Вам также может понравиться
- What Is InfluenzaДокумент4 страницыWhat Is InfluenzamatorrecОценок пока нет
- Flu Treatment, Symptoms, Shot, Causes & Cold Vs FluДокумент22 страницыFlu Treatment, Symptoms, Shot, Causes & Cold Vs FluLeanne TehОценок пока нет
- A Simple Guide To Pandemics, Diagnosis, Treatment And Related ConditionsОт EverandA Simple Guide To Pandemics, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Lecture 2: Upper Respiratory Tract Viral Infection Ifluenza & ProphylaxisДокумент11 страницLecture 2: Upper Respiratory Tract Viral Infection Ifluenza & ProphylaxisParisa PourkhosrowОценок пока нет
- Mode of TransmissionДокумент7 страницMode of TransmissionPrexiedes WaswaОценок пока нет
- Use Various Resources To Find The Answers To The Questions BelowДокумент3 страницыUse Various Resources To Find The Answers To The Questions BelowNicole SanchezОценок пока нет
- By Niharika Sharma Prabhakar Kumar Under The Guidance of K.K Ojha (B.H.U)Документ17 страницBy Niharika Sharma Prabhakar Kumar Under The Guidance of K.K Ojha (B.H.U)Prabhakar KumarОценок пока нет
- The Bird Flu and YouДокумент15 страницThe Bird Flu and YouMahogony ScottОценок пока нет
- Swine FluДокумент34 страницыSwine FlusayedmОценок пока нет
- InfluenzaДокумент30 страницInfluenzaHb KamalОценок пока нет
- Pandemic Preparedness HandoutДокумент30 страницPandemic Preparedness Handoutsnidely_whiplashОценок пока нет
- A (H1N1)Документ3 страницыA (H1N1)vincesumergidoОценок пока нет
- InfluenzaДокумент16 страницInfluenzaTrue AlphaОценок пока нет
- UK Prof Influenza Conditon LeafletДокумент7 страницUK Prof Influenza Conditon LeafletsuryaОценок пока нет
- Classification:: Influenza, Commonly Referred To As The Flu, Is An Infectious Disease Caused by RNA Viruses ofДокумент6 страницClassification:: Influenza, Commonly Referred To As The Flu, Is An Infectious Disease Caused by RNA Viruses ofSi VeekeeОценок пока нет
- H1N1 Flu Virus (Swine Flu)Документ4 страницыH1N1 Flu Virus (Swine Flu)Louise OpinaОценок пока нет
- Cold and Flu OverviewДокумент2 страницыCold and Flu Overviewdinesh11rОценок пока нет
- Clinical Review: Influenza Pandemics and Avian FluДокумент4 страницыClinical Review: Influenza Pandemics and Avian FluRatna SariyatunОценок пока нет
- C CCCC CC CCCДокумент18 страницC CCCC CC CCCRichard QuiochoОценок пока нет
- Seasonal Influenza Awareness Guide 2023 2024.aspxДокумент7 страницSeasonal Influenza Awareness Guide 2023 2024.aspxzarishnaveedОценок пока нет
- Spread The Message of Swine Flu To EveryoneДокумент3 страницыSpread The Message of Swine Flu To EveryoneDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU PhilippinesОценок пока нет
- Bacterial InfectionsДокумент20 страницBacterial InfectionsFahad RasheedОценок пока нет
- Assignment 3Документ3 страницыAssignment 3EurydiceОценок пока нет
- Swine Flu: Submittedby: Kristine Mae Sulla Danilo Lisondra Pn2-1 Submitted To: MR - Michael John EncinaДокумент29 страницSwine Flu: Submittedby: Kristine Mae Sulla Danilo Lisondra Pn2-1 Submitted To: MR - Michael John EncinaDaniell LisondraОценок пока нет
- Characteristics/Description of The Disease: "Influenza"Документ5 страницCharacteristics/Description of The Disease: "Influenza"Nathaniel PulidoОценок пока нет
- Swien InfluenzaДокумент2 страницыSwien InfluenzaASHFAQ REHMANIОценок пока нет
- Note On Swine FluДокумент9 страницNote On Swine Flumrigendrarai1987Оценок пока нет
- A H1N1 (Swine Flu) 2009 PandemicДокумент8 страницA H1N1 (Swine Flu) 2009 PandemicVehn Marie Dela RosaОценок пока нет
- Swine FluДокумент5 страницSwine FluHpu JogindernagerОценок пока нет
