Академический Документы
Профессиональный Документы
Культура Документы
Fiadjoe 2016
Загружено:
Dita DitotОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Fiadjoe 2016
Загружено:
Dita DitotАвторское право:
Доступные форматы
Articles
Airway management complications in children with difficult
tracheal intubation from the Pediatric Difficult Intubation
(PeDI) registry: a prospective cohort analysis
John Edem Fiadjoe, Akira Nishisaki, Narasimhan Jagannathan, Agnes I Hunyady, Robert S Greenberg, Paul I Reynolds, Maria E Matuszczak,
Mohamed A Rehman, David M Polaner, Peter Szmuk, Vinay M Nadkarni, Francis X McGowan Jr, Ronald S Litman, Pete G Kovatsis
Summary
Background Despite the established vulnerability of children during airway management, remarkably little is Lancet Respir Med 2015
known about complications in children with difficult tracheal intubation. To address this concern, we developed a Published Online
multicentre registry (Pediatric Difficult Intubation [PeDI]) to characterise risk factors for difficult tracheal December 16, 2015
http://dx.doi.org/10.1016/
intubation, establish the success rates of various tracheal intubation techniques, catalogue the complications of
S2213-2600(15)00508-1
children with difficult tracheal intubation, and establish the effect of more than two tracheal intubation attempts
See Online/Comment
on complications. http://dx.doi.org/10.1016/
S2213-2600(15)00519-6
Methods The PeDI registry consists of prospectively collected tracheal intubation data from 13 children’s hospitals in Children’s Hospital of
the USA. We established standard data collection methods before implementing the secure web-based registry. After Philadelphia, Philadelphia, PA,
establishing standard definitions, we collected and analysed patient, clinician, and practice data and tracheal USA (A Nishisaki MD,
J E Fiadjoe MD,
intubation outcomes. We categorised complications as severe or non-severe. Prof F X McGowan Jr MD,
Prof V M Nadkarni MD,
Findings Between August, 2012, and January, 2015, 1018 difficult paediatric tracheal intubation encounters were done. Prof R S Litman DO); Perelman
School of Medicine,
The most frequently attempted first tracheal intubation techniques were direct laryngoscopy (n=461, 46%), fibre-optic
University of Pennsylvania,
bronchoscopy (n=284 [28%]), and indirect video laryngoscopy (n=183 [18%]) with first attempt success rates of 16 (3%) Pennsylvania, PA, USA
of 461 with direct laryngoscopy, 153 (54%) of 284 with fibre-optic bronchoscopy, and 101 (55%) of 183 with indirect (J E Fiadjoe, Prof F X McGowan Jr,
video laryngoscopy. Tracheal intubation failed in 19 (2%) of cases. 204 (20%) children had at least one complication; Prof V M Nadkarni,
Prof M A Rehman MD,
30 (3%) of these were severe and 192 (19%) were non-severe. The most common severe complication was cardiac
Prof R S Litman); Children’s
arrest, which occurred in 15 (2%) patients. The occurrence of complications was associated with more than two Hospital Boston, Boston, MA,
tracheal intubation attempts, a weight of less than 10 kg, short thyromental distance, and three direct laryngoscopy USA (P G Kovatsis MD);
attempts before an indirect technique. Temporary hypoxaemia was the most frequent non-severe complication. Harvard Medical School,
Boston, MA, USA (P G Kovatsis);
Ann and Robert H Lurie
Interpretation More than two direct laryngoscopy attempts in children with difficult tracheal intubation are associated Children’s Hospital of Chicago,
with a high failure rate and an increased incidence of severe complications. These results suggest that limiting the Chicago, IL, USA
number of direct laryngoscopy attempts and quickly transitioning to an indirect technique when direct laryngoscopy (N Jagannathan MD); Feinberg
School of Medicine,
fails would enhance patient safety.
Northwestern University,
Illinois, IL, USA (N Jagannathan);
Funding None. The Children’s Hospital Denver,
Denver, CO, USA
(Prof D M Polaner MD);
Introduction Project (NAP4) of the UK Royal College of Anaesthetists University of Colorado School of
Tracheal intubation is a potentially life-saving procedure and the Difficult Airway Society did a study7,8 of major Medicine, Denver, CO, USA
done by many clinicians and is usually easily accomplished complications of airway management in their National (Prof D M Polaner); Seattle
with conventional direct laryngoscopy. Difficult tracheal Health Service hospitals during 1 year. They reported only Children’s Hospital, Seattle, WA,
USA (A I Hunyady MD);
intubation requires unique expertise and methods such ten events in children younger than 10 years, four of University of Washington
as extraglottic airway devices, fibre-optic bronchoscopy, which were related to difficult intubation. Complications Medical School, Seattle, WA,
and video laryngoscopy.1 Despite the widespread use of included subglottic narrowing, aspiration, and death. A USA (A I Hunyady); University of
these indirect techniques by various clinicians (eg, knowledge gap exists about the efficacy of various indirect Michigan Medical School,
Michigan, MI, USA
emergency room physicians, neonatologists, intensivists, tracheal intubation methods in children, related (P I Reynolds MD); University of
surgeons, and anaesthesiologists), little is known about complications, and their risk factors. We successfully Texas Southwestern Medical
related adverse events.2–4 Children under care of an designed and implemented a collaborative, multicentre Center, Dallas, TX, USA
anaesthetist have more airway-related adverse events web-based registry (the Pediatric Difficult Intubation (Prof P Szmuk MD); Dallas and
Children’s Medical Center at
than adults.5 Analysis of the American Society of (PeDI) registry) under the auspices of the Society for Dallas and Outcome Research
Anesthesiologists (ASA) closed claims database showed Pediatric Anesthesia to address these concerns and Consortium, Cleveland, OH,
that respiratory events were more common in children improve airway management in children with difficult USA (Prof P Szmuk); University
than in adults (43% vs 30% respectively; p≤ 0·01) with tracheal intubation. of Texas Health Science Center
Houston, Texas, TX, USA
greater mortality in paediatric claims than in adult claims The goals of the present study were to define the type and (M E Matuszczak MD);
(50% vs 35%; p ≤0·01).5,6 The Fourth National Audit incidence of complications that arise from airway
www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1 1
Articles
Children’s Memorial Herman
Hospital, Houston, TX, USA Research in context
(M E Matuszczak); and
The Johns Hopkins Medical Evidence before the study Added value of this study
Insitutions, Baltimore, MD, USA Findings of single centre studies in adults have shown that This study is the first to assess the complications of children
(R S Greenberg MD) repeated conventional tracheal intubation attempts in critically with difficult tracheal intubation as established by
Correspondence to: ill patients contribute to patient morbidity. Multicentre studies anaesthesiologists. This study establishes the complication
Dr John E Fiadjoe, Children’s
from paediatric intensive care units suggest that critically ill rates in these patients, identifies the risk factors for
Hospital of Philadelphia,
Department of Anesthesiology children are at high risk of complications during airway complications, and estimates the incidence of difficult tracheal
and Critical Care, Philadelphia, PA management in the intensive care unit. Little is known about intubation in children under anaesthesia care. This study has
19104, USA the complications and associated risk factors of airway identified a high complication rate. This finding should
FIADJOEJ@email.chop.edu
management in children with difficult tracheal intubation cared encourage further investigations and a change in clinical
for by anaesthesiologists. Before undertaking this study we practice patterns to enhance patient safety.
searched the scientific literature published between October,
Implications of all the available evidence
1975, and October, 2011, with the terms “pediatric difficult
Children with difficult tracheal intubation are a high-risk group
intubation”, “difficult airway”, “difficult direct laryngoscopy”,
and multiple tracheal intubation attempts are a key risk factor for
“difficult tracheal intubation”, “complications and pediatric
complications. Clinicians should treat every tracheal intubation
intubation”, “anesthesiology and pediatric difficult intubation”
attempt as a critical intervention and should limit the number of
in various combinations. We filtered our results to exclude adult
direct laryngoscopy and tracheal intubation attempts in this
studies, case reports, and case series. We found no relevant
population. Future research should investigate interventions to
large multicentre trials directly relating to this topic. The aim of
reduce these complications such as checklists and care protocols.
our study was to establish the complications and their
Additionally, the role and efficacy of passive oxygenation during
associated risk factors in children included in a prospective
tracheal intubation is unclear and should be investigated.
