Вам также может понравиться
- 2017 Article 2060Документ8 страниц2017 Article 2060Indira SellyОценок пока нет
- BMC Public HealthДокумент8 страницBMC Public HealthAnselmo MatusseОценок пока нет
- Jurnal Bhs InggrisДокумент2 страницыJurnal Bhs InggrisAlda SafitriОценок пока нет
- Dengue in CambodiaДокумент10 страницDengue in CambodiaRobert BennettОценок пока нет
- Tugas Ulang Metodologi PenelitianДокумент55 страницTugas Ulang Metodologi PenelitianMuhammad Candra R.AОценок пока нет
- Treatment OutcomesДокумент7 страницTreatment OutcomestarisafidiaОценок пока нет
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaДокумент12 страницChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaОценок пока нет
- JurnalДокумент7 страницJurnalyenni elfiraОценок пока нет
- Factors Associated With Severe Malaria in Children Under Five Years of Age at Mbarara Regional Referral Hospital, UgandaДокумент12 страницFactors Associated With Severe Malaria in Children Under Five Years of Age at Mbarara Regional Referral Hospital, UgandaKIU PUBLICATION AND EXTENSIONОценок пока нет
- Tropical Infections SymposiumДокумент79 страницTropical Infections SymposiumVishwaCrОценок пока нет
- The Healthcare Needs of Families Caring For Patients With Pulmonary TuberculosisДокумент8 страницThe Healthcare Needs of Families Caring For Patients With Pulmonary TuberculosisINTAN MADULARAОценок пока нет
- Knowledge, Attitude and Practice of Mothers With Children Less Than Five Years Toward Vaccination in Khartoum State-Ummbada Locality-Allbugaa-2017Документ4 страницыKnowledge, Attitude and Practice of Mothers With Children Less Than Five Years Toward Vaccination in Khartoum State-Ummbada Locality-Allbugaa-2017krishnasree100% (1)
- Tazinya 2018Документ8 страницTazinya 2018Risnawati PurbaОценок пока нет
- Jurnal 10 HariantoДокумент7 страницJurnal 10 Hariantoaryzamelindah channelОценок пока нет
- Out 17Документ10 страницOut 17laodesyuhadarОценок пока нет
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoДокумент20 страницMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriОценок пока нет
- Adiutarini 2Документ7 страницAdiutarini 2Eva Tirtabayu HasriОценок пока нет
- Why Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniaДокумент10 страницWhy Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniajlventiganОценок пока нет
- Exploring Women Knowledge of Newborn Danger Signs: A Case of Mothers With Under Five ChildrenДокумент8 страницExploring Women Knowledge of Newborn Danger Signs: A Case of Mothers With Under Five ChildrenJohnjohn MateoОценок пока нет
- Final Copy (Tipdas) 111Документ80 страницFinal Copy (Tipdas) 111Zachary Bañez100% (1)
- Factors Associated With Malaria Infection in Mudzi District, Mashonaland East Zimbabwe, 2019: A Case-Control StudyДокумент9 страницFactors Associated With Malaria Infection in Mudzi District, Mashonaland East Zimbabwe, 2019: A Case-Control StudyRizka Mulia FebriantiОценок пока нет
- Faktor Resiko PneumoniaДокумент13 страницFaktor Resiko PneumoniaintandiahningrumОценок пока нет
- Health Impact Framework Paper Nur 310Документ9 страницHealth Impact Framework Paper Nur 310api-726326591Оценок пока нет
- Ijerph 16 03752Документ10 страницIjerph 16 03752Angel Ellene MarcialОценок пока нет
- Impact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityДокумент9 страницImpact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDebby Astasya AnnisaОценок пока нет
- JournalДокумент13 страницJournalYasin HrОценок пока нет