- Mumps and Influenza ComparedДокумент11 страницMumps and Influenza ComparedPutri CaesarriniОценок пока нет
- Swine Influenza: Nature of The DiseaseДокумент8 страницSwine Influenza: Nature of The Diseasejawairia_mmgОценок пока нет
- TBL 15 V4 - Viral PneumoniaДокумент24 страницыTBL 15 V4 - Viral PneumoniaFaysal RafiОценок пока нет
- Swine Influenza (Also Called Swine Flu, Hog Flu, Pig Flu and Sometimes, The Swine) Is An InfectionДокумент9 страницSwine Influenza (Also Called Swine Flu, Hog Flu, Pig Flu and Sometimes, The Swine) Is An InfectionAjith J NairОценок пока нет
- Nfluenza H N: Prepared by Ms. Carmelle Grace Cabaron BSN IiiaДокумент33 страницыNfluenza H N: Prepared by Ms. Carmelle Grace Cabaron BSN IiiaLoverMind CabaronОценок пока нет
- 584 1130 1 PBДокумент3 страницы584 1130 1 PBAlden Lui SevillaОценок пока нет
- Are IsДокумент2 страницыAre IshannahbucsОценок пока нет
- Scan 16 May 2021 at 8.20 PMДокумент8 страницScan 16 May 2021 at 8.20 PMGringgo PanesОценок пока нет
- InfluenzaVirusInfectionsHumans Jul13Документ2 страницыInfluenzaVirusInfectionsHumans Jul13dw_duchОценок пока нет
- The Pathology of Influenza Virus InfectionsДокумент33 страницыThe Pathology of Influenza Virus InfectionsAgronaSlaughterОценок пока нет
- Communicable DiseasesДокумент22 страницыCommunicable DiseaseskaramnОценок пока нет
- Bird FluДокумент5 страницBird FluNader SmadiОценок пока нет
- Bird FluДокумент3 страницыBird FluMd KhanОценок пока нет
- CDs L2 4th 2021 2022Документ46 страницCDs L2 4th 2021 2022محمد رافد لطيفОценок пока нет
- Influenza A H1N1 (English Version)Документ57 страницInfluenza A H1N1 (English Version)Dr.Sathaporn Kunnathum100% (4)
- Symposium Transcript 11 2004Документ49 страницSymposium Transcript 11 2004Mark ReinhardtОценок пока нет
- Avian Influenza H5N1 Bird Flu: DR Sanjay Shrestha IM Resident, NAMSДокумент54 страницыAvian Influenza H5N1 Bird Flu: DR Sanjay Shrestha IM Resident, NAMSSanjay ShresthaОценок пока нет
- Swine Flu Research Paper PDFДокумент6 страницSwine Flu Research Paper PDFeghkq0wf100% (1)
- Novel H1N1 Flu (Swine Flu) and You: On This PageДокумент8 страницNovel H1N1 Flu (Swine Flu) and You: On This PagethadikkaranОценок пока нет
- NSTP 1 Public Health AwarenessДокумент19 страницNSTP 1 Public Health AwarenessChristian Jed M. Bito-onОценок пока нет
- Red Cross: Be ReadyДокумент1 страницаRed Cross: Be ReadykoodhorahОценок пока нет
- World Health Organization - Swine Flu FAQ (April 26, 2009)Документ3 страницыWorld Health Organization - Swine Flu FAQ (April 26, 2009)antcomtech100% (9)
- Sample of Essay - The FluДокумент2 страницыSample of Essay - The FluMerisa WahyuningtiyasОценок пока нет
- Influenza A (h1n1) VirusДокумент5 страницInfluenza A (h1n1) VirusJanine SantosОценок пока нет
- Who Influenza 21082009Документ2 страницыWho Influenza 21082009SikainfluenssaОценок пока нет
- If You Think You Have Swine Flu: Swine Flu - Treatment and Prevention Swine Flu Vaccination ProgrammeДокумент8 страницIf You Think You Have Swine Flu: Swine Flu - Treatment and Prevention Swine Flu Vaccination Programmepoojapriya204Оценок пока нет
- Summary 1: Bird Flu: Avian InfluenzaДокумент15 страницSummary 1: Bird Flu: Avian InfluenzaedrichaОценок пока нет
- Avian Influenza (Bird Flu)Документ4 страницыAvian Influenza (Bird Flu)Gia Mae MagdaleraОценок пока нет
- NutrisiДокумент5 страницNutrisiWahyuni RusengОценок пока нет
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateДокумент1 страницаHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaОценок пока нет
- Técnica Inhalatoria en Lactantes Hospitalizados PDFДокумент5 страницTécnica Inhalatoria en Lactantes Hospitalizados PDFMario Chavez AvilaОценок пока нет