multicentre difficult tracheal intubation registry.
management in children with difficult tracheal intubation; standard operating procedures by expert consensus. This
establish the success of various tracheal intubation consensus was reached iteratively by open discussions
techniques; identify associations between patient, clinician, until all ten core members reached agreement.
and practice characteristics, and the occurrence of
complications; and establish the effect of multiple tracheal Study population
intubation attempts (>2 attempts) on complications. We collected tracheal intubations supervised or
performed by anaesthesiologists in elective and non-
Methods elective tracheal intubation situations. These situations
Study design included tracheal intubations in various anaesthetic
The PeDI Collaborative Group was created as a special locations and non-elective tracheal intubations from
interest group within the Society for Pediatric Anesthesia other hospital locations such as the emergency
with the goal to make possible multicentre collaboration department and intensive care unit whenever the
and quality improvement in patients with difficult anaesthesiology team assisted with airway management.
tracheal intubation. In December, 2010, members of the We used the following inclusion criteria in children
Society for Pediatric Anesthesia were solicited via younger than 18 years in whom an anaesthesiologist
electronic mail to take part in the special interest group; supervised or performed tracheal intubation: children
known experts in the paediatric anaesthesia community with difficult laryngeal exposure with conventional direct
were also invited to participate. 48 members of the society laryngoscopy as assessed by the attending
responded and were included in the group; however, ten anaesthesiologist (Cormack and Lehane classification
active members were instrumental in formulating the ≥3);9 children in whom conventional direct laryngoscopy
definitions for the registry. The group held four consensus was physically impossible because of anatomical reasons
development meetings between Oct 14, 2011, and Oct 17, (eg, severely limited mouth opening or other craniofacial
2012, which were attended by all the core members in anomalies); children who had failed conventional direct
person or by telephone conference. In addition to laryngoscopy within the preceding 6 months; children
meetings held at the Society for Pediatric Anesthesia and in whom the attending anaesthesiologist deferred
ASA annual meetings, task force discussions were conventional direct laryngoscopy because of an
continued using a dedicated group listserv and telephone unfavourable (predictive of a difficult laryngoscopy)
conferences to define paediatric airway management airway physical examination (eg, neonatal Robin
related terminology and adopt standard definitions in sequence) or the clinical situation in which a non-
order to create a multicentre registry. The group defined attending clinician obtains an unfavourable view that is
relevant outcomes, developed a standard data collection unconfirmed with a subsequent conventional direct
sheet, standardised data definitions, and established laryngoscopy by the attending anaesthesiologist.
2 www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1
Articles
The airway physical examination was not standardised We defined an intubation attempt as the act of inserting
but was based on the assessment of the attending an airway device into the pharynx or naris with the
anaesthesiologists. Several cases met more than one intent to perform tracheal intubation. Many attempts to
inclusion criteria and all tracheal intubation attempts were pass the tracheal tube through the vocal cords were
collected if one of the inclusion criteria was met. Separately regarded as one attempt provided the intubating device
we also queried each anaesthesiologist attending about
whether he or she anticipated the difficulty with mask
Cases entered Complication
ventilation or tracheal intubation or both.
Centre A 395 92 (23%)
Site enrolment and data capture Centre B 231 33 (14%)
After Institutional Review Board approval, we developed Centre C 117 23 (20%)
and piloted a secure, password-protected web-based data Centre D 76 22 (29%)
entry portal at the data coordinating centre (at the Centre E 37 9 (24%)
Children’s Hospital of Philadelphia, PA, USA). We Centre F 33 7 (21%)
expanded this portal to 13 academic children’s hospitals Centre G 31 4 (13%)
in the USA. The contributing sites are listed in the Centre H 26 4 (15%)
acknowledgments section. Each site identified a project Centre I 24 2 (8%)
coordinator (paediatric anaesthesiologist attending). The Centre J 24 3 (13%)
project coordinator educated their faculty about the Centre K 14 2 (14%)
registry, developed a site-specific compliance plan to Centre L 10 3 (30%)
ensure 100% data capture and did monthly audits for Total 1018 204 (20%)
data capture and accuracy. Our compliance plan included Median (IQR) 33 (24–97) 18% (14–24)
monthly data audits at each site and a standardised
Data are n or n (%) unless stated otherwise. Centres sorted by the number of
electronic medical record or manual search for missed difficult cases of tracheal intubation.
cases. The data coordinating centre did monthly audits
of the aggregate data to ensure data entry completeness Table 1: Case distribution across centres
and sent monthly missing data reports to the project
coordinators at each site. A steering committee reviewed
and approved each centre’s compliance plan before their Anticipated Unanticipated Total (n=1018)
full participation. One site failed to meet compliance difficult airway difficult airway
with audits and 100% data capture and was excluded (n=821) (n=197)
from the analysis. The web-based data entry portal used Success* 810 (99%) 188 (95%) 998 (98%)
the Research Electronic Data Capture (REDCap) method Surgical or failed airway* 10 (1%) 9 (5%) 19 (2%)
hosted at the data coordinating centre.10 Any complications 157 (19%) 47 (24%) 204 (20%)
We prospectively created a standard data collection sheet Severe complications† 19 (2%) 11 (6%) 30 (3%)
that was completed either by a member of the anaesthesia Cardiac arrest 10 (1%) 5 (3%) 15 (1%)
care team, the site principal investigator, or one of the Severe airway trauma 8 (1%) 6 (3%) 14 (1%)
principal investigator’s designees whenever a difficult Death 3 (<1%) 2 (1%) 5 (<1%)
intubation was encountered. We had three methods of Aspiration 1 (<1%) 0 1 (<1%)
data collection and entry: an electronic medical record hot Pneumothorax 1 (<1%) 0 1 (<1%)
key alerted a research assistant by pager whenever a Non-severe complications† 148 (18%) 44 (22%) 192 (19%)
difficult intubation was encountered and the data was Hypoxaemia 65 (8%) 29 (15%) 94 (9%)
attempted to be collected shortly after the intubation; the Minor airway trauma 36 (4%) 8 (4%) 44 (4%)
attending physician completed the data entry sheet Oesophageal intubation with immediate 21 (3%) 11 (6%) 32 (3%)
immediately after encountering a difficult intubation; and recognition
the care team was interviewed and data entry sheet was Laryngospasm 24 (3%) 8 (4%) 32 (3%)
completed after a discovered case via an electronic medical Epistaxis 12 (1%) 2 (1%) 14 (1%)
record search or quality assurance process. In most cases Bronchospasm 7 (1%) 5 (3%) 12 (1%)
the data sheet was collected immediately after the difficult Pharyngeal bleeding 10 (1%) 2 (1%) 12 (1%)
intubation occurred. The site principal investigator or a Arrhythmia 3 (<1%) 1 (1%) 4 (<1%)
member of the research team was responsible for verifying Emesis 4 (<1%) 0 4 (<1%)
the data on the collection forms and entering the data into
Data are n (%). *Outcome is missing in one case in anticipated difficult airway group. †Note that each case can have
the online registry.
more than one complication. The complication rates were not significantly different between the anticipated and the
unanticipated groups; however, severe complications were more commonly observed in the unanticipated difficult
Definitions airway group (p=0·015, χ² test).
We deemed any patient who met our inclusion criteria
Table 2: Airway management outcomes and complications
(category 1–4) as having difficult tracheal intubation.
www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1 3
Articles
Anticipated difficult airway (n=821) Unanticipated difficult airway (n=197) Total (n=1018)
No complications Complications p value No Complications p value No Complications p value
(n=664) (n=157) complications (n=47) complications (n=204)
(n=150) (n=814)
General
Age (months) 79 (10–156) 34 (8–147) 0·08 25 (4–149) 7 (2–34) 0·009 68 (8–154) 23 (5–131) 0·003
Weight (kg) 20 (8–35) 12 (6–30) 0·007 12 (5–41) 7 (4–20) 0·009 18 (7–35) 11 (5–28) 0·0002
Weight <10 kg 200 (30%) 71 (45%) 0·0003 66 (44%) 28 (60%) 0·06 266 (33%) 99 (49%) <0·0001
Male 369 (56%) 96 (61%) 0·21 108 (72%) 32 (68%) 0·61 477 (59%) 128 (63%) 0·28
ASA status (mean, median, IQR)* 2·9 (3:3–3) 3·1 (3:3–3) 0·02 2·6 (3:2–3) 1·8 (3:2–3) 0·08 2·9 (3:3–3) 3 (3:3–3) 0·01
ASA-Emergency* 30 (5%) 14 (9%) 0·03 8 (6%) 2 (4%) 0·73 38 (5%) 16 (8%) 0·07
Location
Operating room 606 (91%) 144 (92%) 0·86† 128 (86%) 36 (77%) 0·16† 734 (90%) 180 (88%) 0·41†
Off-site location 33 (5%) 3 (2%) .. 14 (9%) 2 (4%) .. 47 (6%) 5 (3%) ..
