Вам также может понравиться
- PanoramikДокумент38 страницPanoramikStephanie Victoria100% (1)
- Immunohematology & Transfusion Medicine FinalДокумент33 страницыImmunohematology & Transfusion Medicine FinalCollen Mae Silos Diapues100% (1)
- Endo NotesДокумент184 страницыEndo NotesSOMVIR KUMARОценок пока нет
- What Is EBD?Документ7 страницWhat Is EBD?RATHEESH M. S.Оценок пока нет
- Endomishaps SeminarДокумент44 страницыEndomishaps SeminarSuma TettaОценок пока нет
- Practical Pharmacology Review for DentistsДокумент30 страницPractical Pharmacology Review for DentistsalijanmarwatОценок пока нет
- Interpretation of OpgДокумент6 страницInterpretation of Opgjawaad29375% (8)
- Sample Questions MJDF Part 1 Sample Questions MJDF Part 1Документ21 страницаSample Questions MJDF Part 1 Sample Questions MJDF Part 1HarkanОценок пока нет
- Caldwell TechniqueДокумент4 страницыCaldwell TechniqueNurul RamadhantyОценок пока нет
- Dental Digital Photography - Whalen, MackeyДокумент16 страницDental Digital Photography - Whalen, MackeyVijay K PatelОценок пока нет
- Calculate The Max Doses of Local Anesthesia in DentistryДокумент13 страницCalculate The Max Doses of Local Anesthesia in DentistryYasser MagramiОценок пока нет
- Access Cavity Preparation: Dr. Ahmed NegmДокумент55 страницAccess Cavity Preparation: Dr. Ahmed NegmSantika IndahsariОценок пока нет
- Vaccine Handbook Process Br5237en MKДокумент26 страницVaccine Handbook Process Br5237en MKhadeer100% (2)
- Overseas Registration Examination Reading ListДокумент3 страницыOverseas Registration Examination Reading ListyoОценок пока нет
- Basics of Endodontics GuideДокумент26 страницBasics of Endodontics GuideAreebaKhalidОценок пока нет
- Dental Mastery BoardДокумент449 страницDental Mastery BoardFe Rivera100% (1)
- Practice Questions Exam Cram (3rd Edition)Документ1 страницаPractice Questions Exam Cram (3rd Edition)Kiran Kumar0% (3)
- Gingival InflammationДокумент12 страницGingival InflammationdeenmОценок пока нет
- Neet Mds 2021 Recall 161-233 Questions - Meriters StrikesДокумент279 страницNeet Mds 2021 Recall 161-233 Questions - Meriters StrikesAmritha SОценок пока нет
- Study Place Resto Comdent Set5Документ14 страницStudy Place Resto Comdent Set5Zean TrainОценок пока нет
- EsophagusДокумент132 страницыEsophagusBogdan Niculae100% (2)
- MdsДокумент356 страницMdsARJUN SreenivasОценок пока нет
- 3D-CT Evaluation of Facial Asymmetry in Patients With Maxillofacial DeformitiesДокумент9 страниц3D-CT Evaluation of Facial Asymmetry in Patients With Maxillofacial DeformitiesR KОценок пока нет
- 3D Teeth ReconstructionДокумент0 страниц3D Teeth ReconstructionSamir Alberita KeljmendiОценок пока нет
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Journal ClubДокумент2 страницыJournal ClubWaseem AhmedОценок пока нет
- Secondary Space Infection Oral SurgeryДокумент4 страницыSecondary Space Infection Oral SurgeryFourthMolar.comОценок пока нет
- Department of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearДокумент29 страницDepartment of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearFarzana ShereenОценок пока нет
- Oral Tuberculosi S: Dr. Ishita Singhal Mds First YearДокумент31 страницаOral Tuberculosi S: Dr. Ishita Singhal Mds First YearDR. ISHITA SINGHALОценок пока нет
- Luting CementsДокумент13 страницLuting CementsPanah SalahiОценок пока нет
- Mandibular Condylar and Subcondylar Fractures PDFДокумент16 страницMandibular Condylar and Subcondylar Fractures PDFWayan Sutresna YasaОценок пока нет
- Pediatric Dentistry Exam QuestionnaireДокумент2 страницыPediatric Dentistry Exam QuestionnaireVagelis RaftopoulosОценок пока нет
