imbalance 1Marius Clifford BilledoОценок пока нет
- Neurodegenerative Cerebellar AtaxiaДокумент26 страницNeurodegenerative Cerebellar AtaxiaМилица МилошевићОценок пока нет
- 16th Week of Pregnancy: Tips for Safe Travel While ExpectingДокумент4 страницы16th Week of Pregnancy: Tips for Safe Travel While ExpectingNaveenbabu SoundararajanОценок пока нет
- LAB EXERCISE 1 Organization of The Human BodyДокумент8 страницLAB EXERCISE 1 Organization of The Human Bodyley leynОценок пока нет
- q3 Sci10 Unit1 Feedback MechanismsДокумент125 страницq3 Sci10 Unit1 Feedback MechanismsIvann EboraОценок пока нет
- A Kinesiological Analysis of Shot BY WILLISДокумент16 страницA Kinesiological Analysis of Shot BY WILLISNoraina AbdullahОценок пока нет
- Amniodarone (Norvasc) Drug SummДокумент1 страницаAmniodarone (Norvasc) Drug SummWarrenОценок пока нет
- Posture and AlignmentДокумент1 страницаPosture and AlignmentNell KeeneОценок пока нет
- The Normal Anterior Inferior Cerebellar ArteryДокумент19 страницThe Normal Anterior Inferior Cerebellar Artery16fernandoОценок пока нет
- B2 Revision PIXLДокумент26 страницB2 Revision PIXLtunmishetobilawalОценок пока нет
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskДокумент8 страницTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaОценок пока нет
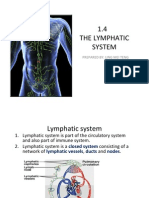
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengДокумент15 страниц1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingОценок пока нет
- Manajemen Pre-Operatif Pasien Dengan DMДокумент12 страницManajemen Pre-Operatif Pasien Dengan DMyanayas28Оценок пока нет
- Left Posterior Fascicular BlockДокумент4 страницыLeft Posterior Fascicular BlockFathimah afifah zahrahОценок пока нет
- 3 9 1 bMSDS-Reagen-LaboratoriumДокумент4 страницы3 9 1 bMSDS-Reagen-Laboratoriumswahyulisah100% (1)
- CP On AmoebiasisДокумент77 страницCP On Amoebiasiskathy100% (1)
- Point MarmaДокумент2 страницыPoint MarmaAnonymous yzbnd8Оценок пока нет
- CH4106 Formulation Module GuideДокумент29 страницCH4106 Formulation Module GuideWeimingTanОценок пока нет
- The Anterior Cranial FossaДокумент4 страницыThe Anterior Cranial FossaArshad hussainОценок пока нет
- Overview of Complications Occurring in The Post-Anesthesia Care UnitДокумент14 страницOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhОценок пока нет