Intensive care unit 14 (2%) 6 (4%) .. 2 (1%) 1 (2%) .. 16 (2%) 7 (3%) ..
Other 11 (2%) 4 (2%) .. 6 (4%) 8 (17%) .. 17 (2%) 12 (6%) ..
Syndrome
Syndrome diagnosis‡ 498 (75%) 119 (76%) 0·97‡ 62 (42%) 16 (34%) 0·80‡ 560 (69%) 135 (66%) 0·54‡
No syndrome diagnosis 143 (22%) 34 (22%) .. 83 (55%) 27 (57%) 226 (28%) 61 (30%)
Undefined§ 23 (3%) 4 (2%) 5 (3%) 4 (9%) 28 (3%) 8 (4%)
Specific syndrome
Pierre-Robin sequence 94 (14%) 22 (14%) 0·96 4 (3%) 2 (4%) 0·58 98 (12%) 24 (12%) 0·91
Goldenhar syndrome 74 (11%) 11 (7%) 0·13 2 (1%) 0 (0%) 0·43 76 (9%) 11 (5%) 0·07
Difficult airway exam¶
Normal 32 (5%) 11 (7%) 0·27 70 (47%) 17 (36%) 0·21 102 (13%) 28 (14%) 0·65
Abnormal 631 (95%) 146 (93%) .. 80 (53%) 30 (64%) .. 711 (87%) 176 (86%) ..
Specific exam finding
Micrognathia 290 (44%) 71 (45%) 0·73 21 (14%) 12 (26%) 0·07 311 (38%) 83 (41%) 0·52
Limited mouth opening 269 (41%) 58 (37%) 0·41 11 (7%) 7 (15%) 0·12 280 (34%) 65 (32%) 0·49
Cervical spine immobility 137 (21%) 30 (19%) 0·67 3 (2%) 1 (2%) 0·96 140 (17%) 31 (15%) 0·49
Short thyromental distance 77 (12%) 33 (21%) 0·002 9 (6%) 5 (11%) 0·28 86 (11%) 38 (19%) 0·002
Anticipated difficulty with:
Mask ventilation and 94 (14%) 30 (19%) NA NA NA NA 94 (12%) 30 (15%) ··
laryngoscopy
Laryngoscopy only 565 (85%) 126 (80%) NA NA NA NA 565 (69%) 126 (62%) ··
Mask ventilation only 5 (1%) 1 (1%) NA NA NA NA 5 (1%) 1 (0%) ··
Unanticipated 0 (0%) 0 (0%) NA NA NA NA 150 (18%) 47 (23%) 0·13||
Difficult direct laryngoscopy
(inclusion criteria)**
Cormack scale 3–4 215 (32%) 85 (54%) <0·001 143 (95%) 43 (91%) 0·32 358 (44%) 128 (63%) <0·0001
Direct laryngoscopy impossible 169 (25%) 37 (24%) 0·62 0 (0%) 1 (2%) 0·24 169 (21%) 38 (19%) 0·50
Direct laryngoscopy failure within 109 (16%) 25 (16%) 0·88 2 (1%) 0 (0%) 1·00 111 (14%) 25 (12%) 0·60
6 months
Direct laryngoscopy is possible 231 (35%) 29 (18%) <0·001 4 (3%) 2 (4%) 0·58 235 (29%) 31 (15%) <0·0001
but harmful
Data are n (%) or median (IQR), unless otherwise stated. ASA=American Society of Anesthesiology. NA=not applicable. *Datapoints were missing in 17 cases. †p value based on operating room vs outside of
operating room. ‡Syndrome diagnosis was marked as yes if any known syndrome was diagnosed or suspected at the time of airway management; p value based on no syndrome vs syndrome undefined or
confirmed. §Undefined was marked when a syndrome was suspected but not confirmed. ¶Difficult airway exam was performed by attending anaesthesiologists, data missing in one case. ||p value based on
anticipated vs unanticipated difficulty before the case. **Difficult direct laryngoscopy (inclusion criteria): each case may meet more than one criterion. Syndrome diagnosis: marked as yes if any known syndrome
is diagnosed or suspected at the time of airway management.
Table 3: Patient demographics and outcomes
(eg, direct laryngoscope or video laryngoscope) Children (NEAR4KIDS) operational definitions.11,12 The
remained in place. following were categorised as severe complications: severe
We categorised complications as severe and non-severe, airway trauma (glottic or subglottic injury), clinical evidence
modified from the National Emergency Airway Registry for of aspiration (chest radiograph or bronchoscopy evidence),
4 www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1
Articles
Anticipated difficult airway (n=821) Unanticipated difficult airway (n=197) Total (n=1018)
No Complications p value No complications Complications p value No Complications p value
complications (n=157) (n=150) (n=47) complications (n=204)
(n=664) (n=814)
First attempt provider*
Trainee 389 (59%) 99 (63%) 0·053 80 (54%) 29 (62%) 0·39 469 (58%) 128 (63%) 0·18
CRNA 116 (17%) 15 (10%) ·· 37 (25%) 7 (15%) ·· 153 (19%) 22 (11%) ··
Attending anaesthesiologist 139 (21%) 33 (21%) ·· 29 (19%) 9 (19%) ·· 168 (21%) 42 (21%) ··
Otolaryngologist 18 (3%) 8 (5%) ·· 1 (1%) 0 (0%) ·· 19 (2%) 8 (4%) ··
Other 2 (0%) 1 (1%) ·· 2 (1%) 2 (4%) ·· 4 (0%) 3 (1%) ··
Successful provider†
Trainee 312 (47%) 55 (37%) ·· 31 (22%) 3 (6%) ·· 343 (43%) 58 (30%) ··
CRNA 72 (11%) 7 (5%) ·· 6 (4%) 0 (0%) ·· 78 (10%) 7 (4%) ··
Attending anaesthesiologist 236 (36%) 71 (48%) 0·007 96 (68%) 38 (83%) 0·051 332 (41%) 109 (56%) 0·001
Otolaryngologist 39 (6%) 14 (9%) ·· 6 (4%) 4 (9%) ·· 45 (5%) 18 (9%) ··
Other 2 (0%) 2 (1%) ·· 3 (2%) 1 (2%) ·· 5 (1%) 3 (1%) ··
Attending only 107 (16%) 22 (14%) 0·52 29 (19%) 8 (17%) 0·72 136 (17%) 30 (15%) 0·49
Attending experience
Median (year, IQR) 8 (3–20) 7 (3–14) 0·23 8 (4–18) 9 (3–18) 0·77 8 (3–20) 8 (3–17) 0·37
Fellowship training (%)‡ 631 (97%) 151 (97%) 0·68 137 (94%) 44 (94%) 0·73 768 (96%) 195 (97%) 0·96
Data are n (%) unless otherwise stated. CRNA=certified registered nurse anaesthetist. *Data missing in two cases; p value was based on trainee vs non-trainee. †17 intubations were never successful; data were
missing in three cases; p value was based on attending anaesthesiologist vs other. ‡Attending fellowship training status is missing in 17 cases.
Table 4: Provider characteristics
cardiac arrest, emergent surgical airway, oesophageal
1200 Trainee
intubation with delayed recognition, pneumothorax, and CRNA
death. Non-severe complications included minor airway Otolaryngologist
Other anaesthesiologist
trauma (dental or lip), pharyngeal bleeding, arrhythmia 1000
Primary anaesthesiologist
without haemodynamic consequences, bronchospasm,
epistaxis, oesophageal intubation with immediate
800
recognition, hypoxaemia, laryngospasm, and emesis
Number of cases
without aspiration. We defined hypoxaemia as a 10%
decrease from the pre-intubation oxygen saturation for 600
more than 45 s.
