Вам также может понравиться
- Lynch Syndrome: Molecular Mechanism and Current Clinical PracticeОт EverandLynch Syndrome: Molecular Mechanism and Current Clinical PracticeNaohiro TomitaОценок пока нет
- Rosen 2011Документ6 страницRosen 2011Evelynππ θσυОценок пока нет
- Cervical Cancer Trends in The United States: A 35-Year Population-Based AnalysisДокумент7 страницCervical Cancer Trends in The United States: A 35-Year Population-Based Analysisbehanges71Оценок пока нет
- Cancer ColorectalДокумент13 страницCancer ColorectalSihuar Fernando Abarca Lozano100% (1)
- Manejo de Neoplasia Intraepitelial AnalДокумент10 страницManejo de Neoplasia Intraepitelial AnalLibertad DíazОценок пока нет
- Thyroid Ca MortalityДокумент9 страницThyroid Ca MortalityMade RusmanaОценок пока нет
- Human Papillomavirus-Associated Cancers in Patients With Human Immunodeficiency Virus Infection and Acquired Immunodeficiency SyndromeДокумент11 страницHuman Papillomavirus-Associated Cancers in Patients With Human Immunodeficiency Virus Infection and Acquired Immunodeficiency SyndromeKerin ArdyОценок пока нет
- 612.full Bisa JadiДокумент8 страниц612.full Bisa JadiSunjaya TunggalaОценок пока нет
- Clinical Practice GuidelinesДокумент9 страницClinical Practice GuidelinesAhmad13 RizzqiОценок пока нет
- Ahmed 2014Документ12 страницAhmed 2014indahОценок пока нет
- MEHU130 U2 T74 Colorectal CancerДокумент14 страницMEHU130 U2 T74 Colorectal CancerStefani AtlleОценок пока нет
- (International Journal of Cancer Vol. 77 Iss. 5) Milena Sant - Riccardo Capocaccia - Arduino Verdecchia - Jacques Es - Survival of Women With BreastДокумент5 страниц(International Journal of Cancer Vol. 77 Iss. 5) Milena Sant - Riccardo Capocaccia - Arduino Verdecchia - Jacques Es - Survival of Women With BreastTulioОценок пока нет
- Pi Is 1470204519304565Документ13 страницPi Is 1470204519304565Agung Budi PamungkasОценок пока нет
- 2011 ArticleДокумент14 страниц2011 Articleyongky sugandaОценок пока нет
- Colorectal Cancer RiskДокумент17 страницColorectal Cancer RiskHerlina TanОценок пока нет
- J Amjoto 2019 102279Документ5 страницJ Amjoto 2019 102279Gisela LalitaОценок пока нет
- International Incidence and Mortality Trends of Liver Cancer: A Global ProfileДокумент9 страницInternational Incidence and Mortality Trends of Liver Cancer: A Global ProfileNovita ApramadhaОценок пока нет
- Colorectal Cancer Screening English 2007 PDFДокумент18 страницColorectal Cancer Screening English 2007 PDFtanjudinОценок пока нет
- Penile Cancer: January 2018Документ46 страницPenile Cancer: January 2018jogjagudegОценок пока нет
- Biology - Sample Research Paper-1Документ10 страницBiology - Sample Research Paper-1Prasanna SankheОценок пока нет
- The Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFДокумент7 страницThe Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFJorge JaraОценок пока нет
- Radiotherapy and OncologyДокумент6 страницRadiotherapy and OncologyIntan Kartika NursyahbaniОценок пока нет
- Ijbc2020 1963814Документ6 страницIjbc2020 1963814Kurnia AlkatiriОценок пока нет
- Colon Cancer Clinical Macroscopic and MiДокумент10 страницColon Cancer Clinical Macroscopic and MiElena CaterevОценок пока нет
- 10 1038@srep29765Документ9 страниц10 1038@srep29765jenny12Оценок пока нет
- 23 - Cancer Risk in Patients With Candidiasis - A NationwideДокумент12 страниц23 - Cancer Risk in Patients With Candidiasis - A NationwideRenan RodriguesОценок пока нет
- Salivary Gland YumorДокумент6 страницSalivary Gland YumorreioctabianoОценок пока нет
- Incidence Mortality Survival and Prognostic AnalysДокумент15 страницIncidence Mortality Survival and Prognostic AnalyslhykaОценок пока нет
