Вам также может понравиться
- Clinical Cardiology - August 1990 - Malik - Heart Rate VariabilityДокумент7 страницClinical Cardiology - August 1990 - Malik - Heart Rate VariabilityP AlexiaОценок пока нет
- Monitoring Fluid ResponsivenessДокумент7 страницMonitoring Fluid Responsivenessvaleria SepviОценок пока нет
- 08 Chapter 2Документ10 страниц08 Chapter 2surbhi pareekОценок пока нет
- Biology NotesДокумент8 страницBiology NotesJenna PretalОценок пока нет
- Autorregulacion CerebralДокумент74 страницыAutorregulacion CerebralMarisol M CastilloОценок пока нет
- Bezold-Jarisch: The Reflex Revisited: Clinical Implications of Inhibitory Reflexes Originating in The HeartДокумент13 страницBezold-Jarisch: The Reflex Revisited: Clinical Implications of Inhibitory Reflexes Originating in The HeartDenny IntanОценок пока нет
- Raven Et Al-2006-Experimental PhysiologyДокумент13 страницRaven Et Al-2006-Experimental PhysiologyJesus Maturana YañezОценок пока нет
- Passive Leg Raising and Fluid Responsiveness Monnet CCM 2006Документ6 страницPassive Leg Raising and Fluid Responsiveness Monnet CCM 2006Leiniker Navarro ReyОценок пока нет
- Baker 2013Документ6 страницBaker 2013Moni-k GuarnerosОценок пока нет
- Documento PDFДокумент5 страницDocumento PDFJose Miguel CastellonОценок пока нет
- Heart Rate Variability in Anaesthesiology - Narrative ReviewДокумент8 страницHeart Rate Variability in Anaesthesiology - Narrative ReviewvienvienkkОценок пока нет
- Time and Frequency Domain Analysis of Heart Rate VariabilityДокумент7 страницTime and Frequency Domain Analysis of Heart Rate VariabilityArchana TatavartiОценок пока нет
- MilicevicДокумент6 страницMilicevicKlaudijus VitkauskasОценок пока нет
- HEARTRATEVARIABILITYДокумент8 страницHEARTRATEVARIABILITYdenta aeОценок пока нет
- VVS y VPP EN CIRUGÍA CARDÍACA BYPASS SIN CEC - 2005Документ7 страницVVS y VPP EN CIRUGÍA CARDÍACA BYPASS SIN CEC - 2005Elsa AivarОценок пока нет
- J Cobeha 2017 12 017Документ7 страницJ Cobeha 2017 12 017Soumitra KunduОценок пока нет
- Evaluation of Heart Rate Variability - UpToDateДокумент31 страницаEvaluation of Heart Rate Variability - UpToDateGonçalo MirandaОценок пока нет
- Hipotensi Ortostatik JurnalДокумент4 страницыHipotensi Ortostatik JurnalmuhammadОценок пока нет
- Ajpheart 1985 249 4 h867Документ9 страницAjpheart 1985 249 4 h867Rakibul HasanОценок пока нет
- Safat2018 Interaction Between HT and Arterial StiffnessДокумент10 страницSafat2018 Interaction Between HT and Arterial StiffnessMumtaz MaulanaОценок пока нет
- Park 2012Документ5 страницPark 2012Arankesh MОценок пока нет
- Hemodynamic Monitoring ModalitiesДокумент14 страницHemodynamic Monitoring Modalitiesrudy sanabriaОценок пока нет
- Functional Hemodynamic Monitoring PDFДокумент10 страницFunctional Hemodynamic Monitoring PDFPGI AnaesthesiaОценок пока нет
- Effects of Respiratory Interval On Vagal Modulation of Heart RateДокумент8 страницEffects of Respiratory Interval On Vagal Modulation of Heart RateGuillermo Castro ContardoОценок пока нет
- Aplicacao Da Analise de Onda de PAДокумент6 страницAplicacao Da Analise de Onda de PACrystal LabancaОценок пока нет
- Heart Rate Variability (HRV) BiofeedbackДокумент9 страницHeart Rate Variability (HRV) BiofeedbackLUCIENE CRISTALDO ALBUQUERQUEОценок пока нет
- Reflexes That Control Cardiovascular FunctionДокумент11 страницReflexes That Control Cardiovascular FunctionJoão Pedro Dantas AlkimimОценок пока нет
- Dutra de Souza 2023Документ11 страницDutra de Souza 2023Paulo Emilio Marchete RohorОценок пока нет
- Lehrer2000 Article ResonantFrequencyBiofeedbackTrДокумент15 страницLehrer2000 Article ResonantFrequencyBiofeedbackTrAderilson OliveiraОценок пока нет
- CES Estimulacion en Nervio Vago-16Документ9 страницCES Estimulacion en Nervio Vago-16gonzalez1Оценок пока нет
- Jurnal Donor Darah 1Документ13 страницJurnal Donor Darah 1Ismi Prasastawati KurniawanОценок пока нет