We collected other patient, clinician, and practice data 400
related to airway management. These included patient
demographics, airway physical examination findings,
mask ventilation efficacy (assessed with the Han scale13), 200
anaesthesia induction method, airway interventions, and
outcome (intubation success or failure). Patients were 0
1st 2nd 3rd 4th 5th
a-priori categorised by weight (<10 kg vs ≥10 kg).14–18
Tracheal intubation attempt
Clinician data included the clinician type (attending,
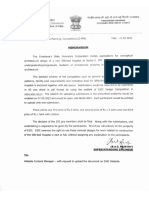
trainee, or registered nurse anaesthetist), the attending’s Figure 1: Proportion of airway providers for each attempt
fellowship training status and years of experience (time CRNA=certified registered nurse anaesthetist.
since completion of fellowship training). We also
documented the patients’ ASA physical status with interquartile ranges for non-parametric variables.
classification (1–6), a system to describe the patients’ We used histograms of the variable distributions to
medical condition before their anaesthetic.19 The addition determine normality. We used a contingency table
of E to the classification denotes an emergent procedure. method with χ² test for categorical variables with a
dichotomous outcome. For non-parametric variables, we
Statistical analysis used the Wilcoxon rank sum test. For multivariable
We did our statistical analysis with Stata (version 11.2). analysis, occurrence of any complications was a
Our sample included all available data during the study dichotomous dependent variable, multiple attempts
period. We report summary statistics using means and (≤2 attempts vs >2 attempts) was an independent variable,
standard deviation for parametric variables and medians and factors associated with multiple attempts in
www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1 5
Articles
Anticipated difficult airway (n=821) Unanticipated difficult airway (n=197) Total (n=1018)
No Complications p value No Complications p value No Complications p value
complications (n=157) complications (n=47) complications (n=204)
(n=664) (n=150) (n=814)
Induction technique 0·36 0·15 0·083
Mask induction 430 (65%) 99 (63%) ·· 93 (62%) 24 (51%) ·· 523 (64%) 123 (60%) ··
Intravenous induction 180 (27%) 43 (27%) ·· 53 (36%) 20 (43%) ·· 233 (29%) 63 (31%) ··
Intravenous sedation 36 (6%) 8 (5%) ·· 2 (1%) 0 (0%) ·· 38 (5%) 8 (4%) ··
Tracheal induction 9 (1%) 1 (1%) ·· 0 (0%) 0 (0%) ·· 9 (1%) 1 (0%) ··
NA 9 (1%) 6 (4%) ·· 2 (1%) 3 (6%) ·· 11 (1%) 9 (4%) ··
Anaesthesia approach 0·11 0·04 0·005
General 610 (92%) 145 (92%) ·· 145 (97%) 44 (94%) ·· 755 (93%) 189 (93%) ··
Sedation 47 (7%) 7 (4%) ·· 3 (2%) 0 (0%) ·· 50 (6%) 7 (3%) ··
Awake 6 (1%) 4 (3%) ·· 2 (1%) 0 (0%) ·· 8 (1%) 4 (2%) ··
None 1 (0%) 1 (1%) ·· 0 (0%) 3 (6%) ·· 1 (0%) 4 (2%) ··
Intubation route* 0·12 0·22 0·088
Oral 488 (74%) 109 (73%) ·· 128 (90%) 40 (87%) ·· 616 (77%) 149 (76%) ··
Nasal 166 (25%) 37 (25%) ·· 10 (7%) 5 (11%) ·· 176 (22%) 42 (21%) ··
Surgical 0 (0%) 1 (0%) ·· 0 (0%) 1 (2%) ·· 0 (0%) 2 (1%) ··
Other 5 (1%) 3 (2%) ·· 4 (3%) 0 (0%) ·· 9 (1%) 3 (2%) ··
First attempt device† 0·006 0·30 0·001
Direct laryngoscope 220 (33%) 69 (45%) ·· 128 (87%) 44 (94%) ·· 348 (43%) 113 (56%) ··
Flexible fibreoptic bronchoscope 226 (34%) 51 (33%) ·· 5 (3%) 2 (4%) ·· 231 (29%) 53 (26%) ··
Glidescope 158 (24%) 19 (12%) ·· 5 (3%) 1 (2%) ·· 163 (20%) 20 (10%) ··
Other or combined 57 (9%) 15 (10%) ·· 10 (7%) 0 (0%) ·· 67 (8%) 15 (7%) ··
Successful device‡ 0·06 0·49 0·037
Direct laryngoscope 41 (6%) 17 (12%) ·· 46 (34%) 17 (37%) ·· 87 (11%) 34 (18%) ··
Flexible fibreoptic bronchoscope 281 (43%) 69 (47%) ·· 22 (16%) 6 (13%) ·· 303 (39%) 75 (39%) ··
Glidescope 241 (37%) 42 (29%) ·· 48 (36%) 13 (28%) ·· 289 (37%) 55 (29%) ··
Other or combined 89 (14%) 18 (12%) ·· 18 (13%) 10 (22%) ·· 107 (14%) 28 (15%) ··
Neuromuscular blockade use 268 (40%) 63 (40%) 0·96 72 (48%) 30 (64%) 0·06 340 (42%) 93 (46%) 0·32
Data are n (%), unless otherwise stated. NA=not applicable. *Data are missing in 19 cases. †Data are missing in eight cases. ‡Intubation was not successful in 17 intubations.
Table 5: Association between practice characteristics and complications
univariate analysis as covariates. We deemed a p value of of 38 813, 35 000, and 8000, respectively. This finding
less than 0·05 as statistically significant. translates to 0·28%, 0·47%, and 0·25% of anaesthetics,
respectively suggesting a range of 2–5 difficult tracheal
Role of the funding source intubations in 1000 anaesthetised children. 80% (821/1018)
There was no funding source for this study. The of the difficult tracheal intubation cases were anticipated.
corresponding author had full access to all the data in the 20% (204/1018) of cases had at least one complication.
study and had final responsibility for the decision to Cardiac arrest (n=15; 2%) was the most common severe
submit for publication. complication, and hypoxaemia (n=94; 9%) was the most
common non-severe complication. All cardiac arrests
Results were preceded by hypoxaemia. Table 2 shows tracheal
The study period included data collected from our centres intubation-related outcomes. Four of the cardiac arrests
between Aug 6, 2012, and Jan 31, 2015. The 13 centres were non-elective urgent intubations; two cases in the
reported 1061 cases of tracheal intubation during this intensive care unit and two in the emergency room. 11 of
period. The four largest centres contributed most of the the cardiac arrest cases were elective non-urgent tracheal
cases in the registry; table 1 reports the distribution of intubations. Five patients died shortly after tracheal
cases across centres. One centre was excluded because of intubation (within 7 days), four were unrelated to tracheal
lack of full compliance with data capture rates and audits, intubation (cardiac arrest and withdrawal of care), and one
leaving 1018 cases for analysis (table 1). Three centres was related to difficult tracheal intubation (hypoxaemic
reported 112, 164, and 20 cases of difficult tracheal arrest). The complication rates were not significantly
intubation in 2014 with anaesthetic case volumes that year different between the anticipated and unanticipated
6 www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1
Articles
Anticipated difficult airway (n=821) Unanticipated difficult airway (n=197) Total (n=1018)
No Complications p value No Complications p value No complications Complications p value
complications (n=157) complications (n=47) (n=814) (n=204)
(n=664) (n=150)
Mask ventilation <0·0001 0·03 <0·0001
Easy mask ventilation 430 (65%) 66 (42%) ·· 118 (79%) 30 (64%) ·· 548 (67%) 96 (47%) ··
Airway adjunct needed 119 (18%) 39 (25%) ·· 24 (16%) 11 (23%) ·· 143 (18%) 50 (25%) ··
Difficult mask ventilation 39 (6%) 28 (18%) ·· 4 (3%) 6 (13%) ·· 43 (5%) 34 (17%) ··
Impossible for mask 0 (0%) 5 (3%) ·· 1 (<1%) 0 (0%) ·· 1 (<1%) 5 (2%) ··
ventilation
Not attempted 76 (11%) 19 (12%) 3 (2%) 0 (0%) 79 (10%) 19 (9%)
Extraglottic airway* <0·0001 0·45 <0·0001
Not attempted 553 (84%) 100 (64%) ·· 120 (80%) 37 (79%) ·· 673 (83%) 137 (67%) ··
Easy placement and 96 (14%) 34 (22%) ·· 23 (15%) 6 (13%) ·· 119 (15%) 40 (20%) ··
ventilation
Easy placement and poor 10 (2%) 11 (7%) ·· 5 (3%) 3 (6%) ·· 15 (2%) 14 (7%) ··
ventilation (tidal volume
<5 mL/kg)
Difficult placement and 2 (<1%) 4 (2%) ·· 1 (1%) 0 (0%) ·· 3 (<1%) 4 (2%) ··
easy ventilation
Difficult placement and 0 (0%) 6 (4%) ·· 0 (0%) 1 (2%) ·· 0 (0%) 7 (3%) ··
difficult ventilation
Impossible to place 1 (0%) 2 (1%) ·· 1 (1%) 0 (0%) ·· 2 (<1%) 2 (1%) ··
Number of attempts 2 (1–3) 3 (2–4) <0·0001 3 (3–5) 4 (3–6) 0·009 2 (1–3) 3 (2–5) <0·0001
(median, IQR)†
1 271 (41%) 23 (15%) ·· 10 (7%) 2 (4%) ·· 281 (34%) 25 (13%) ··
2 181 (27%) 33 (21%) ·· 20 (13%) 4 (9%) ·· 201 (25%) 37 (18%) ··
3 107 (16%) 36 (23%) ·· 46 (31%) 9 (19%) ·· 153 (19%) 45 (22%) ··
4 60 (9%) 26 (16%) ·· 32 (21%) 11 (23%) ·· 92 (11%) 37 (18%) ··
5 22 (4%) 11 (7%) ·· 23 (15%) 7 (15%) ·· 45 (6%) 18 (9%) ··
6 8 (1%) 8 (5%) ·· 7 (5%) 3 (6%) ·· 15 (2%) 11 (5%) ··
7 or more 15 (2%) 20 (13%) ·· 12 (8%) 11 (24%) ·· 27 (3%) 31 (15%) ··
Data are n (%), unless otherwise stated. *Extraglottic airway: data are missing in two cases. †p value calculated by Wilcoxon rank-sum test.