- Articol1 1Документ12 страницArticol1 1Smaranda GavrilОценок пока нет
- Research: ArticleДокумент4 страницыResearch: ArticleMuthu KumarОценок пока нет
- Human Germ Cell Tumors Are Developmental Cancers: Impact of Epigenetics On Pathobiology and ClinicДокумент28 страницHuman Germ Cell Tumors Are Developmental Cancers: Impact of Epigenetics On Pathobiology and Clinicarcobaleno589Оценок пока нет
- Filipou - 2016Документ4 страницыFilipou - 2016TurboОценок пока нет
- 2-Jankovic (4-12)Документ9 страниц2-Jankovic (4-12)Okki Masitah Syahfitri NasutionОценок пока нет
- Leukemia in Iran: Epidemiology and Morphology Trends: Research ArticleДокумент6 страницLeukemia in Iran: Epidemiology and Morphology Trends: Research ArticleMuhammad Rifal MardaniОценок пока нет
- Cancers 13 02025 v2Документ23 страницыCancers 13 02025 v2Sha AbdulaОценок пока нет
- Mcglynn 2020Документ23 страницыMcglynn 2020Luluil MunirohОценок пока нет
- Obesity Surgery and Risk of CoДокумент7 страницObesity Surgery and Risk of CoNs. Dini Tryastuti, M.Kep.,Sp.Kep.,KomОценок пока нет
- Worldwide Burden of Colorectal Cancer: A ReviewДокумент5 страницWorldwide Burden of Colorectal Cancer: A ReviewRomário CerqueiraОценок пока нет
- The New England Journal of MedicineДокумент12 страницThe New England Journal of MedicineElyzabeth BonnesОценок пока нет
- Epidemiology of Vestibular Schwannoma in The United States 2004-2016Документ8 страницEpidemiology of Vestibular Schwannoma in The United States 2004-2016Indra PrimaОценок пока нет
- Cummings Et Al-2014-The Journal of PathologyДокумент9 страницCummings Et Al-2014-The Journal of Pathologyalicia1990Оценок пока нет
- DanielДокумент8 страницDanielLora MyrickОценок пока нет
- Carol E. 2015Документ12 страницCarol E. 2015Andrea QuillupanguiОценок пока нет
- Problem Statement WORLD Cancer Afflicts All Communities WorldwideДокумент30 страницProblem Statement WORLD Cancer Afflicts All Communities Worldwidesalma0430100% (2)
- Lacet ReportДокумент21 страницаLacet Reportm_manuela2002Оценок пока нет
- Esophageal Cancer Male To Female Incidence Ratios in Africa A - 2018 - Cancer EДокумент10 страницEsophageal Cancer Male To Female Incidence Ratios in Africa A - 2018 - Cancer EFlorin AchimОценок пока нет
- 07 Rosemurgy2019Документ5 страниц07 Rosemurgy2019Natalindah Jokiem Woecandra T. D.Оценок пока нет
- Research Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisДокумент10 страницResearch Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisAnonymous aH8gCZ7zjОценок пока нет
- The Prognosis of Breast Cancer in MalesДокумент8 страницThe Prognosis of Breast Cancer in Malesd17oОценок пока нет
- Clinical Oncology: S. Otter, S. Whitaker, J. Chatterjee, A. StewartДокумент10 страницClinical Oncology: S. Otter, S. Whitaker, J. Chatterjee, A. StewartKhrisna Whaty SilalahiОценок пока нет
- Cancers: Sex Difference and Smoking Effect of Lung Cancer Incidence in Asian PopulationДокумент12 страницCancers: Sex Difference and Smoking Effect of Lung Cancer Incidence in Asian PopulationMhd Fakhrur RoziОценок пока нет
- Profile and Survival of Tongue Cancer Patients in "Dharmais" Cancer Hospital, JakartaДокумент5 страницProfile and Survival of Tongue Cancer Patients in "Dharmais" Cancer Hospital, JakartaAlyani Akramah BasarОценок пока нет
- Lectura 1 PDFДокумент5 страницLectura 1 PDFCarmen Castillo RequenaОценок пока нет
- 2018 - Article - 6627 SurvivalДокумент10 страниц2018 - Article - 6627 SurvivalMario OrtizОценок пока нет
- Colorectal Cancer Facts and Figures 2014 2016 (1) 6Документ5 страницColorectal Cancer Facts and Figures 2014 2016 (1) 6joseОценок пока нет
