Вам также может понравиться
- PrimerДокумент56 страницPrimerAyesha Alonto MambuayОценок пока нет
- DM No. 05, S. 2018 Naga City Preparations For The 2018 Palarong BicolДокумент9 страницDM No. 05, S. 2018 Naga City Preparations For The 2018 Palarong BicolAt Day's WardОценок пока нет
- Water Statistics Report 2009-2018Документ2 страницыWater Statistics Report 2009-2018At Day's WardОценок пока нет
- Office Directory NWRBДокумент4 страницыOffice Directory NWRBAt Day's WardОценок пока нет
- Birth Certificates and Other Civil Documents PDFДокумент22 страницыBirth Certificates and Other Civil Documents PDFAt Day's WardОценок пока нет
- Nutrition in Early Childhood Care and DevelopmentДокумент36 страницNutrition in Early Childhood Care and DevelopmentJonathan Renier VerzosaОценок пока нет
- Official Directory RCI 2018-2019Документ1 129 страницOfficial Directory RCI 2018-2019At Day's Ward100% (1)
- Road Traffic SignsДокумент40 страницRoad Traffic SignsRonald McRonaldОценок пока нет
- PIYC 2018 Advocacy PartnersДокумент12 страницPIYC 2018 Advocacy PartnersAt Day's WardОценок пока нет
- CS HF Directory 2018 Print PDFДокумент80 страницCS HF Directory 2018 Print PDFAt Day's WardОценок пока нет
- Rotary Club of Pasay Metro SunriseДокумент3 страницыRotary Club of Pasay Metro SunriseAt Day's WardОценок пока нет
- 26321-Phi-Pcr PH Integrated Community Health Svcs PRJДокумент59 страниц26321-Phi-Pcr PH Integrated Community Health Svcs PRJAt Day's WardОценок пока нет
- MembersInAClub PasayMetroSunriseДокумент4 страницыMembersInAClub PasayMetroSunriseAt Day's WardОценок пока нет
- Three Ingredients That Unclog Arteries and Destroy Fats in The Blood PDFДокумент2 страницыThree Ingredients That Unclog Arteries and Destroy Fats in The Blood PDFAt Day's WardОценок пока нет
- Birth Certificates and Other Civil DocumentsДокумент5 страницBirth Certificates and Other Civil DocumentsAt Day's WardОценок пока нет
- HSPME Endorsement Letter For PHA (Bato)Документ1 страницаHSPME Endorsement Letter For PHA (Bato)At Day's WardОценок пока нет
- Individual Performance Commitment and Review Ipcr Blank FormДокумент1 страницаIndividual Performance Commitment and Review Ipcr Blank FormAt Day's Ward100% (4)
- Fourmula 1 Slides by HPUДокумент15 страницFourmula 1 Slides by HPUAt Day's Ward100% (1)
- Declaration of Alma AtaДокумент3 страницыDeclaration of Alma AtaJustin James AndersenОценок пока нет
- FSMM OverviewДокумент11 страницFSMM OverviewAt Day's WardОценок пока нет
- Ra - 7846 - An Act Requiring Compulsory ImmunizationДокумент1 страницаRa - 7846 - An Act Requiring Compulsory ImmunizationAt Day's WardОценок пока нет
- Book 1Документ61 страницаBook 1Elinor DashwoodОценок пока нет
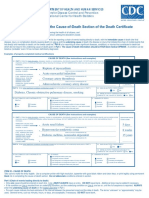
- Instructions For Completing The Cause of Death Section On Death Certificate PDFДокумент2 страницыInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoОценок пока нет
- Pantawidfaq PDFДокумент7 страницPantawidfaq PDFAbbey RoadОценок пока нет
- DOH AO 29 Rapid Reduction MN Mortality PDFДокумент13 страницDOH AO 29 Rapid Reduction MN Mortality PDFAt Day's WardОценок пока нет
- CITY ORDINANCE NO. 98-060 of Naga City, PhilippinesДокумент2 страницыCITY ORDINANCE NO. 98-060 of Naga City, PhilippinesAt Day's WardОценок пока нет
- Ordinance No. 06 Series of 2012-Anti-Rabies OrdinanceДокумент11 страницOrdinance No. 06 Series of 2012-Anti-Rabies OrdinanceAt Day's WardОценок пока нет
- Best Practices Bauang La UnionДокумент3 страницыBest Practices Bauang La UnionAt Day's WardОценок пока нет
- Ao15-95 - Reinstitution of The Previous Tetanus Toxoid Vaccination ScheduleДокумент1 страницаAo15-95 - Reinstitution of The Previous Tetanus Toxoid Vaccination ScheduleAt Day's WardОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)