Table 6: Process characteristics
groups; however, severe complications were more (trainee and certified registered nurse anaesthetist).
common in the unanticipated group (χ² test p=0·015; Figure 1 shows the distribution of clinician types
table 2). attempting the first five tracheal intubations in patients
Patients who weighed less than 10 kg had more tracheal who had five or more attempts. Of note trainees made
intubations with complications (49% [99/204]) than 20% of fifth tracheal intubation attempts. The first
tracheal intubations without complications (33% attempt provider type was similar between anticipated
[266/814]; table 3). This was true in both the anticipated and unanticipated difficult airway cases. The attending
and unanticipated groups. Patients entered in the registry anaesthesiologist was the more successful provider in
because of a failed direct laryngoscopy by the attending unanticipated difficult airway cases than in anticipated
anaesthesiologist. Patients in category 1 (cases with difficult airway cases.
Cormack classification 3 and 4) had a greater proportion Inhalational induction of anaesthesia via facemask was
of complications (n=128; 63%; p<0·0001), and patients in the most common induction method used (64%
category 4 (suspected difficulty without attending direct [646/1018]; table 5). 77 (8%) of 1018 cases were difficult to
laryngoscopy confirmation) had fewer complications ventilate by facemask. Six patients were impossible to
(n=31 [15%]; p<0·0001; table 3). ventilate by facemask. This difficulty was anticipated in
The median number of years of experience of the five of these patients. Two patients received neuro-
supervising anaesthesiologist was 8 years (IQR 3–20; muscular blockade without improvement in the ability to
table 4). Although attending physicians made 21% of ventilate. Two patients were ventilated successfully using
first intubation attempts, they were the eventual an extraglottic airway device after facemask ventilation
successful clinician in 44% of cases, which meant they failed. Tracheal intubation was successful in all six patients
often took over the intubation from the other clinicians (table 6). The median number of tracheal intubation
www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1 7
Articles
(95% CI 1·4–1·6; p<0·0001). The median number of
0·6
attempts was 3 (IQR 2–5) for cases with complications
while the median was two attempts (IQR 1–3) for cases
Proportion of cases with complications
0·5
without complications (p<0·0001; table 6). Oxygen was
0·4 rarely given during tracheal intubation attempts. The
approaches reported included nasal cannula in 17 tracheal
0·3 intubations, modified nasopharyngeal airway in
76 tracheal intubations, and an endoscopy mask in four
0·2 tracheal intubations.
Tracheal intubation failed in 2% (19/1017) of cases
0·1
(table 2). The success rate of the first tracheal intubation
0 attempt in the registry cohort was only 30% (n=288);
1 2 3 4 5 6 ≥7 however, 98% of the patients were eventually successfully
Number of tracheal intubation attempts intubated. Figure 3 shows the distributions of devices
Figure 2: Proportion of cases with complications by the number of attempts used for each attempt. 46% (461/1010) of cases used
for airway management direct laryngoscopy for the first tracheal intubation
The average proportion of cases with complications by the number of required attempt, while it was the successful device in 12%
intubation attempts. Each error bar represents mean (SD). (121/978) of cases. Flexible fibre-optic laryngoscope was
the first attempt device in 28% (284/1010) of patients,
Other
whereas it was the successful device in 37% (378/978) of
1200
Glidescope cases. The most frequently attempted first tracheal
Flexible fibre-optic bronchoscope intubation techniques were direct laryngoscopy (direct
Direct laryngoscope
1000 laryngoscopy; n=461 [46%]), indirect video laryngoscopy
(n=183 [18%]), and fibre-optic bronchoscopy (n=284
800
[28%]) with success rates of 16 (3%) of 461, 101 (55%) of
183, and 153 (54%) of 284, respectively. An extraglottic
Number of cases
airway was attempted in 208 (20%) of 1016 cases.
600 Ventilation with the extraglottic airway was poor in 17%
(36/208) cases in which it was attempted, and extraglottic
400 airway placement was impossible in 2% (4/208) of
insertion attempts (table 6). Of the 36 failed extraglottic
airways 17% (14/84) received neuromuscular blockade
200
and 19% (22/118) received no neuromuscular blockade.
There were 455 cases with direct laryngoscopy as the
0
1st 2nd 3rd 4th 5th
initial approach that required three or more tracheal
Tracheal intubation attempt
intubation attempts. Of these cases, an early transition
(after the first or second direct laryngoscopy attempt) to a
Figure 3: Type of device for each attempt non-direct laryngoscopy technique was associated with
Other includes Airtraq, Karl Storz C-MAC, optical stylet, Anterior Commissure
fewer complications (62/297 [21%]) than cases with late
scope, and others.
transition (>2 direct laryngoscopy attempts; 48/158 [30%];
See Online for appendix p=0·024). The appendix shows associations between the
attempts was 2·5 (IQR 2–6) in these six patients. Three first attempted device and patient and provider
patients were intubated by otolaryngologists—one with a characteristics (appendix p 1).
rigid bronchoscope and two with standard direct After adjusting for clustering by site, patient factors,
laryngoscopy with a grade 4 view. Flexible fibre-optic weight less than 10 kg, thyromental distance, ASA
intubation was done successfully through an extraglottic physical status, inclusion criteria, and first attempt
airway in two patients and the GlideScope Cobalt was device, many attempts (>2) were independently
used in one patient. Two of these patients had cardiac associated with the occurrence of any complication
arrest during tracheal intubation attempts and were (OR 3·1, 95% CI 2·1–4·6; p<0·0001; table 7)
successfully resuscitated.