- 2013 Predicting Lymph Node Metastases in Early Rectal CancerДокумент5 страниц2013 Predicting Lymph Node Metastases in Early Rectal CancerjohnnhekoОценок пока нет
- Cancers 10 00248Документ81 страницаCancers 10 00248Deepak ChinchapattanamОценок пока нет
- The Role of Immune Suppression and HHV-8 in TheДокумент5 страницThe Role of Immune Suppression and HHV-8 in TheAbsalom MwazhaОценок пока нет
- PIIS0923753419454938Документ10 страницPIIS0923753419454938indahОценок пока нет
- English Vocabulary: No. Nama FotoДокумент7 страницEnglish Vocabulary: No. Nama Fotofiora.ladesvitaОценок пока нет
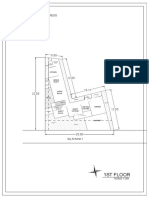
- 1St Floor: House On Paus Schematic Plan ProgressДокумент2 страницы1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaОценок пока нет
- English Vocabulary 2: No. Nama FotoДокумент8 страницEnglish Vocabulary 2: No. Nama Fotofiora.ladesvitaОценок пока нет
- Vocab Coco 2Документ7 страницVocab Coco 2fiora.ladesvitaОценок пока нет
- Des An Jose 2019Документ6 страницDes An Jose 2019fiora.ladesvitaОценок пока нет
- Smooth Sailing - Navigating The Sea of Law Applicable To The CruiДокумент35 страницSmooth Sailing - Navigating The Sea of Law Applicable To The Cruifiora.ladesvitaОценок пока нет
- Mahjoob2014 PDFДокумент5 страницMahjoob2014 PDFfiora.ladesvitaОценок пока нет
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyДокумент10 страницDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaОценок пока нет
- Eilers 2007Документ12 страницEilers 2007fiora.ladesvitaОценок пока нет
- Quat Trin 2006Документ10 страницQuat Trin 2006fiora.ladesvitaОценок пока нет
- F374W1M2L5G52563 FirstДокумент1 страницаF374W1M2L5G52563 Firstfiora.ladesvitaОценок пока нет
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaДокумент12 страницChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaОценок пока нет
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaДокумент12 страницChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaОценок пока нет
- Gibson 2010Документ19 страницGibson 2010fiora.ladesvitaОценок пока нет
- Quat Trin 2006Документ10 страницQuat Trin 2006fiora.ladesvitaОценок пока нет
- Abdul Kadir 2016Документ7 страницAbdul Kadir 2016fiora.ladesvitaОценок пока нет
- Lalla 2008Документ17 страницLalla 2008fiora.ladesvitaОценок пока нет
- Abdul Kadir 2016Документ7 страницAbdul Kadir 2016fiora.ladesvitaОценок пока нет
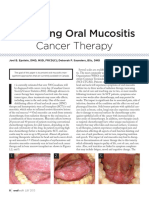
- Managing Oral Mucositis Oral Health July 2015Документ4 страницыManaging Oral Mucositis Oral Health July 2015fiora.ladesvitaОценок пока нет
- Full TextДокумент127 страницFull Textfiora.ladesvitaОценок пока нет
- Medicalscience: EcancerДокумент7 страницMedicalscience: Ecancerfiora.ladesvitaОценок пока нет
- ID Perbandingan Kualitas Hidup Pasien Gagal PDFДокумент9 страницID Perbandingan Kualitas Hidup Pasien Gagal PDFAlawiyahRasyaОценок пока нет
- Lalla 2008Документ17 страницLalla 2008fiora.ladesvitaОценок пока нет
- 2015 Conference 10Документ11 страниц2015 Conference 10fiora.ladesvitaОценок пока нет
- Assessment Rating ScaleДокумент8 страницAssessment Rating Scalefiora.ladesvitaОценок пока нет
- G15 v03 ED Design Guidelines Dec-14Документ77 страницG15 v03 ED Design Guidelines Dec-14gracegozaliОценок пока нет
- Ambulatory Care Nursing: Coming Soon!Документ16 страницAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaОценок пока нет
- Ni Hms 544150Документ15 страницNi Hms 544150fiora.ladesvitaОценок пока нет
- Anderson2004 PDFДокумент7 страницAnderson2004 PDFfiora.ladesvitaОценок пока нет