- Quinine Thin Film DosageДокумент13 страницQuinine Thin Film DosageStephen Yao GbedemaОценок пока нет
- Related-LitДокумент4 страницыRelated-LitBianca Alexy MataОценок пока нет
- 2019 Article 4497 PDFДокумент13 страниц2019 Article 4497 PDFsanita putriОценок пока нет
- BongДокумент1 страницаBongRod Reynon BorceОценок пока нет
- Child Health and TBДокумент3 страницыChild Health and TBsoukumar8305Оценок пока нет
- Franck2014 Article AssessingTheImpactOfMultidrugДокумент10 страницFranck2014 Article AssessingTheImpactOfMultidrugFarrell AnggoroОценок пока нет
- Factors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsДокумент14 страницFactors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsAnonymous QPXAgjBwОценок пока нет
- Reported Incidence of Fever For Under-5 Children in Zambia: A Longitudinal StudyДокумент7 страницReported Incidence of Fever For Under-5 Children in Zambia: A Longitudinal StudyBassim BirklandОценок пока нет
- EPI.2006.Unger - Tmih.can Malaria Be Controlled Where Basic Health Services Are Not UsedДокумент9 страницEPI.2006.Unger - Tmih.can Malaria Be Controlled Where Basic Health Services Are Not UsedderekwwillisОценок пока нет
- Research On Prevalence of TB FinalДокумент9 страницResearch On Prevalence of TB FinalBontuОценок пока нет
- 2017 Article 2184Документ11 страниц2017 Article 2184diana sulistianОценок пока нет
- Dengue KAPДокумент9 страницDengue KAPElinОценок пока нет
- Understanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoДокумент16 страницUnderstanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoKarina ChristantoОценок пока нет
- Barriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVДокумент15 страницBarriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVKIU PUBLICATION AND EXTENSIONОценок пока нет
- 2020 Article 5324Документ8 страниц2020 Article 5324Sorina ElenaОценок пока нет
- Mothers' Knowledge and Attitudes Towards Child Immunization in GeorgiaДокумент7 страницMothers' Knowledge and Attitudes Towards Child Immunization in Georgiagabb bbОценок пока нет
- Comparison of Antiretroviral Therapy Adherence Among HIV Infected Older Adults With Younger Adults in Africa: Systematic Review and Meta AnalysisДокумент14 страницComparison of Antiretroviral Therapy Adherence Among HIV Infected Older Adults With Younger Adults in Africa: Systematic Review and Meta AnalysisCliff Daniel DIANZOLE MOUNKANAОценок пока нет
- Lessons Learned From COVID-19 Impact of Pandemic On Children With Neurological Disorders in Sfax, TunisiaДокумент13 страницLessons Learned From COVID-19 Impact of Pandemic On Children With Neurological Disorders in Sfax, TunisiaIJPHSОценок пока нет
- Integrating Severe Acute Malnutrition Into The Management of Childhood Diseases at Community Level in South SudanДокумент36 страницIntegrating Severe Acute Malnutrition Into The Management of Childhood Diseases at Community Level in South Sudanmalaria_consortium100% (1)
- Pharmaceutical Sciences: Factors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsДокумент6 страницPharmaceutical Sciences: Factors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsMehreen KhanОценок пока нет
- Maternal ThesisДокумент10 страницMaternal ThesisMerwynmae PobletinОценок пока нет
- My ProjectДокумент38 страницMy ProjectfaizamuhammadaligmlОценок пока нет
