Вам также может понравиться
- Not A Simple Plantar Wart: A Case of TungiasisДокумент5 страницNot A Simple Plantar Wart: A Case of TungiasisfikirudinОценок пока нет
- Bed Bug Outbreak in A Neonatal UnitДокумент6 страницBed Bug Outbreak in A Neonatal UnitfikirudinОценок пока нет
- Research Article in Vivo Antimalarial Activity of Annona Muricata Leaf Extract Plasmodium BergheiДокумент5 страницResearch Article in Vivo Antimalarial Activity of Annona Muricata Leaf Extract Plasmodium BergheifikirudinОценок пока нет
- Card1155266 PDFДокумент1 страницаCard1155266 PDFfikirudinОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- TracheostomyДокумент6 страницTracheostomynamithaОценок пока нет
- ASTM E466 Uji Fatik LogamДокумент5 страницASTM E466 Uji Fatik LogamMad Is100% (1)
- Types of Editorial Texts: Queen Zayra Dela Rosa Francisco DagohoyДокумент8 страницTypes of Editorial Texts: Queen Zayra Dela Rosa Francisco DagohoyAkiro KaitoОценок пока нет
- Bts Kat ArmyДокумент3 страницыBts Kat ArmyBeakatrine CabreraОценок пока нет
- Expansion and Contraction of Demand:: Change in Demand vs. Change in Quantity DemandedДокумент6 страницExpansion and Contraction of Demand:: Change in Demand vs. Change in Quantity DemandedbadarОценок пока нет
- History of English Culture and Literature MidДокумент4 страницыHistory of English Culture and Literature Midfirdasalsa59Оценок пока нет
- Test 04 AnswerДокумент16 страницTest 04 AnswerCửu KhoaОценок пока нет
- A Short History of The IsmailisДокумент30 страницA Short History of The IsmailisAbbas100% (1)
- The World of The GerДокумент302 страницыThe World of The GerMystic Master0% (1)
- Machine Learning and Iot For Prediction and Detection of StressДокумент5 страницMachine Learning and Iot For Prediction and Detection of StressAjj PatelОценок пока нет
- Paroles by PrevertДокумент29 страницParoles by PrevertCity Lights90% (10)
- Role of Communication in BusinessДокумент3 страницыRole of Communication in Businessmadhu motkur100% (2)
- 99 Attributes of Allah Al Khaliq (The Creator) Al Bari (The Inventor) Al Musawwir (The Fashioner)Документ7 страниц99 Attributes of Allah Al Khaliq (The Creator) Al Bari (The Inventor) Al Musawwir (The Fashioner)Abdourahamane GarbaОценок пока нет
- 8.31 - Standard CostingДокумент109 страниц8.31 - Standard CostingBhosx Kim100% (1)
- Elasticity of Supply and Demand SessionДокумент23 страницыElasticity of Supply and Demand SessionCharlizeK0% (1)
- Ijel - Mickey's Christmas Carol A Derivation That IДокумент6 страницIjel - Mickey's Christmas Carol A Derivation That ITJPRC PublicationsОценок пока нет
- Chapter 14 Chemical EquilibriumДокумент29 страницChapter 14 Chemical EquilibriumlynloeОценок пока нет
- 10 Tips For Better Legal WritingДокумент12 страниц10 Tips For Better Legal WritingYvzОценок пока нет
- Engineering Code of EthicsДокумент4 страницыEngineering Code of EthicsBeth Beth DiancoОценок пока нет
- Discoid Lupus Erythematosus - Background, Etiology, EpidemiologyДокумент8 страницDiscoid Lupus Erythematosus - Background, Etiology, EpidemiologyJair MathewsОценок пока нет
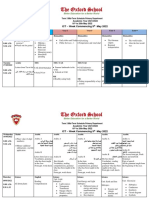
- Term 3 Mid-Term Assessment ScheduleДокумент9 страницTerm 3 Mid-Term Assessment ScheduleRabia MoeedОценок пока нет
- Tool - Single Double Triple Loop LearningДокумент2 страницыTool - Single Double Triple Loop LearningDwiAryantiОценок пока нет
- Conference Diplomacy: After Kenya's Independence in 1963, A Secession Movement Begun inДокумент3 страницыConference Diplomacy: After Kenya's Independence in 1963, A Secession Movement Begun inPeter KОценок пока нет
- Job AnalysisДокумент17 страницJob AnalysisMd. Mezba Uddin ShaonОценок пока нет
- Life in The Middle Ages Unit Study - Grade 8Документ21 страницаLife in The Middle Ages Unit Study - Grade 8HCSLearningCommonsОценок пока нет
- Chartered AccountancyДокумент28 страницChartered AccountancyNidhi ShrivastavaОценок пока нет
- Continuum Mechanics - Wikipedia PDFДокумент11 страницContinuum Mechanics - Wikipedia PDFjflksdfjlkaОценок пока нет
- Application of A One-Dimensional Large-Strain Consolidation Model To A Fullscale Tailings Storage Facility PDFДокумент11 страницApplication of A One-Dimensional Large-Strain Consolidation Model To A Fullscale Tailings Storage Facility PDFchenОценок пока нет
- Wardruna-Yggdrasil Bio EngДокумент3 страницыWardruna-Yggdrasil Bio EngCristian RamirezОценок пока нет
- RB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasДокумент2 страницыRB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasRifat TaopikОценок пока нет