Вам также может понравиться
- Newman's Billing and Coding Technicians Study GuideОт EverandNewman's Billing and Coding Technicians Study GuideРейтинг: 4.5 из 5 звезд4.5/5 (2)
- Denial Management StepsДокумент42 страницыDenial Management StepsDeepak DpkОценок пока нет
- Billing Training CompleteДокумент141 страницаBilling Training CompleteBOBBILI50% (2)
- AR AnalysisДокумент143 страницыAR AnalysisSai Teja100% (2)
- Medical Billing & Coding Demystified, 2nd EditionОт EverandMedical Billing & Coding Demystified, 2nd EditionРейтинг: 4 из 5 звезд4/5 (1)
- Denial Common ActionДокумент10 страницDenial Common ActionSeenuvasanLeeMani100% (1)
- Code from Home: Launch Your Home-Based Medical Billing ServiceОт EverandCode from Home: Launch Your Home-Based Medical Billing ServiceРейтинг: 5 из 5 звезд5/5 (1)
- Patient Billing & Coding SpecialДокумент44 страницыPatient Billing & Coding SpecialAchiever Kumar100% (3)
- Medical Billing Best Practices Ebook GreenwayДокумент26 страницMedical Billing Best Practices Ebook GreenwayKiran KambleОценок пока нет
- Introduction To The Medical Billing ProcessДокумент34 страницыIntroduction To The Medical Billing ProcessSohailRaja100% (5)
- Basics of Medical Billing & CodingДокумент86 страницBasics of Medical Billing & CodingRic Sánchez100% (3)
- AR Billing Manual - V1212-1Документ14 страницAR Billing Manual - V1212-1spicypoova_899586184100% (1)
- Appeal That ClaimДокумент65 страницAppeal That ClaimParag Shinde100% (2)
- Medical Billing-Simple ManualДокумент17 страницMedical Billing-Simple ManualKarna Palanivelu80% (25)
- Medical Billing TerminologyДокумент49 страницMedical Billing TerminologyBhuvana Bala100% (4)
- Denial Action Training: Welcome To AllДокумент25 страницDenial Action Training: Welcome To Allbraney miller100% (6)
- Medical BillingДокумент229 страницMedical BillingMohammad Apzar100% (6)
- Module 2-Medical Billing Denial AllДокумент70 страницModule 2-Medical Billing Denial AllSaeed ahmed100% (2)
- Medical Billing TrainingДокумент11 страницMedical Billing TrainingHarry Canaba100% (1)
- AR Denials & ActionsДокумент5 страницAR Denials & ActionsAswin Alfred Reddy75% (8)
- Denial - Primary Reason Code DescriptionsДокумент21 страницаDenial - Primary Reason Code Descriptionsfahhad lashari100% (1)
- Medical Billing TermsДокумент15 страницMedical Billing TermsAnonymous YJ3z00Оценок пока нет
- Claims Training Powerpoint1 PDFДокумент54 страницыClaims Training Powerpoint1 PDFshashi madishetty100% (1)
- Coding Denial Tip Sheet - August 3 2021Документ17 страницCoding Denial Tip Sheet - August 3 2021dinesh ram100% (2)
- Denials Claims ExplainationДокумент3 страницыDenials Claims ExplainationNaga RajОценок пока нет
- Medical Billing ProcessДокумент24 страницыMedical Billing ProcessNajamHass100% (5)
- Medical Billing TerminologiesДокумент8 страницMedical Billing Terminologiespriya_psalmsОценок пока нет
- Medical Billing TerminologiesДокумент13 страницMedical Billing TerminologiesSai TejaОценок пока нет
- Medical Billing Process: Naveen MajetyДокумент21 страницаMedical Billing Process: Naveen MajetyNaveen KumarОценок пока нет
- Training Manual (New)Документ16 страницTraining Manual (New)fahhad lashari100% (3)
- ANSI Reason Codes Denial CodesДокумент7 страницANSI Reason Codes Denial CodesShiva ReyesОценок пока нет
- Medical Coding and Compliance NIHДокумент18 страницMedical Coding and Compliance NIHBrandi TadlockОценок пока нет
