Вам также может понравиться
- Schizoaffective Disorder FactsheetДокумент16 страницSchizoaffective Disorder FactsheetVictoria AdhityaОценок пока нет
- Covid19 Banerji ProtocolДокумент3 страницыCovid19 Banerji ProtocolAga Kiermasz100% (4)
- Management of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesДокумент10 страницManagement of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesArizkamhОценок пока нет
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Документ1 страницаWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Malisa LukmanОценок пока нет
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Документ1 страницаWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Malisa LukmanОценок пока нет
- Management of Circumscript NeurodermatitisДокумент12 страницManagement of Circumscript NeurodermatitisRoy Prabowo SarumpaetОценок пока нет
- Causes, Symptoms and Treatment of ChorioretinitisДокумент13 страницCauses, Symptoms and Treatment of Chorioretinitisrada tri rosi kurniaОценок пока нет
- Hidradenitis SupuratifДокумент12 страницHidradenitis SupuratifRielz ThereaperzОценок пока нет
- COVID-19 - Informative EssayДокумент1 страницаCOVID-19 - Informative EssayRydl Pnp100% (1)
- Icd XДокумент3 страницыIcd XR Ghianesya GantinaОценок пока нет
- Kamus Icd 10 Dan Icd 9Документ10 страницKamus Icd 10 Dan Icd 9trisnawati100% (1)
- Tinea UnguiumДокумент8 страницTinea UnguiumwirdahajaОценок пока нет
- Topical Treatment of Common Superficial Tinea InfectionsДокумент8 страницTopical Treatment of Common Superficial Tinea InfectionsColate LocoОценок пока нет
- Humeral Shaft Fracture DiscussionДокумент18 страницHumeral Shaft Fracture DiscussionRushdaОценок пока нет
- Gnaps EmedicineДокумент13 страницGnaps Emedicineharyanti lupitaОценок пока нет
- Episkleritis N Skleritis EditДокумент12 страницEpiskleritis N Skleritis EditAnonymous HgX3mN1oОценок пока нет
- Differential Diagnosis of Rash Illness: Disease Sign/Symptoms Type of Rash Other FeaturesДокумент2 страницыDifferential Diagnosis of Rash Illness: Disease Sign/Symptoms Type of Rash Other FeaturesCarlo CondeОценок пока нет
- Otitis Media AkutДокумент30 страницOtitis Media Akutindah sariОценок пока нет
- Dermatological Infection Management UpdateДокумент29 страницDermatological Infection Management UpdateyheyenОценок пока нет
- Tinea BarbaeДокумент4 страницыTinea BarbaeKevin EdroОценок пока нет
- Basic Radiology PDFДокумент104 страницыBasic Radiology PDFsimona mariana dutu100% (1)
- Larynx InfectionsДокумент28 страницLarynx InfectionsMuskan GogiaОценок пока нет
- Patch Test ROAT PDFДокумент9 страницPatch Test ROAT PDFrochmandrg dokter gigiОценок пока нет
- Mallory Weiss TearДокумент12 страницMallory Weiss TeararshadmunОценок пока нет
- External Hordeolum OD: Oleh: A.A.A Lie Lhianna M.P H1A013001Документ25 страницExternal Hordeolum OD: Oleh: A.A.A Lie Lhianna M.P H1A013001Liliana MpОценок пока нет
- MiliariaДокумент6 страницMiliariaZyzah HasibuanОценок пока нет
- Vesicolithiasis BSHДокумент24 страницыVesicolithiasis BSHBobby Faisyal RakhmanОценок пока нет
- Pathogenesis of Systemic Sclerosis Scleroderma UpToDateДокумент27 страницPathogenesis of Systemic Sclerosis Scleroderma UpToDateLê Hạ Long HảiОценок пока нет
- Diagnosis Banding Konjungtivitis And EpiskleritisДокумент1 страницаDiagnosis Banding Konjungtivitis And EpiskleritisMa Rani HaОценок пока нет
- Cardiac Tamponade Diagnosis and TreatmentДокумент14 страницCardiac Tamponade Diagnosis and TreatmentAmin SiagianОценок пока нет
- Cor PulmonaleДокумент14 страницCor PulmonaleEvangelin MelvinОценок пока нет
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Документ14 страницReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaОценок пока нет
- Disorders of the Skin Appendages ExplainedДокумент8 страницDisorders of the Skin Appendages ExplainednandablaguОценок пока нет
