Вам также может понравиться
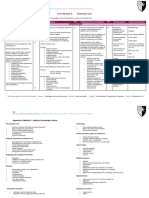
- Chapter 6 Strategy Analysis and Choice: Strategic Management: A Competitive Advantage Approach, 16e (David)Документ27 страницChapter 6 Strategy Analysis and Choice: Strategic Management: A Competitive Advantage Approach, 16e (David)Masum ZamanОценок пока нет
- Cummins: ISX15 CM2250Документ17 страницCummins: ISX15 CM2250haroun100% (4)
- Gracella Irwana - G - Pert 04 - Sia - 1Документ35 страницGracella Irwana - G - Pert 04 - Sia - 1Gracella IrwanaОценок пока нет
- Incontinencia UrinariaДокумент4 страницыIncontinencia Urinariavillo123456Оценок пока нет
- Endoanal Ultrasound Findings and Fecal.10Документ8 страницEndoanal Ultrasound Findings and Fecal.10Ria Veronica N. Carino-VictoriaОценок пока нет
- Obstetric Practice and The Prevalence Urinary Incontinence Three Months After DeliveryДокумент8 страницObstetric Practice and The Prevalence Urinary Incontinence Three Months After DeliveryBharata YudhaОценок пока нет
- Journal Obgyne DR - ApДокумент6 страницJournal Obgyne DR - Apoktaviana54Оценок пока нет
- International Journal of Gynecology and Obstetrics: Adolf Lukanovi Č, Katarina Dra ŽičДокумент4 страницыInternational Journal of Gynecology and Obstetrics: Adolf Lukanovi Č, Katarina Dra ŽičkevindjuandaОценок пока нет
- W H D S D P F ?: Hat Arm Oes A Econd Elivery To The Elvic LoorДокумент5 страницW H D S D P F ?: Hat Arm Oes A Econd Elivery To The Elvic LoorRadis Virna Da GustaОценок пока нет
- Singleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalДокумент6 страницSingleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalSarah SilaenОценок пока нет
- Anal Sphincter Tears at Vaginal Delivery Risk.5Документ8 страницAnal Sphincter Tears at Vaginal Delivery Risk.5Melian AnitaОценок пока нет
- Risk Factors Associated With Fetal Pleural Effusion in Prenatal Diagnosis: A Retrospective Study in A Single Institute in Southern ChinaДокумент6 страницRisk Factors Associated With Fetal Pleural Effusion in Prenatal Diagnosis: A Retrospective Study in A Single Institute in Southern Chinachristian roblesОценок пока нет
- Rupture of Tubal Pregnancy in The Vilnius Population: Pasquale Berlingieri, Grazina Bogdanskiene, Jurgis G. GrudzinskasДокумент4 страницыRupture of Tubal Pregnancy in The Vilnius Population: Pasquale Berlingieri, Grazina Bogdanskiene, Jurgis G. Grudzinskaslilis lestariОценок пока нет
- Evaluation of Transvaginal Sonography in Detecting Endometrial Polyps and The Pregnancy Outcome Following Hysteroscopic Polypectomy in Infertile WomenДокумент5 страницEvaluation of Transvaginal Sonography in Detecting Endometrial Polyps and The Pregnancy Outcome Following Hysteroscopic Polypectomy in Infertile WomenMoe AboamОценок пока нет
- Cases With Ruptured Membranes That "Reseal": Gainesville, FloridaДокумент7 страницCases With Ruptured Membranes That "Reseal": Gainesville, FloridaHòa HồОценок пока нет
- Can Ultrasonography or Uroflowmetry Predict Which Children With Voiding Dysfunction Will Have Recurrent Urinary Tract Infections?Документ3 страницыCan Ultrasonography or Uroflowmetry Predict Which Children With Voiding Dysfunction Will Have Recurrent Urinary Tract Infections?graciaОценок пока нет
- Seijmonsbergenschermers 2013Документ9 страницSeijmonsbergenschermers 2013Febyan AbotОценок пока нет