43% (433/1018) of patients in the registry were managed Discussion
with neuromuscular blockade. Cases where direct This prospective multicentre study estimated that
laryngoscopy was attempted for the first three attempts difficult tracheal intubation occurred in 2–5 per
(direct laryngoscopy persistence) had more complications 1000 paediatric anaesthesia cases in large academic
(48/158 [30%] vs 62/297 [21%]; p=0·02). The occurrence of centres in the USA. Furthermore, this registry showed
a complication was associated with the number of that 20% of children with difficult tracheal intubations
attempts (figure 2): odds ratio (OR) 1·5 per attempt had a complication. We identified the following
8 www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1
Articles
Univariate analysis Multivariate analysis
OR (95% CI) p value OR (95% CI) p value
Multiple attempt (>2 attempts) 3·48 (2·48–4·89) <0·0001 3·08 (2·08–4·57) <0·0001
Weight <10 kg 2·09 (1·51–2·88) <0·0001 1·61 (1·13–2·31) 0·009
Physical exam: short thyromental distance 1·96 (1·28–3·00) 0·002 2·72 (1·71–4·35) <0·0001
ASA status
ASA-1 Reference Reference
ASA-2 1·60 (0·44–5·74) 0·47 1·97 (0·53–7·27) 0·31
ASA-3 1·36 (0·39–4·72) 0·63 1·92 (0·54–6·85) 0·32
ASA-4 3·22 (0·89–11·57) 0·07 4·04 (1·07–15·20) 0·038
Difficult direct laryngoscopy as inclusion criteria 2·31 (1·66–3·21) <0·0001 2·01 (1·20–3·37) 0·008
(Cormack-Lehane 3–4 or failed)
First attempt device
Direct laryngoscope Reference Reference
Flexible fiberoptic bronchoscope 0·66 (0·45–0·97) 0·03 2·13 (1·19–3·81) 0·011
Glidescope 0·37 (0·22–0·63) <0·0002 0·92 (0·48–1·76) 0·79
Other device 0·80 (0·43–1·49) 0·48 1·13 (0·57–2·25) 0·72
Univariate and multivariate analysis with multiple attempts (≤2 attempts vs >2 attempts), weight (<10 kg vs ≥10 kg), American Society of Anesthesia (ASA) physical status,
Direct laryngoscopy failure or Cormack-Lehane 3–4 as inclusion criteria, and first attempt device, adjusted for site-level clustering with random-effect model. Univariate analysis
is adjusted for clustering by site. 993 cases in the multivariate analysis (ASA status was missing in 17 cases, device data was missing in eight cases and one case with ASA-5 status
completely predicted outcome, therefore dropped from analysis). Overall model was significant (p<0·0001). OR=odds ratio. ASA=American Society of Anesthesia.
Table 7: Multivariate analysis for patient, provider, and process characteristics
associations with any complication (severe or non- administration during the attempt. Facemask pre-
severe): multiple tracheal intubation attempts (>2), oxygenation is routinely done before tracheal intubation
weight less than 10 kg, short thyromental distance, and is consistent with the ASA guideline to “administer
abnormal airway physical examination, and persistent facemask pre-oxygenation before initiating management
direct laryngoscopy attempts (for the first three tracheal of a difficult airway”.20,21 The ASA further states that
intubation attempts). Multivariable analysis confirmed practitioners should “actively pursue opportunities to
the independent association of multiple attempts with deliver supplemental oxygen throughout the process of
complications (severe or non-severe). Furthermore, we difficult airway management”. Although pre-oxygenation
noted an incremental increase in the occurrence of is presumably practised, few practitioners in participating
complications with each additional tracheal intubation centres provided supplemental oxygen during the actual
attempt. intubation (10%). Children have higher oxygen
The high percentage of difficult tracheal intubations consumption rates than adults and their rate of arterial
that were anticipated (80%) probably meant that the team oxygen desaturation when apnoeic is consequently much
was prepared with the appropriate equipment and faster. This rapid desaturation rate creates a time
personnel and had information about the previously pressure to intubate these children. This pressure is
successful tracheal intubation approach. In the heightened by the common practice of intubation by
unanticipated difficult tracheal intubation group, teams trainees with senior supervision. When hypoxaemia
were probably unprepared and not ready with the occurs during tracheal intubation, the team has to
optimum equipment. Despite these population interrupt the intubation attempt to ventilate the patient.
differences, increasing attempts and lower weight were This results in more tracheal intubation attempts to
associated with more complications in both groups. secure the airway. We speculate that passive oxygen
Understandably unanticipated difficult tracheal administration during tracheal intubation might reduce
intubations had more severe complications and more the number of tracheal intubation attempts and the
tracheal intubation attempts and the attending incidence of hypoxaemia. Anaesthesiologists often
anaesthesiologist was more likely to be the successful leverage the benefits of passive oxygenation during
provider. These findings suggest that preparation matters routine anaesthetic cases such as rigid bronchoscopy for
and might lower the likelihood of severe complications. airway examinations. Passive oxygenation during rigid
Hypoxaemia was the most common non-severe bronchoscopy increases the time available for the
complication related to tracheal intubation and occurred otolaryngologist to complete the airway examination
in 9% of tracheal intubation attempts. Strategies to without oxygen desaturation. Likewise, passive
prevent hypoxaemia during tracheal intubation include oxygenation (eg, via nasal cannula, modified nasal airway
pre-oxygenation via facemask and passive oxygen or extraglottic airway) during the intubation will delay
www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1 9
Articles
the onset of hypoxaemia and provide more time for the Other investigators have shown that repeated
team to secure the tracheal tube with fewer overall intubation attempts are associated with adverse events.
tracheal intubation attempts. Passive oxygenation is Mort and colleagues25 noted that adult emergency room
effective in adults and was anecdotally reported to be patients with more than two attempts had more
effective in children with pyloric stenosis requiring rapid hypoxaemia, oesophageal intubation, and cardiac arrest.
sequence intubation; we plan to explore the effectiveness Our study examined a different population (children),
more systematically in the future.22,23 under controlled conditions (mostly elective operating
The 15 children with difficult tracheal intubation who room intubations) done by more experienced clinicians
required cardiopulmonary resuscitation for cardiac arrest (mainly paediatric anaesthesiology fellows and
translates to an incidence of one in 68 cases experiencing attendings), but the effect of more than two tracheal
cardiac arrest. This cardiac arrest incidence is substantially intubation attempts is similar. Graciano and colleagues11
higher than the 1·4 in 10 000 reported in the general also reported similar findings in the paediatric intensive
paediatric anaesthesiology population.24 11 of these care unit. Neonatal and paediatric intensive care data
procedures were non-emergent tracheal intubations in suggest that inexperienced clinicians, frequent attempts,
the operating room. This unexpectedly high incidence is and younger patients were associated with greater
a potential target for quality improvement. Reduction of complication rates. Based on our results, using a specific
hypoxaemia and persistent direct laryngoscopy, and the airway checklist may reduce adverse events in these
introduction of a protocol in which the most experienced patients. Deriving and implementing a standardised
laryngoscopist intervenes quickly when a trainee fails airway bundle checklist has been described in previous
might reduce the incidence of cardiac arrest. studies and seems like a natural progression of our
We studied cases with five tracheal intubation attempts work.26 The airway checklist could incorporate the plan to
to understand the role the device and personnel had in use an extraglottic airway early, consider and prepare for
the airway management. Standard direct laryngoscopy passive oxygenation during tracheal intubation attempts,
had a poor overall success rate (12%), but it still accounted and restrict the number of direct laryngoscopy attempts.
for 21% of fifth attempts (figure 3). Attending physicians Our study has several limitations. First, although
made only 21% of first tracheal intubation attempts and 13 paediatric centres contributed data into the registry,
yet were the successful laryngoscopist more than 44% of four large centres contributed most of the cases. The
the time indicating that they rescued the other clinicians specialised nature of the participating institutions and the
(trainee, certified registered nurse anaesthetist) proportion of cases reported by a small number of centres
frequently. If these additional attempts were for the might limit the ability to generalise the results and their
educational benefit of the trainees, the experience gained implications. Second, although we established a standard
by trainees has to be carefully weighed against the operational plan including rigorous data collection and
consequences of multiple tracheal intubation attempts. audit processes, cases could still have been missed if
The transition to the most experienced clinician should difficult tracheal intubations were not documented in
happen quickly in these patients. These data could be patient’s charts or reported by the care team. Missed cases
relevant to paediatric practitioners in other acute care could lead to under-reporting of multiple attempts or
areas including emergency departments, intensive care occurrence of complications. Furthermore tracheal
units, and intubations in the field. intubation attempts and complications data are probably
The original ASA practice guidelines for the management an under-representation of the true numbers because they
of patients with a difficult airway defined a difficult tracheal were not independently collected and were self reported
intubation as three failed conventional attempts and by the team. A video-based assessment of tracheal
recommended that subsequent attempts use alternate intubations in a paediatric emergency department showed
devices.20 Our data suggest that this guideline was often that clinicians reported fewer adverse events than were
not followed because repeated attempts with conventional recorded on independent video review. This result is
direct laryngoscopy happened in many patients (figure 3). probably a major limitation of our study and implies that
Could the use of an alternative technique after the failed we might have under-reported our complications.27 Third,
attempt expedite intubation with fewer complications? we classified training level as trainees versus attendings,
Our data showed the tracheal intubations with late and we did not capture the actual trainee’s postgraduate
transition from repeated direct laryngoscopy attempts year or whether the trainee was a resident or fellow.