- Ir-024 GangreneДокумент5 страницIr-024 GangreneMuhammad ShakeelОценок пока нет
- Drug Eruption Fix PrintДокумент30 страницDrug Eruption Fix PrintAshari MohpulОценок пока нет
- Alopecia AreataДокумент13 страницAlopecia AreataAchoonk RamadhanОценок пока нет
- DRUG ERUPTION GUIDEДокумент46 страницDRUG ERUPTION GUIDESyahDikaОценок пока нет
- Cutaneous Lupus ErythematosusДокумент15 страницCutaneous Lupus ErythematosusErika KusumawatiОценок пока нет
- Journal ReadingДокумент18 страницJournal ReadingnafisyarifahОценок пока нет
- Responsi Spontan PneumothoraxДокумент49 страницResponsi Spontan PneumothoraxNizarAbdullahОценок пока нет
- Referat CTSДокумент32 страницыReferat CTStrikurniati27Оценок пока нет
- OphthalmoplegiaДокумент5 страницOphthalmoplegiaPatricia Feliani SitohangОценок пока нет
- Refrst Sindrom KompartementДокумент28 страницRefrst Sindrom Kompartementdesti cahyantiОценок пока нет
- Neoplasma MataДокумент65 страницNeoplasma MataFadilah NSОценок пока нет
- Journal Reading THT - OMAДокумент15 страницJournal Reading THT - OMAIndira MaycellaОценок пока нет
- 13 - 266fourniers Gangrene PDFДокумент5 страниц13 - 266fourniers Gangrene PDFMochamad RizalОценок пока нет
- MILIARIAДокумент6 страницMILIARIARien Anggraini RazakОценок пока нет
- REFERAT Cluster HeadacheДокумент39 страницREFERAT Cluster HeadacheSafitriОценок пока нет
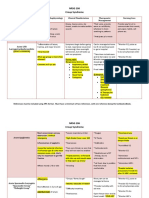
- NRSG 206 Croup SyndromeДокумент3 страницыNRSG 206 Croup SyndromeGirlwithnonameОценок пока нет
- CLARA SKIN Who PDFДокумент154 страницыCLARA SKIN Who PDFhasnul ramadhaniОценок пока нет
- Cor Pulmonale - StatPearls - NCBI BookshelfДокумент4 страницыCor Pulmonale - StatPearls - NCBI BookshelfAldi RafaelОценок пока нет
- Pityriasis Rosea PatogenesisДокумент4 страницыPityriasis Rosea PatogenesisAdrian KuswantoОценок пока нет
- Jurnal AcneДокумент5 страницJurnal AcneStacy VaniaОценок пока нет
- Review Article Bombax Ceiba Linn. Pharma PDFДокумент8 страницReview Article Bombax Ceiba Linn. Pharma PDFpankaj chaudharyОценок пока нет
- Ventikular Septal Defect FixДокумент18 страницVentikular Septal Defect FixPutri Sari DewiОценок пока нет
- Case Report OMEДокумент8 страницCase Report OMEYosephine ninaОценок пока нет
- Continuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress SyndromeДокумент4 страницыContinuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress Syndromelaudya100% (1)
- Hordeolum - Background, Pathophysiology, EpidemiologyДокумент6 страницHordeolum - Background, Pathophysiology, EpidemiologyKeren SingamОценок пока нет
- Status Kalazion - Yoga 1161050136Документ10 страницStatus Kalazion - Yoga 1161050136Yoga WitularОценок пока нет
- Diagnosing Psoriatic ArthritisДокумент4 страницыDiagnosing Psoriatic ArthritisgunnasundaryОценок пока нет
- Laporan Kasus Sindroma NefrotikДокумент13 страницLaporan Kasus Sindroma NefrotikZenithaMeidaОценок пока нет
- Life-Threatening Cellulitis of the Floor of the MouthДокумент17 страницLife-Threatening Cellulitis of the Floor of the Mouthlutfia papitaОценок пока нет
- Pityriasis RoseaДокумент20 страницPityriasis RoseaMendy Herianto100% (1)
- Tinea Korporis FitzpatrickДокумент2 страницыTinea Korporis FitzpatrickAstri MelistriОценок пока нет
- Epidemiology.: Fig. 188-9AДокумент2 страницыEpidemiology.: Fig. 188-9AintanphОценок пока нет
- Translate TineaДокумент12 страницTranslate TineaIndah Permata SariОценок пока нет
- Abn Abn0000119Документ10 страницAbn Abn0000119Baharudin Yusuf RamadhaniОценок пока нет
- NeuroДокумент13 страницNeuroAkhdan AufaОценок пока нет
- NeuroДокумент13 страницNeuroAkhdan AufaОценок пока нет
- HematokritДокумент5 страницHematokritSamanuddin ManawariОценок пока нет
- Jurnal 1Документ8 страницJurnal 1AndiTriciliaDwiPuspaОценок пока нет
- 612 1206 1 SMДокумент9 страниц612 1206 1 SMAndiTriciliaDwiPuspaОценок пока нет