- Medical Billing Service Marketing PlanДокумент20 страницMedical Billing Service Marketing PlanPalo Alto Software100% (7)
- Reason CodesДокумент12 страницReason CodesNaga RajОценок пока нет
- Coding and Billing BasicsДокумент33 страницыCoding and Billing BasicsGinwong100% (3)
- Beginner S Guide To Medical Billing Coding and Transcription PDFДокумент57 страницBeginner S Guide To Medical Billing Coding and Transcription PDFSuganya BalachandranОценок пока нет
- Rapidcare Medical Billing ManualДокумент93 страницыRapidcare Medical Billing Manualapi-19789919100% (3)
- Medical Coding 101: Boost Your CareerДокумент19 страницMedical Coding 101: Boost Your CareerSupercoder67% (3)
- US Medical Billing CycleДокумент46 страницUS Medical Billing Cycleanon_49916805575% (4)
- Hospital Billing and Coding Process PDFДокумент44 страницыHospital Billing and Coding Process PDFrahul_didoОценок пока нет
- Denial Management White PaperДокумент10 страницDenial Management White PaperPraveen Shenoi100% (1)
- Healthcare Coding Billing Reimbursement OverviewДокумент130 страницHealthcare Coding Billing Reimbursement Overviewsvuhari100% (3)
- ModifiersДокумент8 страницModifiersKarna Palanivelu100% (6)
- Advanced Denial Management TechniquesДокумент41 страницаAdvanced Denial Management TechniquesmairyuОценок пока нет
- Electronic Remittance AdviceДокумент55 страницElectronic Remittance AdviceAbdur RaufОценок пока нет
- Free Medical Coding Course PDFДокумент7 страницFree Medical Coding Course PDFSrinivasa Reddy Reddys75% (4)
- Medical Billing Training: Official Study GuideДокумент16 страницMedical Billing Training: Official Study GuideAbu Salman50% (2)
- Medical BillingДокумент16 страницMedical BillingAbdul Gaffoor100% (5)
- Timely Filing LimitsДокумент3 страницыTimely Filing LimitsShiva ReyesОценок пока нет
- Billing Process ChecklistДокумент2 страницыBilling Process ChecklistSandeep SharmaОценок пока нет
- AR ScenariosДокумент28 страницAR ScenariosBOBBILI100% (1)
- Health Insurance Domain Basics PDFДокумент47 страницHealth Insurance Domain Basics PDFGautam Kumar DwivedyОценок пока нет
- Coding Modifiers TableДокумент22 страницыCoding Modifiers TableArindamDuttaChoudhury100% (1)
- Top 100 Medical Billing and Coding Programs AnnouncedДокумент4 страницыTop 100 Medical Billing and Coding Programs AnnouncedPR.comОценок пока нет
- Medical Coding OrientationДокумент16 страницMedical Coding Orientationdrrskhan100% (1)
- Training MateriaL RCM (Healthcare)Документ66 страницTraining MateriaL RCM (Healthcare)Naveen Babu100% (1)
- Stakeholders in ShippingДокумент4 страницыStakeholders in Shippingnandini_mba4870Оценок пока нет
- Trade Routes and Shipping OverviewДокумент152 страницыTrade Routes and Shipping Overviewnandini_mba4870Оценок пока нет
- Banana CaseДокумент14 страницBanana Casenandini_mba4870Оценок пока нет
- SCM NotesДокумент166 страницSCM Notesnandini_mba4870100% (1)
- Overview of Indian PortsДокумент35 страницOverview of Indian Portsnandini_mba4870Оценок пока нет
- S.No. Name Phone Number E-Mail IdДокумент2 страницыS.No. Name Phone Number E-Mail Idnandini_mba4870Оценок пока нет
- Internship Project - Corporate PresentationДокумент39 страницInternship Project - Corporate Presentationnandini_mba4870Оценок пока нет
- 1st SetДокумент11 страниц1st Setnandini_mba4870Оценок пока нет
- Adidas CasestudyДокумент3 страницыAdidas Casestudynandini_mba4870Оценок пока нет