- European Journal of Obstetrics & Gynecology and Reproductive BiologyДокумент3 страницыEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyRaissa Metasari TantoОценок пока нет
- Endometriosis EurДокумент5 страницEndometriosis EurReynaldi AbdullahОценок пока нет
- Bladder Calculus Resulting From The Migration of An IntrauterineДокумент8 страницBladder Calculus Resulting From The Migration of An IntrauterineFabrien Hein WillemОценок пока нет
- Jurnal Rupture Perineum 1Документ11 страницJurnal Rupture Perineum 1Muh AqwilОценок пока нет
- Routine Episiotomy For Vaginal Birth: Should It Be Ignored?Документ8 страницRoutine Episiotomy For Vaginal Birth: Should It Be Ignored?IOSRjournalОценок пока нет
- Postpartum Urinary Retention After Vaginal Delivery: Research ArticleДокумент5 страницPostpartum Urinary Retention After Vaginal Delivery: Research ArticleZiafadeОценок пока нет
- Detection of Chromosome Aberrations in TheДокумент3 страницыDetection of Chromosome Aberrations in TheSonia Delgado EspinozaОценок пока нет
- Hard Arson 2008Документ7 страницHard Arson 2008elda zulkarnainОценок пока нет
- Art 20177509Документ4 страницыArt 20177509Jashashree SaikiaОценок пока нет
- Uterine ProlapseДокумент6 страницUterine ProlapseIndah Rizki Haksapani Nasution100% (1)
- Journal Pre-Proof: Journal of Pediatric and Adolescent GynecologyДокумент18 страницJournal Pre-Proof: Journal of Pediatric and Adolescent GynecologyCorey WoodsОценок пока нет
- 1911-Article Text-3239-1-10-20181114Документ5 страниц1911-Article Text-3239-1-10-20181114drumerОценок пока нет
- Long-Term Risks of Stress and Urgency Urinary Incontinence After Different Vaginal Delivery ModesДокумент8 страницLong-Term Risks of Stress and Urgency Urinary Incontinence After Different Vaginal Delivery Modespalomachagas1986Оценок пока нет
- Spectrum of Normal Intrauterine Cavity Sonographic Findings After First-Trimester AbortionДокумент5 страницSpectrum of Normal Intrauterine Cavity Sonographic Findings After First-Trimester AbortionOrchid LandОценок пока нет
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Документ21 страницаGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguОценок пока нет
- Seminar: J Eric Jelovsek, Christopher Maher, Matthew D BarberДокумент12 страницSeminar: J Eric Jelovsek, Christopher Maher, Matthew D BarberViesna Beby AulianaОценок пока нет
- Jurnal Bhs. Inggris Obgyn 1Документ7 страницJurnal Bhs. Inggris Obgyn 1RiLa Dwi KurniatiОценок пока нет
- Myomas and Assisted Reproductive Technologies: When and How To Act?Документ8 страницMyomas and Assisted Reproductive Technologies: When and How To Act?Marco Julcamoro AsencioОценок пока нет
- Association of Voiding Dysfunction With Functional ConstipationДокумент3 страницыAssociation of Voiding Dysfunction With Functional ConstipationSisca Dwi AgustinaОценок пока нет
- Transvaginal Ultrasound Findings Among The Women Presenting With InfertilityДокумент4 страницыTransvaginal Ultrasound Findings Among The Women Presenting With InfertilityLajja Parikh PatelОценок пока нет
- Episio PDFДокумент4 страницыEpisio PDFEduBarranzuelaОценок пока нет
- Ijph 41 92Документ7 страницIjph 41 92Trung Kien VoОценок пока нет
- Ovarian Endometriomas and IVF: A Retrospective Case-Control StudyДокумент6 страницOvarian Endometriomas and IVF: A Retrospective Case-Control Studydr.pravitasari23Оценок пока нет