- Effects of Hypertonic Saline On Myocardial Contractility in AnaesthetizedДокумент7 страницEffects of Hypertonic Saline On Myocardial Contractility in AnaesthetizedliyaОценок пока нет
- Acharya Et Al. - 2006 - Heart Rate Variability A ReviewДокумент22 страницыAcharya Et Al. - 2006 - Heart Rate Variability A Reviewicaro 2024Оценок пока нет
- Net Notes CardioДокумент9 страницNet Notes CardioJess PeltraОценок пока нет
- Pulse Rate Variability Is Not A Surrogate For Heart Rate VariabilityДокумент7 страницPulse Rate Variability Is Not A Surrogate For Heart Rate VariabilityFiras ZakОценок пока нет
- Heart Rate Variability DissertationДокумент8 страницHeart Rate Variability DissertationWriteMyPaperFastSingapore100% (1)
- Heart Rate Variability: A Diagnostic and Prognostic Tool in Anesthesia and Intensive CareДокумент15 страницHeart Rate Variability: A Diagnostic and Prognostic Tool in Anesthesia and Intensive CarenrlaprilianiОценок пока нет
- Nursing in Critical Care - 2011 - Parry - Inotropic Drugs and Their Uses in Critical CareДокумент9 страницNursing in Critical Care - 2011 - Parry - Inotropic Drugs and Their Uses in Critical Careأركان هيلث Arkan healthОценок пока нет
- Comparing LVEDP Vs PCWP JAMA Cardio.2018Документ2 страницыComparing LVEDP Vs PCWP JAMA Cardio.2018Sajjad HussainОценок пока нет
- Bedside Preload Assessment CVP, PLR and USG Guided JCCA Bali 2016Документ36 страницBedside Preload Assessment CVP, PLR and USG Guided JCCA Bali 2016Ari YudhaОценок пока нет
- 145 FullДокумент7 страниц145 FullIndrati TstrОценок пока нет
- Heart Rate Variability Measurement and Emerging UsДокумент11 страницHeart Rate Variability Measurement and Emerging UsDario GerpeОценок пока нет
- Paranjapeetal 2019PLRMpigsДокумент10 страницParanjapeetal 2019PLRMpigsCristina RamirezОценок пока нет
- Reflexes That Control Cardiovascular FunctionДокумент11 страницReflexes That Control Cardiovascular FunctionRaam NaikОценок пока нет
- Recanalization, Reperfusion, and Recirculation in StrokeДокумент6 страницRecanalization, Reperfusion, and Recirculation in StrokeJosver PretellОценок пока нет
- Nishimura 1986 Val SalvaДокумент7 страницNishimura 1986 Val SalvaAlfred MCgregorОценок пока нет
- 1 s2.0 S2452302X21003648 MainДокумент29 страниц1 s2.0 S2452302X21003648 MainMahdi HosseiniОценок пока нет
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersДокумент8 страницJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonОценок пока нет
- Heart Rate Variability in An Ageing PopulationДокумент9 страницHeart Rate Variability in An Ageing PopulationBasharat BhatОценок пока нет
- Vijayaraman 2017Документ16 страницVijayaraman 2017Mickola VorokhtaОценок пока нет
- Vascular Pedicle Width On Chest Radiograph As A MeДокумент8 страницVascular Pedicle Width On Chest Radiograph As A MeSoftwarebolivia EnriqueОценок пока нет
- Breath Holding Index in The Evaluation of Cerebral VasoreactivityДокумент5 страницBreath Holding Index in The Evaluation of Cerebral Vasoreactivityydhapratama11Оценок пока нет
- Guidelines: Heart Rate VariabilityДокумент28 страницGuidelines: Heart Rate VariabilityAlejandro Peñaloza TapiaОценок пока нет
- A Review of Heart Rate Variability and Its ApplicationsДокумент6 страницA Review of Heart Rate Variability and Its ApplicationsBalkan RomeroОценок пока нет
- Furlan 2000Документ8 страницFurlan 2000Ivana MilakovicОценок пока нет
- Electrocardiographic Artifact MisleadiДокумент5 страницElectrocardiographic Artifact MisleadiMSОценок пока нет
- Establishing The Mechanism of Supraventricular Tachycardia in The Electrophysiology LaboratoryДокумент15 страницEstablishing The Mechanism of Supraventricular Tachycardia in The Electrophysiology LaboratorySamuelОценок пока нет
- Electrocardiographic Criteria For The Diagnosis of Left Ventricular HypertrophyДокумент10 страницElectrocardiographic Criteria For The Diagnosis of Left Ventricular HypertrophyHendri SaputraОценок пока нет