- Nursing Careplan Lung CancerДокумент16 страницNursing Careplan Lung Canceranamika sharma100% (2)
- A Single-Arm Study of Sublobar Resection For Ground-Glass Opacity Dominant Peripheral Lung CancerДокумент15 страницA Single-Arm Study of Sublobar Resection For Ground-Glass Opacity Dominant Peripheral Lung CancerYTM LoongОценок пока нет
- Problem Statement WORLD Cancer Afflicts All Communities WorldwideДокумент30 страницProblem Statement WORLD Cancer Afflicts All Communities Worldwidesalma0430100% (2)
- Cancer and Oncology Nursing NCLEX Practice Quiz-1Документ30 страницCancer and Oncology Nursing NCLEX Practice Quiz-1Susie Salmon100% (2)
- She Jan 2010Документ122 страницыShe Jan 2010shemagononlyОценок пока нет
- Assignment On Investigations-OncologyДокумент12 страницAssignment On Investigations-OncologyAxsa AlexОценок пока нет
- Chapter 5 - Recognizing Airspace Versus Interstitial Lung DiseaseДокумент19 страницChapter 5 - Recognizing Airspace Versus Interstitial Lung DiseaseRisky IndraОценок пока нет
- MBChB4 5PastPapersДокумент172 страницыMBChB4 5PastPapersHariharan NarendranОценок пока нет
- 331-Book Chapter-3614-2-10-20210406Документ20 страниц331-Book Chapter-3614-2-10-20210406Yolla GitamayaОценок пока нет
- Self Administered Exam 4Документ31 страницаSelf Administered Exam 4priyarajan007100% (4)
- Case Presentation: Group 2Документ30 страницCase Presentation: Group 2Wendy EscalanteОценок пока нет
- Project Isr - JascapДокумент42 страницыProject Isr - JascapPrakrutiShahОценок пока нет
- Sarcoma SpecialistДокумент5 страницSarcoma SpecialistaminudinrahmanОценок пока нет
- Cisplatin Monograph 1jul2016Документ11 страницCisplatin Monograph 1jul2016Kurnia AnharОценок пока нет
- Breast and Lung CancerДокумент141 страницаBreast and Lung CancerabdurehmanОценок пока нет
- Daftar PustakaДокумент6 страницDaftar PustakaVERTEBRAE COASSОценок пока нет
- IM Intern's Entrance ExamДокумент23 страницыIM Intern's Entrance ExamAlfonso Martin PlantillaОценок пока нет
- Clay Farris Naff Nicotine and TobaccoДокумент112 страницClay Farris Naff Nicotine and TobaccoYurie SaegusaОценок пока нет
- Uterine Cancer Pa Tho PhysiologyДокумент17 страницUterine Cancer Pa Tho PhysiologyJeneva L. Lauzon100% (2)
- Rtog 0813 Marina CousinsДокумент22 страницыRtog 0813 Marina Cousinsapi-426094285Оценок пока нет
- Treatment & Prognosis of Ewing Sarcoma (Charles)Документ5 страницTreatment & Prognosis of Ewing Sarcoma (Charles)Charles BayogОценок пока нет
- Rare Malignant Glomus Tumor of The Esophagus With PulmonaryДокумент6 страницRare Malignant Glomus Tumor of The Esophagus With PulmonaryRobrigo RexОценок пока нет
- Persuasive SpeechДокумент4 страницыPersuasive SpeechRyan RanaОценок пока нет
- Cancer QuizДокумент3 страницыCancer QuizOsama AtifОценок пока нет
- 2015 Xsmoke - Student.731-703 CardozaДокумент12 страниц2015 Xsmoke - Student.731-703 CardozaAdrian Catin100% (1)
- Lung Disease Prediction System Using Data Mining TechniquesДокумент6 страницLung Disease Prediction System Using Data Mining TechniquesKEZZIA MAE ABELLAОценок пока нет
- Hilar EnlargementДокумент19 страницHilar EnlargementGriggrogGingerОценок пока нет
- Lung Cancer Lecture Notes (Quick Summary)Документ4 страницыLung Cancer Lecture Notes (Quick Summary)Ibrahim FoondunОценок пока нет
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTДокумент8 страницCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianОценок пока нет
- German New Medicine® (GNM) The New Medical Paradigm: Scientific Chart GNM BookstoreДокумент13 страницGerman New Medicine® (GNM) The New Medical Paradigm: Scientific Chart GNM Bookstoremayanekita100% (10)