- Faculty & Coordinator: IIKM Business SchoolДокумент2 страницыFaculty & Coordinator: IIKM Business Schoolnandini_mba4870Оценок пока нет
- Case Study - 1Документ1 страницаCase Study - 1nandini_mba4870Оценок пока нет
- Transaction Processing, Electronic Commerce, and Enterprise Resource Planning SystemsДокумент46 страницTransaction Processing, Electronic Commerce, and Enterprise Resource Planning Systemsnandini_mba4870Оценок пока нет
- Demand Analysis and Law of Demand: Nikhil - 97 Jun-98 Vaidehi-99 Nikita-100 Vishakha-101 Pooja-102Документ15 страницDemand Analysis and Law of Demand: Nikhil - 97 Jun-98 Vaidehi-99 Nikita-100 Vishakha-101 Pooja-102nandini_mba4870Оценок пока нет
- Globalisation & Decline in Public Sector Economy-34Документ13 страницGlobalisation & Decline in Public Sector Economy-34nandini_mba4870Оценок пока нет
- Mis Report - McdonaldsДокумент16 страницMis Report - Mcdonaldsnandini_mba4870100% (3)
- Human Development Index and Quality of Human LifeДокумент7 страницHuman Development Index and Quality of Human Lifenandini_mba4870Оценок пока нет
- Effects of Globalisation On Indian Youth - Sybms A - 31Документ13 страницEffects of Globalisation On Indian Youth - Sybms A - 31nandini_mba4870100% (1)
- Pharma Pricing and ReimbursementДокумент143 страницыPharma Pricing and ReimbursementfatimaОценок пока нет
- IMG Orientation Power Point v1.4Документ102 страницыIMG Orientation Power Point v1.4Jora IonОценок пока нет
- Among The Laws Affecting The Practice of NursingДокумент3 страницыAmong The Laws Affecting The Practice of Nursingmarie100% (35)
- Bridgewater: Global Conditions, Asset Returns and Investment StrategyДокумент341 страницаBridgewater: Global Conditions, Asset Returns and Investment StrategyValueWalk100% (1)
- Modern - Healthcare 21.march.2022Документ66 страницModern - Healthcare 21.march.2022Belu IonОценок пока нет
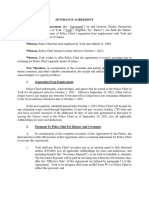
- York Police Chief Separation AgreementДокумент8 страницYork Police Chief Separation AgreementportsmouthheraldОценок пока нет
- Medical Billing Claims Manager in Tampa FL Resume Debra StewartДокумент2 страницыMedical Billing Claims Manager in Tampa FL Resume Debra StewartDebraStewartОценок пока нет
- Primer On Hospital Accounting and Finance, 4th EditionДокумент32 страницыPrimer On Hospital Accounting and Finance, 4th EditionRiyaz Padikkathazha100% (1)
- Rural Hospital Closures Threaten Access ReportДокумент10 страницRural Hospital Closures Threaten Access ReportCourtney RowlesОценок пока нет
- Up 22aug2012Документ4 страницыUp 22aug2012localonОценок пока нет
- Fundamentals 10 Ed Workbook Answer Key PDFДокумент304 страницыFundamentals 10 Ed Workbook Answer Key PDFeric parl88% (108)
- Your Travel Insurance Policy: Reference Number: Insurefor/EA/2009 09IST, 09ISA & 09ISEДокумент12 страницYour Travel Insurance Policy: Reference Number: Insurefor/EA/2009 09IST, 09ISA & 09ISEOmar DahouОценок пока нет
- Philadelphia Resource Directory October 2016Документ70 страницPhiladelphia Resource Directory October 2016Michael ShannonОценок пока нет
- E. Characteristics and Nature of Insurance Contracts - 6 CasesДокумент7 страницE. Characteristics and Nature of Insurance Contracts - 6 CasesJohn Ceasar Ucol ÜОценок пока нет
- Kaushal Vaidya - ProfileДокумент1 страницаKaushal Vaidya - Profilekvaidya100% (1)