- Essential Newborn Care Practice at Four Primary Health Facilities in Conflict Affected Areas of Bossaso Somalia A Cross Sectional StudyДокумент13 страницEssential Newborn Care Practice at Four Primary Health Facilities in Conflict Affected Areas of Bossaso Somalia A Cross Sectional StudyROBLE ABDIОценок пока нет
- TB Complain Ce PM PJДокумент8 страницTB Complain Ce PM PJAnonymous QPXAgjBwОценок пока нет
- Ijisr 19 017 04Документ8 страницIjisr 19 017 04patrick NKAMEDJIEОценок пока нет
- 3 Non Adherence and Its Contributing PDFДокумент9 страниц3 Non Adherence and Its Contributing PDFODONG MARTINОценок пока нет
- 2016 Article 1588Документ12 страниц2016 Article 1588ArcciPradessatamaОценок пока нет
- Malaria Among The Geriatric Population in Parts of Southeastern Nigeriaprevalence Complications and Comorbidity With Noncommunicab 2161Документ6 страницMalaria Among The Geriatric Population in Parts of Southeastern Nigeriaprevalence Complications and Comorbidity With Noncommunicab 2161Sarah HumayraОценок пока нет
- 11 Jurnal Surya 2017Документ9 страниц11 Jurnal Surya 2017Charis MurwadiОценок пока нет
- Dengue Kap AcceptedДокумент28 страницDengue Kap AcceptedClarise Vera Simangan NabennegОценок пока нет
- Peer Facilitators's Role To Support Pregnant Women in Utilizing HIV Services During The COVID-19 PandemicДокумент8 страницPeer Facilitators's Role To Support Pregnant Women in Utilizing HIV Services During The COVID-19 PandemicIJPHSОценок пока нет
- Journal of Clinical Tuberculosis and Other Mycobacterial DiseasesДокумент16 страницJournal of Clinical Tuberculosis and Other Mycobacterial DiseasesIlna RamadhaniОценок пока нет
- Vaccines: Making the Right Choice for Your ChildОт EverandVaccines: Making the Right Choice for Your ChildРейтинг: 5 из 5 звезд5/5 (2)
- Coronavirus Disease 2019: Covid-19 Pandemic, States of Confusion and Disorderliness of the Public Health Policy-making ProcessОт EverandCoronavirus Disease 2019: Covid-19 Pandemic, States of Confusion and Disorderliness of the Public Health Policy-making ProcessОценок пока нет
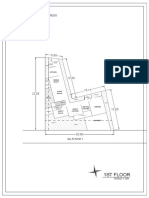
- 1St Floor: House On Paus Schematic Plan ProgressДокумент2 страницы1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaОценок пока нет
- Medicalscience: EcancerДокумент7 страницMedicalscience: Ecancerfiora.ladesvitaОценок пока нет
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyДокумент11 страницSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaОценок пока нет
- Gibson 2010Документ19 страницGibson 2010fiora.ladesvitaОценок пока нет
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaДокумент12 страницChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaОценок пока нет
- Assessment Rating ScaleДокумент8 страницAssessment Rating Scalefiora.ladesvitaОценок пока нет
- Ambulatory Care Nursing: Coming Soon!Документ16 страницAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaОценок пока нет
- 2015 Conference 10Документ11 страниц2015 Conference 10fiora.ladesvitaОценок пока нет
- Anderson2004 PDFДокумент7 страницAnderson2004 PDFfiora.ladesvitaОценок пока нет
- Sistematic Review HoneyДокумент159 страницSistematic Review Honeyfiora.ladesvitaОценок пока нет
- Idiom Meaning Examples: Toefl PreparationДокумент4 страницыIdiom Meaning Examples: Toefl Preparationfiora.ladesvitaОценок пока нет
- Living With Kidney DiseaseДокумент96 страницLiving With Kidney Diseasefiora.ladesvitaОценок пока нет
- Caring: Prof. Dr. Budi Anna Keliat, MappscДокумент59 страницCaring: Prof. Dr. Budi Anna Keliat, Mappscfiora.ladesvitaОценок пока нет