- ClassificationДокумент65 страницClassificationkharachi100% (1)
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarДокумент6 страницEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargОценок пока нет
- Comprehensive Review for Saudi Licence Exam for General DentistДокумент4 страницыComprehensive Review for Saudi Licence Exam for General Dentistzoaib aliОценок пока нет
- Culture Media in Oral PathologyДокумент6 страницCulture Media in Oral Pathologyimi4Оценок пока нет
- Indications For Removal of TeethДокумент27 страницIndications For Removal of TeethMoh'dMAssufiОценок пока нет
- Complete Denture Impression 101Документ3 страницыComplete Denture Impression 101DentalLearningОценок пока нет
- Nbde Part 1 NerveДокумент12 страницNbde Part 1 NerveMrunal DoiphodeОценок пока нет
- Types of Fixed RestorationsДокумент10 страницTypes of Fixed RestorationsRose SkyОценок пока нет
- A Guide To Succeeding in The Df1 Interview (Sample Pages Only)Документ15 страницA Guide To Succeeding in The Df1 Interview (Sample Pages Only)jaipald9067% (3)
- Changing Concepts in Cariology - Forty Years OnДокумент7 страницChanging Concepts in Cariology - Forty Years OnDavid CaminoОценок пока нет
- Imaging in Forensic DentistryДокумент42 страницыImaging in Forensic DentistryAME DENTAL COLLEGE RAICHUR, KARNATAKAОценок пока нет
- Failures in Periodontal Therapy: Review ArticleДокумент6 страницFailures in Periodontal Therapy: Review ArticlezinniaОценок пока нет
- GDC Scope of Practice GuideДокумент11 страницGDC Scope of Practice GuideAlexandra LauraОценок пока нет
- AIIMS Dental PG November 2008 Question PaperДокумент6 страницAIIMS Dental PG November 2008 Question PaperRudra VermaОценок пока нет
- Fellowship in Maxillofacial Trauma: GoalsДокумент6 страницFellowship in Maxillofacial Trauma: GoalsMax FaxОценок пока нет
- Clinical Judgement Protocol 2013 FinalДокумент12 страницClinical Judgement Protocol 2013 FinalSara Faris100% (1)
- Literature GuideДокумент60 страницLiterature Guide12345sagarОценок пока нет
- The Effectiveness of Auxiliary Features On A Tooth Preparation With Inadequate Resistance FormДокумент9 страницThe Effectiveness of Auxiliary Features On A Tooth Preparation With Inadequate Resistance FormJhon Anderson Buendìa GarcìaОценок пока нет
- Comparing Flap Designs for Impacted Tooth RemovalДокумент6 страницComparing Flap Designs for Impacted Tooth RemovalArindam DuttaОценок пока нет
- Iotn Ruler Made EasyДокумент7 страницIotn Ruler Made EasyZahid Ahmad100% (1)
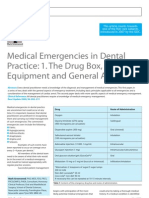
- Medical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachДокумент6 страницMedical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachRodelix San Juan Dacanay100% (1)
- 2015Документ45 страниц2015jimmyОценок пока нет
- ProposalДокумент5 страницProposalapi-354921474Оценок пока нет
- Apical Surgery PDFДокумент7 страницApical Surgery PDFsalman azizОценок пока нет
- Review Peek PDFДокумент11 страницReview Peek PDFAlexandra Dumitrache100% (1)
- Flint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsДокумент20 страницFlint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsNicco Jake AlegroОценок пока нет
- Soffit and PCD PDFДокумент4 страницыSoffit and PCD PDFKalpanaОценок пока нет
- Fixed Orthodontic Appliances: A Practical GuideОт EverandFixed Orthodontic Appliances: A Practical GuideРейтинг: 1 из 5 звезд1/5 (1)
- VitiligoДокумент3 страницыVitiligoAmbar ZenОценок пока нет
- Guidelines Management HSV PregnancyДокумент7 страницGuidelines Management HSV PregnancyAmbar ZenОценок пока нет
- Bagan 2 (1) EritrodermaДокумент1 страницаBagan 2 (1) EritrodermaAmbar ZenОценок пока нет