- Test Bank For Medical-Surgical Nursing: Concepts & Practice, 2Nd Edition, Susan C. Dewit, Isbn-10: 1437717071, Isbn-13: 9781437717075Документ36 страницTest Bank For Medical-Surgical Nursing: Concepts & Practice, 2Nd Edition, Susan C. Dewit, Isbn-10: 1437717071, Isbn-13: 9781437717075saucisseserratedv8s97100% (22)
- Patient Education Reducing The Costs of Medicines The Basics - UptodateДокумент9 страницPatient Education Reducing The Costs of Medicines The Basics - Uptodateapi-351447133Оценок пока нет
- Wisconsin Senate Debate Transcript 10/18/2012Документ15 страницWisconsin Senate Debate Transcript 10/18/2012adamehirschОценок пока нет
- Johnson & Johnson 10K 2022 PDFДокумент151 страницаJohnson & Johnson 10K 2022 PDFFaisal HusainОценок пока нет
- Parivarthan ModicareДокумент53 страницыParivarthan Modicareisometric_view78% (9)
- Patient Information SheetДокумент1 страницаPatient Information Sheetapi-354525636Оценок пока нет
- Ansi Loop Logic-2010Документ135 страницAnsi Loop Logic-2010YOGESHОценок пока нет
- Medical Symptoms QuestionnaireДокумент29 страницMedical Symptoms QuestionnaireOlesiaОценок пока нет
- Ahm 540Документ5 страницAhm 540Manish Srivastava0% (1)
- Mr. Ajayraj Vyas MR - Ankur Amin: A Project Report ON Insurance Service Under The Guidance ofДокумент36 страницMr. Ajayraj Vyas MR - Ankur Amin: A Project Report ON Insurance Service Under The Guidance ofYogesh PatelОценок пока нет
- W21225760934 0 PDFДокумент2 страницыW21225760934 0 PDFAnonymous czHLQeLPB4Оценок пока нет
- Ghost World 2022-2032Документ60 страницGhost World 2022-2032AquarianОценок пока нет
- Budget Justification Fy2021Документ418 страницBudget Justification Fy2021Lisa FabianОценок пока нет
- Impacts of Pharmaceutical Price Controls On Pricing Sales and MДокумент153 страницыImpacts of Pharmaceutical Price Controls On Pricing Sales and MSnehaPandeyОценок пока нет
- Utah Health Innovation PlanДокумент75 страницUtah Health Innovation PlanState of UtahОценок пока нет
- The 7 Habits of Highly Effective People: The Infographics EditionОт EverandThe 7 Habits of Highly Effective People: The Infographics EditionРейтинг: 4 из 5 звезд4/5 (2475)
- The 5 Second Rule: Transform your Life, Work, and Confidence with Everyday CourageОт EverandThe 5 Second Rule: Transform your Life, Work, and Confidence with Everyday CourageРейтинг: 5 из 5 звезд5/5 (12)
- Summary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearОт EverandSummary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearРейтинг: 4.5 из 5 звезд4.5/5 (560)
- The Compound Effect by Darren Hardy - Book Summary: Jumpstart Your Income, Your Life, Your SuccessОт EverandThe Compound Effect by Darren Hardy - Book Summary: Jumpstart Your Income, Your Life, Your SuccessРейтинг: 5 из 5 звезд5/5 (456)
- No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelОт EverandNo Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelРейтинг: 4.5 из 5 звезд4.5/5 (5)
- The Millionaire Fastlane: Crack the Code to Wealth and Live Rich for a LifetimeОт EverandThe Millionaire Fastlane: Crack the Code to Wealth and Live Rich for a LifetimeРейтинг: 4.5 из 5 звезд4.5/5 (2)
- The One Thing: The Surprisingly Simple Truth Behind Extraordinary ResultsОт EverandThe One Thing: The Surprisingly Simple Truth Behind Extraordinary ResultsРейтинг: 4.5 из 5 звезд4.5/5 (709)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Indistractable: How to Control Your Attention and Choose Your LifeОт EverandIndistractable: How to Control Your Attention and Choose Your LifeРейтинг: 3 из 5 звезд3/5 (5)
