Вам также может понравиться
- Lung CancerДокумент96 страницLung Cancersanjivdas100% (4)
- Bronchogenic Carcinoma: Dr. Vineet ChauhanДокумент49 страницBronchogenic Carcinoma: Dr. Vineet ChauhanRaviОценок пока нет
- Understand Cancer & Reduce Cancer Risk - Based On The Teachings Of Dr. Andrew Huberman: Empowering You To Safeguard Against ItОт EverandUnderstand Cancer & Reduce Cancer Risk - Based On The Teachings Of Dr. Andrew Huberman: Empowering You To Safeguard Against ItОценок пока нет
- Lung Cancer: A Guide to Diagnosis and TreatmentОт EverandLung Cancer: A Guide to Diagnosis and TreatmentРейтинг: 5 из 5 звезд5/5 (1)
- Carcinoma of The Breast - Bailey & LoveДокумент5 страницCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Health ResearchДокумент16 страницHealth ResearchTmanoj PraveenОценок пока нет
- Lung Cancer Presentation FinalДокумент48 страницLung Cancer Presentation Finalراس زهد ارفنندОценок пока нет
- Prostate Radiotherapy - Current Standards and Future DirectionsДокумент40 страницProstate Radiotherapy - Current Standards and Future Directionsvikram_bansal84Оценок пока нет
- Bethesda ScoreДокумент7 страницBethesda ScoreTiberiu BircaОценок пока нет
- Thyroid NodulesДокумент34 страницыThyroid NodulesEphobiaОценок пока нет
- Mediastinal MassesДокумент110 страницMediastinal Massesosep77100% (1)
- Adenoid Cystic CarcinomaДокумент7 страницAdenoid Cystic CarcinomalonadiolandaОценок пока нет
- Radiation Therapy 2013Документ59 страницRadiation Therapy 2013AydinОценок пока нет
- 10 Intraoperative RadiotherapyДокумент11 страниц10 Intraoperative RadiotherapyDgek LondonОценок пока нет
- Sentinal Lymph Node BiopsyДокумент12 страницSentinal Lymph Node BiopsySahirОценок пока нет
- Principle of Chemotherapy Main PresentationДокумент84 страницыPrinciple of Chemotherapy Main Presentationadekunle ajayiОценок пока нет
- Trimodality Therapy in Bladder CancerДокумент12 страницTrimodality Therapy in Bladder CancerStirОценок пока нет
- Emetogenicity Tool Kit YaaaДокумент2 страницыEmetogenicity Tool Kit Yaaaandirio7486Оценок пока нет
- Gene Therapy For CancerДокумент7 страницGene Therapy For Canceresraa elsharkawyОценок пока нет
- Forensic Medical Findings in Fatal and Non-Fatal Intimate Partner Strangulation Assaults - Hawley - 2012 PDFДокумент20 страницForensic Medical Findings in Fatal and Non-Fatal Intimate Partner Strangulation Assaults - Hawley - 2012 PDFBoţu AlexandruОценок пока нет
- Gastrointestinal MalignanciesДокумент59 страницGastrointestinal Malignanciesadamu mohammadОценок пока нет
- 2 5 17 991Документ6 страниц2 5 17 991Science JournalОценок пока нет
- Cytotoxic ChemotherapyДокумент33 страницыCytotoxic ChemotherapyDoniTrinandaОценок пока нет
- EAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2Документ145 страницEAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2DellaОценок пока нет
- Benign and Malignant Lesion of Lower GIДокумент45 страницBenign and Malignant Lesion of Lower GIAhmad Alzu3beОценок пока нет
- E Learning Geriatric Oncology An IntroductionДокумент65 страницE Learning Geriatric Oncology An IntroductionHarold JeffersonОценок пока нет
- Major Tropical Diseases - Prof. Dr. Sugeng JuwonoДокумент48 страницMajor Tropical Diseases - Prof. Dr. Sugeng JuwonosittihajarОценок пока нет
- Incisional Hernia RepairДокумент6 страницIncisional Hernia RepairLouis FortunatoОценок пока нет
- Abdominal Organ Transplantation: State of the ArtОт EverandAbdominal Organ Transplantation: State of the ArtNizam MamodeОценок пока нет