were associated with higher occurrence of complications. Fourth, patients in category 4 of our inclusion criteria
Patients in category 1 had a greater proportion of overall were deemed difficult tracheal intubations at the discretion
complications than those in category 4. This finding might of the attending based on physical examination. The
suggest that patients in category 4 might have been easier anaesthesiologist did not perform direct laryngoscopy in
to intubate (their difficulty was suspected and not these patients, and it is possible that they might have been
diagnosed by direct laryngoscopy) or the fact that they did intubated easily with conventional direct laryngoscopy.
not have direct laryngoscopy translated to fewer attempts Next, our statistical analysis assumes that each of the
and less complications. 1018 tracheal intubations are independent; however, if
10 www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1
Articles
there is any dependency between tracheal intubations (eg, Participating centres
repeat patients), there might be less information in our Department of Anesthesia and Critical Care Medicine, Children’s Hospital
of Philadelphia, PA, USA; Department of Anesthesiology Perioperative and
dataset than we think. Although there were probably
Pain Medicine, Boston Children’s Hospital, Boston, MA, USA; Department
repeat patients, we believe that treating each tracheal of Anesthesiology and Pain Management, UT Southwestern Medical
intubation as independent is reasonable in view of the fact Center, Dallas, TX, USA; Department of Anesthesiology, Seattle Children’s
that the airway in children is in transition and because of Hospital, WA, USA; Department of Anesthesiology, Texas Children’s
Hospital, Houston, TX, USA; Department of Pediatric Anesthesiology,
this constant change, conditions during one tracheal University of Michigan Health Center, MI, USA; Department of
intubation can be different from a subsequent tracheal Anesthesiology, University of Texas Medical School at Houston, Houston,
intubation. This idea is well known in paediatric TX, USA; Department of Anesthesiology, Children’s Hospital of Colorado,
anaesthesia practice—eg, children with Pierre Robin CO, USA; Department of Pediatric Anesthesiology, Lurie Children’s
Hospital Chicago, Chicago, IL, USA; Department of Anesthesiology and
sequence can be extremely difficult to intubate at birth but Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA;
often become easier to intubate as they grow. Finally, we Department of Anesthesiology, the University of Mississippi Medical
estimated the rate of difficult tracheal intubation to be Center, Jackson, MI, USA; Department of Anesthesiology, Duke University,
roughly 0·2–0·5% of anaesthetic cases. Our centres Durham, NC, USA; and Department of Anesthesiology and Pain
Management, Children’s Hospital of Cleveland Clinic, Cleveland, OH, USA
tracked the number of anaesthetics done every year not
the number of tracheal intubations done in anaesthetised Declaration of interests
RG discloses patents in the public domain relevant to airway
patients. Because many patients are not intubated when management, FXM discloses grant funding from the Agency for
anaesthetised, our calculations are an approximation of Healthcare Research Quality and the Laerdal Foundation Center for
the true rate. Excellence, and AN discloses grant funding from the Agency for
In conclusion, we have defined the incidence and Healthcare Research Quality and the Laerdal Foundation Center for
Excellence. All other authors declare no competing interests.
types of complications in children with difficult tracheal
intubation across 12 paediatric centres and reported the Acknowledgments
We thank the following individuals for their contributions to this work:
tracheal intubation success rates of commonly used Bill Greeley, Mark Schreiner, Jeff Feldman, Bin Zhang, Bishr Haydar,
tracheal intubation devices and techniques. 20% of the Kenneth Peeples, Ariel Vincent, Thea Goebel, Allison Wright,
patients meeting difficult tracheal intubation criteria Shana Emery, Terri Voepel-Lewis, Sinead Rivard, Roxana Ploski,
Jennifer Spears, John Hajduk, Ranu Jain, Rachel Bernier, Mark Breibart,
had at least one complication. Taken together, we have
Stephanie Coulombre, Ian Lewis, and Jessica Burkhardt.
learned that attempting more than two tracheal
References
intubations in children with difficult tracheal intubation 1 Fiadjoe J, Stricker P. Pediatric difficult airway management:
is associated with a high failure rate and increased current devices and techniques. Anesthesiol Clin 2009; 27: 185–95.
incidence of complications. This high complication rate 2 Fiadjoe JE, Gurnaney H, Dalesio N, et al. A prospective randomized
is multifactorial in origin. The patient-level factors equivalence trial of the GlideScope Cobalt® video laryngoscope to
traditional direct laryngoscopy in neonates and infants.
include abnormal airway physical examination and Anesthesiology 2012; 116: 622–28.
lower patient age and weight. Process factors included 3 Vanderhal AL, Berci G, Simmons CF Jr, Hagiike M.
multiple tracheal intubation attempts and multiple A videolaryngoscopy technique for the intubation of the newborn:
preliminary report. Pediatrics 2009; 124: e339–46.
direct laryngoscopy attempts. Additionally, delays in 4 Long E, Sabato S, Babl FE. Endotracheal intubation in the pediatric
transition from trainee to attending tracheal intubation emergency department. Paediatr Anaesth 2014; 24: 1204–11.
attempts could have contributed to complications. We 5 Morray JP, Geiduschek JM, Caplan RA, Posner KL, Gild WM,
Cheney FW. A comparison of pediatric and adult anesthesia closed
are now poised to create and disseminate a quality malpractice claims. Anesthesiology 1993; 78: 461–67.
improvement bundle to address these complications 6 Jimenez N, Posner KL, Cheney FW, Caplan RA, Lee LA,
across our centres. Our findings should affect the clinical Domino KB. An update on pediatric anesthesia liability: a closed
claims analysis. Anesth Analg 2007; 104: 147–53.
decisions of all clinicians who perform this potentially
7 Cook TM, Woodall N, Harper J, Benger J, and the Fourth National
life-saving procedure in children with difficult tracheal Audit Project. Major complications of airway management in the
intubation. UK: results of the Fourth National Audit Project of the Royal College
of Anaesthetists and the Difficult Airway Society. Part 2: intensive
Contributors care and emergency departments. Br J Anaesth 2011; 106: 632–42.
JEF, NJ, DMP, MEM, PS, VMN, FXM, RSL, MAR, PGK, PIR, and AIH 8 Cook TM, Woodall N, Frerk C, and the Fourth National Audit
contributed to manuscript authorship, study design, data interpretation, Project. Major complications of airway management in the UK:
and data contribution; AN contributed to statistical analysis, study results of the Fourth National Audit Project of the Royal College of
design, data interpretation, and data contribution; and RSG contributed Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia.
to manuscript authorship, study design, and data interpretation. Br J Anaesth 2011; 106: 617–31.
PeDI collaborative group 9 Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics.
Anaesthesia 1984; 39: 1105–11.
Paul Stricker, Brad Taicher, Vidya Raman, Ralph Beltran, Ian Lewis,
Bishr Haydar, Prabhat Koppera, Shobha Malviya, Katherine Gentry, 10 Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG.
Research electronic data capture (REDCap)--a metadata-driven
Adrian Bosenberg, Patrick Olomu, Edgar Kiss, Judit Szolnoki,
methodology and workflow process for providing translational
Jennifer Zieg, Madhankumar Sathyamoorthy, Vikram Patel, research informatics support. J Biomed Inform 2009; 42: 377–81.
Codruta Soneru, Ricardo Falcon, Jimmy Windsor, Tim Peterson,
11 Graciano AL, Tamburro R, Thompson AE, Fiadjoe J, Nadkarni VM,
Raymond Park, James Peyton, Denise Chan, Chris Glover, Paul Hopkins, Nishisaki A. Incidence and associated factors of difficult tracheal
Somaletha T Bhattacharya, Ricardo Riveros, Nicholas Dalesio, intubations in pediatric ICUs: a report from National Emergency
Martina Richtsfeld, Kumar Belani, Bin Zhang, John McCloskey, Airway Registry for Children: NEAR4KIDS. Intensive Care Med 2014;
Olutoyin A Olutoye, Christopher Estrada, and Tarun Bhalla. 40: 1659–69.
www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1 11
Articles
12 Nishisaki A, Turner DA, Brown CA 3rd, Walls RM, Nadkarni VM, 22 Bhagwan SD. Levitan’s no desat with nasal cannula for infants with
and the National Emergency Airway Registry for Children pyloric stenosis requiring intubation. Paediatr Anaesth 2013;
(NEAR4KIDS), and the Pediatric Acute Lung Injury and Sepsis 23: 297–98.