- Assessment of Autonomic Functions in Individuals With Cerebral PalsyДокумент6 страницAssessment of Autonomic Functions in Individuals With Cerebral PalsydevdsantoshОценок пока нет
- Announcement List Displayed Poster 32nd ASMIHAДокумент36 страницAnnouncement List Displayed Poster 32nd ASMIHADewi AmeliaОценок пока нет
- Case Study Post Operative - SumbadДокумент3 страницыCase Study Post Operative - SumbadMb SumbadОценок пока нет
- BP ChartДокумент5 страницBP Chartsunil_bhim100% (1)
- Thermoregulation-Pure PPT BasedДокумент12 страницThermoregulation-Pure PPT BasedMonesa Christy VillanuevaОценок пока нет
- Journal of Ayurveda and Integrative Medicine: Apar Avinash Saoji, B.R. Raghavendra, N.K. ManjunathДокумент9 страницJournal of Ayurveda and Integrative Medicine: Apar Avinash Saoji, B.R. Raghavendra, N.K. ManjunathALiint Nissa NisaniestОценок пока нет
- What Is Cardiovascular FitnessДокумент10 страницWhat Is Cardiovascular FitnessAbigail AnziaОценок пока нет
- AP Bio - Chapter 40 OutlineДокумент8 страницAP Bio - Chapter 40 OutlineEllen LiОценок пока нет
- SSI Freediving Level 1Документ2 страницыSSI Freediving Level 1StephanieОценок пока нет
- Reflection On Taking Blood PressureДокумент3 страницыReflection On Taking Blood PressureFarisa MunirahОценок пока нет
- EAR First AidДокумент4 страницыEAR First Aidr_lakshmi2722Оценок пока нет
- GFZ 038Документ3 страницыGFZ 038adri20121989Оценок пока нет
- Meditec M700 Series: Multi-Parameter Patient MonitorsДокумент8 страницMeditec M700 Series: Multi-Parameter Patient MonitorsXavier Med Pvt. LtdОценок пока нет
- Lesson Plan Simple FormДокумент2 страницыLesson Plan Simple FormShaNe BesaresОценок пока нет
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementДокумент31 страницаPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionОценок пока нет
- A Morphological and Anatomical Observation in Plant LeavesДокумент11 страницA Morphological and Anatomical Observation in Plant LeavesAli SulaimanОценок пока нет
- SB8.2p ThermoregulationДокумент13 страницSB8.2p ThermoregulationHisokagenОценок пока нет
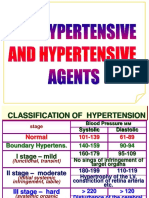
- Antihypertensive DrugsДокумент29 страницAntihypertensive Drugsmailforrandomuse100% (1)
- Photosynthesis 9700 CieДокумент8 страницPhotosynthesis 9700 CietrinhcloverОценок пока нет
- Understanding Recovery: A Wound Healing Model: by Dave StaplinДокумент3 страницыUnderstanding Recovery: A Wound Healing Model: by Dave StaplinluckydexxxОценок пока нет
- Physiological Changes During PregnancyДокумент44 страницыPhysiological Changes During PregnancyAnisa AbdullahiОценок пока нет
- Ventricular and Atrial Fibrillation and FlutterДокумент21 страницаVentricular and Atrial Fibrillation and Flutteryasir ishaqОценок пока нет
- Acute PainДокумент1 страницаAcute PainJohn Herrera TanchuanОценок пока нет
- Unit 1 Part 3 SignallingДокумент32 страницыUnit 1 Part 3 SignallingAnn NguyenОценок пока нет
- Nervous System WSHДокумент2 страницыNervous System WSHArdra AnilОценок пока нет
- Adrenaline PDFДокумент1 страницаAdrenaline PDFPilaRocio YHОценок пока нет
- PhysioEx Nuzla Emira Potensial AksiДокумент7 страницPhysioEx Nuzla Emira Potensial AksiPine's FauОценок пока нет
- An Detailed Lesson Plan For Circulatory and Respiratory SystemДокумент9 страницAn Detailed Lesson Plan For Circulatory and Respiratory SystemclarisseОценок пока нет
- Acupuncture Heart FailureДокумент11 страницAcupuncture Heart Failureabraham rumayaraОценок пока нет
- Gladys Cheing RS3030 CNN Introduction To Neuroscience Note 2021Документ73 страницыGladys Cheing RS3030 CNN Introduction To Neuroscience Note 2021Tsang AmyОценок пока нет
- 4 PharmacodynamicsДокумент21 страница4 Pharmacodynamicsaimi BatrisyiaОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!От EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Рейтинг: 5 из 5 звезд5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)От EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Рейтинг: 4 из 5 звезд4/5 (378)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (58)