- Bagan (1) EritrodermaДокумент1 страницаBagan (1) EritrodermaAmbar ZenОценок пока нет
- Algoritm IHC in Mycosis FungoidesДокумент6 страницAlgoritm IHC in Mycosis FungoidesAmbar ZenОценок пока нет
- Immunoparasitology: Blood Parasites Tissue Parasites Intestinal ParasitesДокумент14 страницImmunoparasitology: Blood Parasites Tissue Parasites Intestinal ParasitesCLEMENTОценок пока нет
- ImpetigoДокумент5 страницImpetigoInges PSОценок пока нет
- MATERI HAND HIGYNE DR - AhmadДокумент40 страницMATERI HAND HIGYNE DR - AhmadAhmad Dailah SudrajatОценок пока нет
- Dengue Fever PreventionДокумент3 страницыDengue Fever PreventionjudodododoОценок пока нет
- PREVALENCE OF PULMONARY NONTUBERCULOUS MYCOBACTERIAДокумент6 страницPREVALENCE OF PULMONARY NONTUBERCULOUS MYCOBACTERIAHiroj BagdeОценок пока нет
- Donor Health Check For New and Returning DonorsДокумент1 страницаDonor Health Check For New and Returning DonorsGaoudam NatarajanОценок пока нет
- Body Fluids and Circulation: BloodДокумент1 страницаBody Fluids and Circulation: BloodArpit AggarwalОценок пока нет
- Common ColdДокумент3 страницыCommon ColdshaliniОценок пока нет
- Idiopathic Thrombocytopenic Purpura (ITP) or Immune ThrombocytopeniaДокумент11 страницIdiopathic Thrombocytopenic Purpura (ITP) or Immune ThrombocytopeniaSreekrishnan TrikkurОценок пока нет
- SN4 Question Paper Sum 2006Документ16 страницSN4 Question Paper Sum 2006EmmaОценок пока нет
- Innate and Adaptive Immunity ExplainedДокумент5 страницInnate and Adaptive Immunity ExplainedKebbewar KhaledОценок пока нет
- Hypersensitivity ReactionДокумент8 страницHypersensitivity ReactionSuzetteBragaSamuelaОценок пока нет
- Allergy Self-Assessment QuestionsДокумент63 страницыAllergy Self-Assessment QuestionsavisenicОценок пока нет
- s41586 020 2798 3 - Reference PDFДокумент16 страницs41586 020 2798 3 - Reference PDFYudi AriefОценок пока нет
- Brochure en Ingles OMNILIFE G Y R PDFДокумент4 страницыBrochure en Ingles OMNILIFE G Y R PDFRoxiri Rodríguez MoreraОценок пока нет
- S87 - Sector-12 Sonipat-Cc Shop No 25, Mainmarket Sec-12 (Part-2) Sonipat-131001, Mob No:-09812905359Документ2 страницыS87 - Sector-12 Sonipat-Cc Shop No 25, Mainmarket Sec-12 (Part-2) Sonipat-131001, Mob No:-09812905359Dhruv KuchhalОценок пока нет
- Lecture 1 - Chapter 1 - Introduction To First AidДокумент18 страницLecture 1 - Chapter 1 - Introduction To First AidCatherine Tagorda TiñaОценок пока нет
- Human MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyДокумент34 страницыHuman MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyJános JuhászОценок пока нет
- News ItemДокумент3 страницыNews ItemNovia 'opy' RakhmawatiОценок пока нет
- PMLS 1 Topic 8.3 TransДокумент6 страницPMLS 1 Topic 8.3 TranslalaОценок пока нет
- Standard Services Lab Testing Rapid Antibody, Antigen and RT-PCR TestsДокумент47 страницStandard Services Lab Testing Rapid Antibody, Antigen and RT-PCR TestsMuhamad SetoОценок пока нет
- Ih Lec M9 11Документ27 страницIh Lec M9 11m65b6hf9ffОценок пока нет
- 2018 MTE GIVD Classification 2018 Rev01Документ14 страниц2018 MTE GIVD Classification 2018 Rev01Dr.Sivakumar SelvarajОценок пока нет
- Comm DiseaseДокумент14 страницComm DiseaseApollo WilliamОценок пока нет
- RIAДокумент3 страницыRIAShah SanketОценок пока нет
- Chronic Arthritis in Chikungunya Virus Infection: Lourdes Mateo, Silvia RoureДокумент4 страницыChronic Arthritis in Chikungunya Virus Infection: Lourdes Mateo, Silvia RoureGalileo R. CastroОценок пока нет
- Subject Plan B.SC Nursing 1 Year: MicrobiologyДокумент2 страницыSubject Plan B.SC Nursing 1 Year: MicrobiologySandeep KumarОценок пока нет