- Lung Cancer: By: Faezah Nur Mohd Redzwan Nooratiqah RahmatДокумент30 страницLung Cancer: By: Faezah Nur Mohd Redzwan Nooratiqah RahmatDumora FatmaОценок пока нет
- Small - Intestinal Neoplasms and Carcinoid TumorsДокумент51 страницаSmall - Intestinal Neoplasms and Carcinoid TumorsOlga GoryachevaОценок пока нет
- Colorectal Cancer 1Документ71 страницаColorectal Cancer 1Anupam SisodiaОценок пока нет
- 4 Lung-CancerДокумент72 страницы4 Lung-CancerTaima FayezОценок пока нет
- LeprosyДокумент26 страницLeprosyFamous manОценок пока нет
- WHO MDR 2020 Handbook Treatment PDFДокумент88 страницWHO MDR 2020 Handbook Treatment PDFYuanita GunawanОценок пока нет
- Informed ConsentДокумент25 страницInformed ConsentMaylodie ingallaОценок пока нет
- Pathology of Lung CancerДокумент24 страницыPathology of Lung CancerWeiLinОценок пока нет
- Pathology Short NotesДокумент10 страницPathology Short NotesMr. PhorОценок пока нет
- Cervical Cancer CPGДокумент88 страницCervical Cancer CPGkhai xian100% (1)
- Intraoperative Irradiation Techniques and ResultsДокумент533 страницыIntraoperative Irradiation Techniques and ResultsTELLY GONZALO ROMERO BRIOSOОценок пока нет
- Viva Questions AllДокумент18 страницViva Questions AllFiaz medicoОценок пока нет
- Necrosis and Apoptosis Short Notes For PathologyДокумент3 страницыNecrosis and Apoptosis Short Notes For PathologyAlias AliquidОценок пока нет
- Spinal TuberculosisДокумент46 страницSpinal TuberculosisAbby Austero100% (1)
- Oncology Questions by DR - OkashaДокумент31 страницаOncology Questions by DR - Okashamohammed okashaОценок пока нет
- Chemotherapeutic DrugsДокумент4 страницыChemotherapeutic DrugsEditor IJTSRDОценок пока нет
- NemaoДокумент94 страницыNemaoRoxenette Gil Bernales PangilinanОценок пока нет
- Lecture 3 - The Cell and Reaction To Injury - 2 Sep 2006Документ19 страницLecture 3 - The Cell and Reaction To Injury - 2 Sep 2006api-3703352Оценок пока нет
- ILRT Dr. Sarbani-1 PDFДокумент48 страницILRT Dr. Sarbani-1 PDFdurgesh kumar100% (1)
- Epid COPDДокумент9 страницEpid COPDAgung WistaraОценок пока нет
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaДокумент63 страницыCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireОценок пока нет
- Breast Self ExaminationДокумент81 страницаBreast Self ExaminationAudrie Allyson Gabales100% (1)
- Oncology-Study of Cancer Cellular AbberationДокумент43 страницыOncology-Study of Cancer Cellular AbberationIrwan M. IskoberОценок пока нет
- MS SurgeryДокумент118 страницMS SurgeryLove wattaОценок пока нет
- Radiotherapy in Gynaecological MalignancyДокумент107 страницRadiotherapy in Gynaecological Malignancyneha100% (1)
- Phyllodes Tumors of The Breast UpToDateДокумент22 страницыPhyllodes Tumors of The Breast UpToDateSean SialanaОценок пока нет
- National Tuberculosis ProgramДокумент37 страницNational Tuberculosis ProgramDon Oliveros ÜОценок пока нет
- Endocarditis, Pericarditic, Myocarditis: TopicДокумент104 страницыEndocarditis, Pericarditic, Myocarditis: TopicOM VERMAОценок пока нет
- NCCN Guideline RC v3 2022Документ20 страницNCCN Guideline RC v3 2022dony hendrawanОценок пока нет
- Prostate Cancer AwarenessДокумент10 страницProstate Cancer AwarenessarthurmathieuОценок пока нет
- Cover LetterДокумент1 страницаCover Lettermiaaudina72Оценок пока нет
- Leaflet WahamДокумент2 страницыLeaflet Wahammiaaudina72Оценок пока нет