- SyllabusДокумент3 страницыSyllabusAditya KoutharapuОценок пока нет
- DLL - DressmakingДокумент3 страницыDLL - DressmakingCatherine SantistebanОценок пока нет
- TH e Problems of Geography EducationДокумент12 страницTH e Problems of Geography EducationLux King TanggaОценок пока нет
- Supervisory Plan: School ID: 501222 Poonbato IS 09455370326 501222pis@deped - Gov.phДокумент2 страницыSupervisory Plan: School ID: 501222 Poonbato IS 09455370326 501222pis@deped - Gov.phBryan JesterОценок пока нет
- 2016 Critical Reflection For ISCORE 2 - Purposeful DesignДокумент3 страницы2016 Critical Reflection For ISCORE 2 - Purposeful DesignFrancis Ho HoОценок пока нет
- Times Leader 05-07-2011Документ60 страницTimes Leader 05-07-2011The Times LeaderОценок пока нет
- Somnath Hore BioДокумент3 страницыSomnath Hore BioLukepouОценок пока нет
- 04 Expressing Satisfaction & Dissatisfaction - ExerciseДокумент2 страницы04 Expressing Satisfaction & Dissatisfaction - ExerciseMarcello AntonyОценок пока нет
- Outline of Rizal's Life 2Документ73 страницыOutline of Rizal's Life 2Reyji Edduba100% (1)
- Activity 1Документ2 страницыActivity 1Mary Alejandra Ipanaque CarrascoОценок пока нет
- 0510 s18 QP 21 PDFДокумент16 страниц0510 s18 QP 21 PDFChernYangEeОценок пока нет
- Weekly Home Learning Plan Grade 4 Learning Area: English Quarter 3 Week No. 2 Date Covered: April 12-16, 2021Документ4 страницыWeekly Home Learning Plan Grade 4 Learning Area: English Quarter 3 Week No. 2 Date Covered: April 12-16, 2021Eman CastañedaОценок пока нет
- Script Parents Orientation Online Summer TUtorial 1Документ2 страницыScript Parents Orientation Online Summer TUtorial 1Herbrey Madrigal100% (2)
- Dhanasekaran Covering LeterДокумент10 страницDhanasekaran Covering LeterAgotОценок пока нет
- Activity 1Документ4 страницыActivity 1Joy Kimberly PaglinawanОценок пока нет
- National Policy On Education (NPE 1986)Документ11 страницNational Policy On Education (NPE 1986)deepak kumarОценок пока нет
- School Memo FGD On Preparation of LCOPДокумент8 страницSchool Memo FGD On Preparation of LCOPShara Jane Sayco SamonteОценок пока нет
- Teacher Book For All TogetherДокумент48 страницTeacher Book For All TogetherJessa Mae Mangubat57% (7)
- Ethical TheoriesДокумент5 страницEthical TheoriesRJ De JesusОценок пока нет
- No1 Answer: D: Soal Try Out Pemprov Paket BДокумент14 страницNo1 Answer: D: Soal Try Out Pemprov Paket BArul Hidayat0% (1)
- Resume Saima Zakir OomerДокумент2 страницыResume Saima Zakir OomerYasi HanifОценок пока нет
- 16th Note Lesson PlanДокумент3 страницы16th Note Lesson Planapi-273160985100% (1)
- 4 Complete Punnett Square LessonДокумент39 страниц4 Complete Punnett Square Lessonapi-312176473Оценок пока нет
- CLD 2021 SCRD v2 Writing Presentation 211015Документ40 страницCLD 2021 SCRD v2 Writing Presentation 211015api-288934833Оценок пока нет
- Chapter 12 NotesДокумент2 страницыChapter 12 Notesapi-262383789Оценок пока нет
- GROUP 7 FAN Technique PVR by MEGILYN T. HOLMANДокумент26 страницGROUP 7 FAN Technique PVR by MEGILYN T. HOLMANMhel KilaОценок пока нет
- Gasal E FormДокумент10 страницGasal E FormMuhammad Nauman Hafeez KhanОценок пока нет
- Mohali Education Board PDFДокумент12 страницMohali Education Board PDFDEVANDRA CHOUDHARYОценок пока нет
- Academic Performance of TVLДокумент8 страницAcademic Performance of TVLEurica Mae M. NabongОценок пока нет
- MCAT 2017 May-2018 Apr Percentiles PDFДокумент2 страницыMCAT 2017 May-2018 Apr Percentiles PDFBarry HeadОценок пока нет