Investigators (PALISI) Network. A National Emergency Airway 23 Wimalasena Y, Burns B, Reid C, Ware S, Habig K. Apneic
Registry for children: landscape of tracheal intubation in 15 PICUs. oxygenation was associated with decreased desaturation rates
Crit Care Med 2013; 41: 874–85. during rapid sequence intubation by an Australian helicopter
13 Han R, Tremper KK, Kheterpal S, O’Reilly M. Grading scale for emergency medicine service. Ann Emerg Med 2015; 65: 371–76.
mask ventilation. Anesthesiology 2004; 101: 267. 24 Morray JP, Geiduschek JM, Ramamoorthy C, et al. Anesthesia-
14 Benumof JL, Dagg R, Benumof R. Critical hemoglobin desaturation related cardiac arrest in children: initial findings of the Pediatric
will occur before return to an unparalyzed state following 1 mg/kg Perioperative Cardiac Arrest (POCA) Registry. Anesthesiology 2000;
intravenous succinylcholine. Anesthesiology 1997; 87: 979–82. 93: 6–14.
15 Denman WT, Goudsouzian NG. Position of the laryngeal mask 25 Mort TC. Emergency tracheal intubation: complications associated
airway. Anesthesiology 1992; 77: 401–02. with repeated laryngoscopic attempts. Anesth Analg 2004;
16 Dubreuil M, Laffon M, Plaud B, Penon C, Ecoffey C. Complications 99: 607–13.
and fiberoptic assessment of size 1 laryngeal mask airway. 26 Li S, Rehder KJ, Giuliano JS Jr, et al, and the National Emergency
Anesth Analg 1993; 76: 527–29. Airway Registry for Children (NEAR4KIDS) Investigators and
17 Park C, Bahk JH, Ahn WS, Do SH, Lee KH. The laryngeal mask Pediatric Acute Lung Injury and Sepsis Investigator (PALISI)
airway in infants and children. Can J Anaesth 2001; 48: 413–17. Network Investigators. Development of a quality improvement
18 Duggan LJN. Unique airway issues in the pediatric population: bundle to reduce tracheal intubation-associated events in pediatric
McGraw Hill, 2012. ICUs. Am J Med Qual 2014; published online Aug 20.
DOI:10.1177/1062860614547259.
19 Sankar A, Johnson SR, Beattie WS, Tait G, Wijeysundera DN.
Reliability of the American Society of Anesthesiologists physical 27 Kerrey BT, Rinderknecht AS, Geis GL, Nigrovic LE, Mittiga MR.
status scale in clinical practice. Br J Anaesth 2014; 113: 424–32. Rapid sequence intubation for pediatric emergency patients: higher
frequency of failed attempts and adverse effects found by video
20 Practice guidelines for management of the difficult airway. A report
review. Ann Emerg Med 2012; 60: 251–59.
by the American Society of Anesthesiologists Task Force on
Management of the Difficult Airway. Anesthesiology 1993; 78: 597–602.
21 Apfelbaum JL, Hagberg CA, Caplan RA, et al, and the American
Society of Anesthesiologists Task Force on Management of the
Difficult Airway. Practice guidelines for management of the difficult
airway: an updated report by the American Society of
Anesthesiologists Task Force on Management of the Difficult
Airway. Anesthesiology 2013; 118: 251–70.
12 www.thelancet.com/respiratory Published online December 16, 2015 http://dx.doi.org/10.1016/S2213-2600(15)00508-1
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Region X: January 1, 2021 Advanced Life Support Standard Operating ProceduresДокумент126 страницRegion X: January 1, 2021 Advanced Life Support Standard Operating ProceduresC ScribОценок пока нет
- Or NCP (Risk For Infection)Документ1 страницаOr NCP (Risk For Infection)Nikki M. Arapol100% (1)
- NAET Infor GuideДокумент7 страницNAET Infor GuideAlejo Ribas SalaОценок пока нет
- University College of DublinДокумент2 страницыUniversity College of DublinDawitОценок пока нет
- NP2 Pre Board Practice TestДокумент12 страницNP2 Pre Board Practice TestErickaОценок пока нет
- Assessment of DiaphragmaticДокумент10 страницAssessment of DiaphragmaticFranco BongiornoОценок пока нет
- Stroke Mimics: Clinical and Radiological Evaluation: Poster No.: Congress: Type: Authors: KeywordsДокумент20 страницStroke Mimics: Clinical and Radiological Evaluation: Poster No.: Congress: Type: Authors: KeywordsOrlin ZlatarskiОценок пока нет
- Bleeding Disorder (Paediatrics)Документ95 страницBleeding Disorder (Paediatrics)Nurul Afiqah Mohd YusoffОценок пока нет
- VerA Ok-Prelim Ncm104 (Autosaved) VeraДокумент30 страницVerA Ok-Prelim Ncm104 (Autosaved) Verajesperdomincilbayaua100% (1)
- Apollo Hospitals FinalДокумент19 страницApollo Hospitals Finalakash_shah_42Оценок пока нет
- A.Chn As A Field of Nursing PracticeДокумент1 страницаA.Chn As A Field of Nursing PracticeHanna LopezОценок пока нет
- Azhar Husain, AL Shifa CaseДокумент10 страницAzhar Husain, AL Shifa CaseAzhar Hussain (Father Name:Imtiaz Ahmed)Оценок пока нет
- Fractures Pathophysiology Treatment and Nursing CareДокумент9 страницFractures Pathophysiology Treatment and Nursing Careaddica0% (1)
- UTI Prevention Fact SheetДокумент1 страницаUTI Prevention Fact Sheetalifia alqibtiaОценок пока нет
- (JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsДокумент7 страниц(JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsAurellia Annisa WulandariОценок пока нет
- Javma-Javma 21 04 0213Документ5 страницJavma-Javma 21 04 0213Black manОценок пока нет
- COVID-19: Impact On The Population, The Mental Health of Society and Mental Health NursesДокумент2 страницыCOVID-19: Impact On The Population, The Mental Health of Society and Mental Health NursesShubhanshu DhakalОценок пока нет
- Daftar Pustaka: ND NDДокумент1 страницаDaftar Pustaka: ND NDCherylina GraceОценок пока нет
- Chilaiditi Syndrom in Child Diagnostic Trap (Case Report)Документ6 страницChilaiditi Syndrom in Child Diagnostic Trap (Case Report)IJAR JOURNALОценок пока нет
- Profile: Doris A. MendozaДокумент4 страницыProfile: Doris A. MendozaGerarld Immanuel KairupanОценок пока нет
- BMED - Lab ReportДокумент7 страницBMED - Lab ReportDaniella Stevanato SanchezОценок пока нет
- Dyskinesia FACT SHEETДокумент2 страницыDyskinesia FACT SHEETRatnaPrasadNalamОценок пока нет
- Stages in Behavior ChangeДокумент4 страницыStages in Behavior ChangeArbab Usman KhanОценок пока нет
- Vibrio Cholerae PosterДокумент1 страницаVibrio Cholerae PosterStela MonkОценок пока нет
- Liu 2017-Herbal Medicine For The Treatment of ObesityДокумент17 страницLiu 2017-Herbal Medicine For The Treatment of ObesityMas NuriОценок пока нет
- Manesar Design Competition NoticeДокумент15 страницManesar Design Competition NoticeAsna DTОценок пока нет
- Johannesson 2004Документ13 страницJohannesson 2004Faeyz OrabiОценок пока нет
- Laporan Praktikum Evidence Based Medicine (EBM)Документ13 страницLaporan Praktikum Evidence Based Medicine (EBM)LalaОценок пока нет
- CTCAE v5.0Документ401 страницаCTCAE v5.0EdОценок пока нет
- Effects of Mouthpiece Use On Airway Openings and Lactate LevelsДокумент6 страницEffects of Mouthpiece Use On Airway Openings and Lactate LevelsFábio LopesОценок пока нет