- Role Play English Language Pediatric Nursing of DHF DiseaseДокумент1 страницаRole Play English Language Pediatric Nursing of DHF Diseasemiaaudina72Оценок пока нет
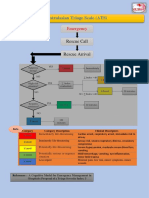
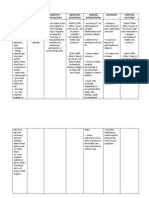
- Australasian Triage Scale (ATS) : EmergencyДокумент2 страницыAustralasian Triage Scale (ATS) : Emergencymiaaudina72Оценок пока нет
- Algoritma CKD PDFДокумент2 страницыAlgoritma CKD PDFDesla Citra100% (1)
- Aramark Book FinalДокумент29 страницAramark Book FinalRavinder NehraОценок пока нет
- NCPДокумент12 страницNCPJonathan Liscano100% (3)
- Steward Score Children AnestheticДокумент3 страницыSteward Score Children AnestheticJuli SatriaОценок пока нет
- Tuberculosis of KneeДокумент17 страницTuberculosis of KneeJithin Bhagavati KalamОценок пока нет
- Lactational Mastitis Puerperal 2020Документ12 страницLactational Mastitis Puerperal 2020bgОценок пока нет
- Sanuvox Case StudiesДокумент4 страницыSanuvox Case StudiesMohd Khairunie IhsanОценок пока нет
- Clonazepam Drug CardДокумент1 страницаClonazepam Drug CardSheri490Оценок пока нет
- Pathology MCQsДокумент10 страницPathology MCQsAnuradha Nanayakkara0% (2)
- Hallucinations, Delusions and Paranoia: See The DoctorДокумент3 страницыHallucinations, Delusions and Paranoia: See The DoctorNyong FenОценок пока нет
- AsthmaДокумент57 страницAsthmaVladanОценок пока нет
- SECOND YEAR PHARMD Syllabus PU PDFДокумент14 страницSECOND YEAR PHARMD Syllabus PU PDFRIYA ROYОценок пока нет
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaДокумент106 страницDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12Оценок пока нет
- Utah Medical Cannabis Act OverviewДокумент10 страницUtah Medical Cannabis Act OverviewThe Salt Lake Tribune100% (1)
- Adime For DiabetesДокумент2 страницыAdime For Diabetesapi-383891195Оценок пока нет
- Keshe - Nano and Gans Health Apps 3of4 29ppДокумент29 страницKeshe - Nano and Gans Health Apps 3of4 29ppExopolitika MagyarországОценок пока нет
- AXA-Self Declaration FormДокумент1 страницаAXA-Self Declaration FormtanishqОценок пока нет
- MAPEH 9 TOS 1st GradingДокумент4 страницыMAPEH 9 TOS 1st Gradingelyn50% (2)
- Chapter 22 Nursing Management of The Postpartum Woman at RiskДокумент18 страницChapter 22 Nursing Management of The Postpartum Woman at RiskSusanna ConigliaroОценок пока нет
- Flu Vaccine: Information For People at RiskДокумент8 страницFlu Vaccine: Information For People at Riskkovi mОценок пока нет
- LBM 4 HerbalДокумент24 страницыLBM 4 HerbalQonitina HafidhaОценок пока нет
- NCP For Imbalanced NutritionДокумент6 страницNCP For Imbalanced NutritionMelvin MartinezОценок пока нет
- High Risk Pregnancy HB TranxДокумент11 страницHigh Risk Pregnancy HB TranxangeliquepastranaОценок пока нет
- Similarities and Differences VocabularyДокумент9 страницSimilarities and Differences VocabularyAliОценок пока нет
- The NysseДокумент208 страницThe NysseSiti Nur JariyahОценок пока нет
- Trigger FingerДокумент1 страницаTrigger FingerWisniardhy Suarnata PradanaОценок пока нет
- Kode Diagnosa BpjsДокумент12 страницKode Diagnosa BpjsHariono KalamОценок пока нет
- Emergency Department Chest Pain Evaluation PathwayДокумент2 страницыEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidОценок пока нет
- Combank NotesДокумент7 страницCombank NotesVee MendОценок пока нет
- Ramadan and Diabetes MCB DiabetesUK LeafletДокумент4 страницыRamadan and Diabetes MCB DiabetesUK LeafletChris MulyoОценок пока нет