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverОт EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverРейтинг: 4.5 из 5 звезд4.5/5 (186)
- The Unbreakable Laws of Self-Confidence: Live Seminar: How to Tap the Infinite Potential WithinОт EverandThe Unbreakable Laws of Self-Confidence: Live Seminar: How to Tap the Infinite Potential WithinРейтинг: 5 из 5 звезд5/5 (112)
- Summary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisОт EverandSummary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (22)
- Eat That Frog!: 21 Great Ways to Stop Procrastinating and Get More Done in Less TimeОт EverandEat That Frog!: 21 Great Ways to Stop Procrastinating and Get More Done in Less TimeРейтинг: 4.5 из 5 звезд4.5/5 (3227)
- Leadership and Self-Deception: Getting out of the BoxОт EverandLeadership and Self-Deception: Getting out of the BoxРейтинг: 5 из 5 звезд5/5 (156)
- Summary: The Gap and the Gain: The High Achievers' Guide to Happiness, Confidence, and Success by Dan Sullivan and Dr. Benjamin Hardy: Key Takeaways, Summary & AnalysisОт EverandSummary: The Gap and the Gain: The High Achievers' Guide to Happiness, Confidence, and Success by Dan Sullivan and Dr. Benjamin Hardy: Key Takeaways, Summary & AnalysisРейтинг: 5 из 5 звезд5/5 (4)
- Quantum Success: 7 Essential Laws for a Thriving, Joyful, and Prosperous Relationship with Work and MoneyОт EverandQuantum Success: 7 Essential Laws for a Thriving, Joyful, and Prosperous Relationship with Work and MoneyРейтинг: 5 из 5 звезд5/5 (38)
- Growth Mindset: 7 Secrets to Destroy Your Fixed Mindset and Tap into Your Psychology of Success with Self Discipline, Emotional Intelligence and Self ConfidenceОт EverandGrowth Mindset: 7 Secrets to Destroy Your Fixed Mindset and Tap into Your Psychology of Success with Self Discipline, Emotional Intelligence and Self ConfidenceРейтинг: 4.5 из 5 звезд4.5/5 (562)
- Fascinate: How to Make Your Brand Impossible to ResistОт EverandFascinate: How to Make Your Brand Impossible to ResistРейтинг: 5 из 5 звезд5/5 (1)
- Mastering Productivity: Everything You Need to Know About Habit FormationОт EverandMastering Productivity: Everything You Need to Know About Habit FormationРейтинг: 4.5 из 5 звезд4.5/5 (23)
- What's Best Next: How the Gospel Transforms the Way You Get Things DoneОт EverandWhat's Best Next: How the Gospel Transforms the Way You Get Things DoneРейтинг: 4.5 из 5 звезд4.5/5 (33)
- Coach Builder: How to Turn Your Expertise Into a Profitable Coaching CareerОт EverandCoach Builder: How to Turn Your Expertise Into a Profitable Coaching CareerРейтинг: 5 из 5 звезд5/5 (2)
- The Happiness Track: How to Apply the Science of Happiness to Accelerate Your SuccessОт EverandThe Happiness Track: How to Apply the Science of Happiness to Accelerate Your SuccessРейтинг: 3.5 из 5 звезд3.5/5 (13)
- Rich Bitch: A Simple 12-Step Plan for Getting Your Financial Life Together . . . FinallyОт EverandRich Bitch: A Simple 12-Step Plan for Getting Your Financial Life Together . . . FinallyРейтинг: 4 из 5 звезд4/5 (8)
- Own Your Past Change Your Future: A Not-So-Complicated Approach to Relationships, Mental Health & WellnessОт EverandOwn Your Past Change Your Future: A Not-So-Complicated Approach to Relationships, Mental Health & WellnessРейтинг: 5 из 5 звезд5/5 (85)