Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- n695 Resume For PortfolioДокумент1 страницаn695 Resume For Portfolioapi-415514156Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- n393 SimulationДокумент5 страницn393 Simulationapi-415514156Оценок пока нет
- n640 w8 SequencingДокумент7 страницn640 w8 Sequencingapi-415514156Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- n610 Leading Change PaperДокумент13 страницn610 Leading Change Paperapi-415514156Оценок пока нет
- Running Head: PRENATAL CARE 1Документ13 страницRunning Head: PRENATAL CARE 1api-415514156Оценок пока нет
- Attention Deficit Hyperactivity Disorder: Molly Gleason RN, BSN N530 Advanced PharmacotherapeuticsДокумент44 страницыAttention Deficit Hyperactivity Disorder: Molly Gleason RN, BSN N530 Advanced Pharmacotherapeuticsapi-415514156Оценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Climate Change, What Is It - Understanding The Basic Facts About Global WarmingДокумент23 страницыClimate Change, What Is It - Understanding The Basic Facts About Global WarmingFer OssОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- VtM2nded1 Page PDFДокумент1 страницаVtM2nded1 Page PDFJoseph CortesОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- P.E & Health G11-Q1-M7Документ13 страницP.E & Health G11-Q1-M7John Gerald CantancioОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Fatimah Kti FixДокумент71 страницаFatimah Kti FixOktaviani MuhaddistОценок пока нет
- Aldridge A Short Introduction To CounsellingДокумент22 страницыAldridge A Short Introduction To Counsellingbyron chieОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Slu Brochure Ay 2014-2015Документ2 страницыSlu Brochure Ay 2014-2015Michael BermudoОценок пока нет
- American Soc. of Addiction Medicine Naloxone StatementДокумент5 страницAmerican Soc. of Addiction Medicine Naloxone Statementwebmaster@drugpolicy.orgОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Freedom From DistractibilityДокумент4 страницыFreedom From DistractibilityΚων/να ΠαπОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- MDWF 1030 Carter Plugged Duct Mastitis Abscess PGДокумент5 страницMDWF 1030 Carter Plugged Duct Mastitis Abscess PGapi-366292665Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- ObamaDeception SupplementalBookletДокумент34 страницыObamaDeception SupplementalBookletAccurateHistorian100% (4)
- Tonometry and Care of Tonometers PDFДокумент7 страницTonometry and Care of Tonometers PDFAnni MuharomahОценок пока нет
- Your Wellness Profile: Laboratory ActivitiesДокумент4 страницыYour Wellness Profile: Laboratory Activitiesdusty kawiОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Guide To Safety Committee Meeting Tech3Документ5 страницA Guide To Safety Committee Meeting Tech3vsrslm100% (1)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Cummins Prem Blue 15w40 1-18 L Sing Ssv3028m18 Asia-Pacific Purple Book (GHS) - EnglishДокумент14 страницCummins Prem Blue 15w40 1-18 L Sing Ssv3028m18 Asia-Pacific Purple Book (GHS) - EnglishjosephvanbacОценок пока нет
- Stress Management Stress Management: NptelДокумент99 страницStress Management Stress Management: NptelDKОценок пока нет
- Town Planning: Q. Identify The Problems in India Regarding Town PlanningДокумент8 страницTown Planning: Q. Identify The Problems in India Regarding Town PlanningYogesh BhardwajОценок пока нет
- Surgery Alasdair ScottДокумент160 страницSurgery Alasdair ScottDanny SchОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Presented By: 1) S.Chandra Prakash 2) Rohith Sirpa Iii B.Tech Bme, BvritДокумент21 страницаPresented By: 1) S.Chandra Prakash 2) Rohith Sirpa Iii B.Tech Bme, BvritBiplav EvolvesОценок пока нет
- 2016 Article InternationalEcoHealthOneHealtДокумент139 страниц2016 Article InternationalEcoHealthOneHealtMauricio FemeníaОценок пока нет
- Otto Gross A Case of Exclusion and Oblivion in TheДокумент13 страницOtto Gross A Case of Exclusion and Oblivion in TheVissente TapiaОценок пока нет
- Nursing Care Plan: Her Last Menstrual Period Was May 28 of The Year WithДокумент2 страницыNursing Care Plan: Her Last Menstrual Period Was May 28 of The Year WithMiguel VismonteОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Fundamentals of Nursing - Nurse As ProfessionДокумент7 страницFundamentals of Nursing - Nurse As ProfessionDarryl C. LocañasОценок пока нет
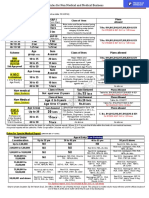
- Rules For Non Medical BusinessДокумент1 страницаRules For Non Medical BusinessAbhijit AminpurОценок пока нет
- PI - Standard - Seafood Processing - Issue 5.0 - 1-February-2019Документ65 страницPI - Standard - Seafood Processing - Issue 5.0 - 1-February-2019pebru yuwono0% (1)
- N Vent Code ENДокумент28 страницN Vent Code ENGwenn LecturaОценок пока нет
- Bayley Scales of Infant Development IIДокумент2 страницыBayley Scales of Infant Development IIbutterflybaby04Оценок пока нет
- Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId p1s0K7qAzHwmL8S2z98THgДокумент3 страницыTdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId p1s0K7qAzHwmL8S2z98THgyesawovОценок пока нет
- 10Документ19 страниц10Bruno100% (3)
- Outpatient Asthma Management Without Rescue BronchodilatorsДокумент4 страницыOutpatient Asthma Management Without Rescue BronchodilatorsHerald Scholarly Open AccessОценок пока нет
- Sinif Ingilizce 8. Unite Calisma Kagidi Test Etkinlik Worksheet FITNESS by Murat DukkanciДокумент13 страницSinif Ingilizce 8. Unite Calisma Kagidi Test Etkinlik Worksheet FITNESS by Murat DukkanciElif yurtsevenОценок пока нет