- Universidad Abierta para Adultos Uapa: Carrera de Psicologia IndustrialДокумент5 страницUniversidad Abierta para Adultos Uapa: Carrera de Psicologia Industrialluis miguel brito de la cruzОценок пока нет
- Mei Neni - PCVДокумент34 страницыMei Neni - PCVbenny christantoОценок пока нет
- FNCPДокумент7 страницFNCPMaria Ivy Rochelle TanОценок пока нет
- A24 - Mathura Lab Home Collection 1st Floor, Tera Tower, Bhuteshwar Road, MathuraДокумент2 страницыA24 - Mathura Lab Home Collection 1st Floor, Tera Tower, Bhuteshwar Road, MathuraAkki MauryaОценок пока нет
- Choking Relief For Adults, Children and Infants Signs of ChokingДокумент3 страницыChoking Relief For Adults, Children and Infants Signs of ChokingJeah Bearl AbellarОценок пока нет
- Chest ExaminationДокумент14 страницChest Examinationsajad abasewОценок пока нет
- Nursing Care Plan For InflammationДокумент2 страницыNursing Care Plan For InflammationJobelle AcenaОценок пока нет
- Respiratory Exam Skill SheetДокумент1 страницаRespiratory Exam Skill SheetMuhammed ElgasimОценок пока нет
- Upper Respiratory InfectionДокумент7 страницUpper Respiratory Infectionhazem barhoomОценок пока нет
- Cystic FibrosisДокумент4 страницыCystic Fibrosisakram alrdayОценок пока нет
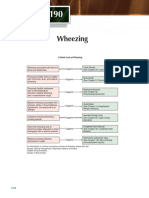
- Wheezing: A Quick Look at WheezingДокумент1 страницаWheezing: A Quick Look at WheezingpelinОценок пока нет
- Clinical, Spirometric and Therapeutic Profil of Frequent Exacerbators in COPDДокумент1 страницаClinical, Spirometric and Therapeutic Profil of Frequent Exacerbators in COPDEddy FriguiОценок пока нет
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Документ43 страницы(Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Haider Nadhem AL-rubaiОценок пока нет
- BronchitisДокумент11 страницBronchitisRenuka Sivaram100% (2)
- Chapter 23 Obstructive Lung Disease Chronic Obstructive Pulmonary DiseaseДокумент10 страницChapter 23 Obstructive Lung Disease Chronic Obstructive Pulmonary DiseaseZahra Margrette SchuckОценок пока нет
- OrthomyxovirusДокумент28 страницOrthomyxoviruskiedd_04Оценок пока нет
- Lower Respiratory Tract Infections in ChildrenДокумент18 страницLower Respiratory Tract Infections in ChildrenAmani HamoodОценок пока нет
- Acute BronchitisДокумент4 страницыAcute BronchitisLenjunОценок пока нет
- Diare September 180922Документ8 страницDiare September 180922anggaОценок пока нет
- 4 Ways To Treat A Cough - WikiHowДокумент16 страниц4 Ways To Treat A Cough - WikiHowamaze12Оценок пока нет
- SeqdumpДокумент7 страницSeqdumpAnayantzin AyalaОценок пока нет
- Explanation of The Problem Objective Nursing Intervention Rational EvaluationДокумент4 страницыExplanation of The Problem Objective Nursing Intervention Rational EvaluationmeteabОценок пока нет
- Cough: by Dr. Meghana Patil (Intern Batch 2016)Документ24 страницыCough: by Dr. Meghana Patil (Intern Batch 2016)Meghana PatilОценок пока нет
- Introduction Common ColdДокумент17 страницIntroduction Common ColdMueez BalochОценок пока нет
- Bronchoobstrustive SyndromeДокумент32 страницыBronchoobstrustive SyndromeCk Kma67% (3)
- Care of Patient With Respiratory DisordersДокумент35 страницCare of Patient With Respiratory Disorderskriiteeabns100% (1)
- Corona Virus Pre Departure Screening Questionnaire R2 PDFДокумент2 страницыCorona Virus Pre Departure Screening Questionnaire R2 PDFKaryaMaju Comp0% (1)
- Community-Acquired Pneumonia: Bello, Mickaela Bianca A. Gumiran, NomerДокумент37 страницCommunity-Acquired Pneumonia: Bello, Mickaela Bianca A. Gumiran, NomerKristine-Joy Legaspi FrancoОценок пока нет