- 12 13 20 1 10 20161201Документ4 страницы12 13 20 1 10 20161201AndiTriciliaDwiPuspaОценок пока нет
- En 15Документ5 страницEn 15AndiTriciliaDwiPuspaОценок пока нет
- 12 13 20 1 10 20161201Документ4 страницы12 13 20 1 10 20161201AndiTriciliaDwiPuspaОценок пока нет
- C 35 eДокумент4 страницыC 35 eAndiTriciliaDwiPuspaОценок пока нет
- En 15Документ5 страницEn 15AndiTriciliaDwiPuspaОценок пока нет
- J. Surg. Case Rep.-2012-Ihedioha-4 PDFДокумент6 страницJ. Surg. Case Rep.-2012-Ihedioha-4 PDFAngga PrabawaОценок пока нет
- NCP For HemorrhoidsДокумент3 страницыNCP For HemorrhoidsTADURAN RENE MAE ANGELLI F.Оценок пока нет
- Physician Certification FormДокумент2 страницыPhysician Certification FormSachin Tukaram SalianОценок пока нет
- Does Drinking Coffee Really Bad for Health? The Benefits Outweigh the RisksДокумент1 страницаDoes Drinking Coffee Really Bad for Health? The Benefits Outweigh the Riskswahyu kencanaОценок пока нет
- LeptospirosisДокумент33 страницыLeptospirosisVyramuthu AtputhanОценок пока нет
- Journal Reading CKDДокумент19 страницJournal Reading CKDSyah Muhammad RezaОценок пока нет
- Respiratory Infection During PregnancyДокумент11 страницRespiratory Infection During PregnancyKubra ĖdrisОценок пока нет
- Ocd 1Документ18 страницOcd 1api-584576706Оценок пока нет
- Serologicchartv 8Документ1 страницаSerologicchartv 8Gautamu ZalavadiyaОценок пока нет
- Microbiology and Parasitology - Activity 4 The Control of DiseaseДокумент3 страницыMicrobiology and Parasitology - Activity 4 The Control of DiseaseClaro M. GarchitorenaОценок пока нет
- Holy Rosary Academy of Las Piñas City SY 2021-2022: Health Optimizing Physical Education Grade 11Документ20 страницHoly Rosary Academy of Las Piñas City SY 2021-2022: Health Optimizing Physical Education Grade 11Alyson CarandangОценок пока нет
- SdasdasdacxzczxczДокумент3 страницыSdasdasdacxzczxczCaraman MihaitaОценок пока нет
- Investigatory Project BiologyДокумент31 страницаInvestigatory Project BiologyRonaldОценок пока нет
- DME in Saudi Arabia - Myth or FactДокумент25 страницDME in Saudi Arabia - Myth or FactHassan Al-DhibiОценок пока нет
- Primary goal of community health nursing is enhancing capacity to cope with health needsДокумент20 страницPrimary goal of community health nursing is enhancing capacity to cope with health needsKeepItSecretОценок пока нет
- Kis and MegДокумент31 страницаKis and MegkisОценок пока нет
- Bells Palsy FPUK Web PDFДокумент11 страницBells Palsy FPUK Web PDFRadhaKrishnanОценок пока нет
- Karol The Great Plague 15 01 15Документ4 страницыKarol The Great Plague 15 01 15api-276953527Оценок пока нет
- Lapitan NCP MyelomeningoceleДокумент4 страницыLapitan NCP MyelomeningoceleRea LapitanОценок пока нет
- Analisa Jurnal Malnutrition and Its Association With Functional, Cognitive and Psychological Status Among Palestinian Older Adults in Long-Term Care HousesДокумент4 страницыAnalisa Jurnal Malnutrition and Its Association With Functional, Cognitive and Psychological Status Among Palestinian Older Adults in Long-Term Care HousesMila ZaskiaОценок пока нет
- Hepatitis Viral AkutДокумент50 страницHepatitis Viral AkutJonovSelfОценок пока нет
- Immunology Interview Questions - 2022Документ4 страницыImmunology Interview Questions - 2022tadeariba1Оценок пока нет
- Module 4.4 NotesДокумент5 страницModule 4.4 Notesa2a4alensunnyОценок пока нет
- Wk17 Cancers of The BloodДокумент46 страницWk17 Cancers of The BloodPotato PceeОценок пока нет
- ID Pharmacy Content Outline Fall2021Документ5 страницID Pharmacy Content Outline Fall2021Ali MehdiОценок пока нет
- PH Covid Cases, Effects on Economy & DOH ResponseДокумент9 страницPH Covid Cases, Effects on Economy & DOH ResponseJohn CayabyabОценок пока нет
- Njdoh School Exclusion GuidelinesДокумент15 страницNjdoh School Exclusion GuidelinesnurullahfatihОценок пока нет