- An Analysis of Uterine Rupture at The Nnamdi AzikiweДокумент5 страницAn Analysis of Uterine Rupture at The Nnamdi AzikiweNublah Permata LestariОценок пока нет
- Risk Factors For Uterine Fibroids Among Women Undergoing Tubal SterilizationДокумент8 страницRisk Factors For Uterine Fibroids Among Women Undergoing Tubal SterilizationWahyu Tri KusprasetyoОценок пока нет
- Evidence-Based Management of Endometrioma: Tarek A Gelbaya, Luciano G NardoДокумент10 страницEvidence-Based Management of Endometrioma: Tarek A Gelbaya, Luciano G NardofebrianoramadhanaОценок пока нет
- Management and Outcome of Testicular Torsion: Background ConclusionДокумент4 страницыManagement and Outcome of Testicular Torsion: Background Conclusionabdullahi husseinОценок пока нет
- Application of Ultrasonography in Female Infertility: A Comprehensive ReviewДокумент11 страницApplication of Ultrasonography in Female Infertility: A Comprehensive ReviewNur Fitryanti Lubis100% (1)
- JejeuryДокумент5 страницJejeuryRizka YusraОценок пока нет
- Risk Factors For Inguinal Hernia in Women: A Case-Control StudyДокумент6 страницRisk Factors For Inguinal Hernia in Women: A Case-Control StudyAl-Harits OctaОценок пока нет
- Endometriosis and Human Infertility: A New Investigation Into The Role of Eutopic EndometriumДокумент8 страницEndometriosis and Human Infertility: A New Investigation Into The Role of Eutopic Endometrium12ock312Оценок пока нет
- Amenore PrimerДокумент4 страницыAmenore PrimerHamka KoersloОценок пока нет
- Jurnal Rupture Perineum 2Документ9 страницJurnal Rupture Perineum 2Muh AqwilОценок пока нет
- Genital Tract Fistulae in The Republic of Yemen, Sana'a - SciAlert Responsive VersionДокумент11 страницGenital Tract Fistulae in The Republic of Yemen, Sana'a - SciAlert Responsive VersionAli AlyousfeОценок пока нет
- Transabdominal Sonography Before Uterine Exploration As A Predictor of Retained Placental FragmentsДокумент5 страницTransabdominal Sonography Before Uterine Exploration As A Predictor of Retained Placental FragmentsDownloadОценок пока нет
- Relationship Between Ovarian Cyst and InfertilityДокумент7 страницRelationship Between Ovarian Cyst and InfertilityiVriskОценок пока нет
- WHO Systematic Review of Maternal Mortality and Morbidity: The Prevalence of Uterine RuptureДокумент8 страницWHO Systematic Review of Maternal Mortality and Morbidity: The Prevalence of Uterine RuptureThomas TombusОценок пока нет
- Selective Vs Routine Midline Episiotomy For The PRДокумент4 страницыSelective Vs Routine Midline Episiotomy For The PRIriawan Indra PutraОценок пока нет
- J Ajog 2019 05 022Документ17 страницJ Ajog 2019 05 022DWI LESTARIОценок пока нет
- Risk Factors For Ectopic Pregnancy in Women With Planned PregnancyДокумент7 страницRisk Factors For Ectopic Pregnancy in Women With Planned PregnancydnnivОценок пока нет
- Comparation Between Levator Ani Avulsion and Size of Genital Hiatus-Perineal Body Complex On Spontaneus DeliveryДокумент10 страницComparation Between Levator Ani Avulsion and Size of Genital Hiatus-Perineal Body Complex On Spontaneus DeliveryDeden Lukman HakimОценок пока нет
- Farman Bhai TreatmentДокумент4 страницыFarman Bhai TreatmentDr-Noor Muhammad KhanОценок пока нет
- Park 2001Документ4 страницыPark 2001witriОценок пока нет
- The Strategy For Vaginal Rejuvenation CO2 Laser or VaginoplastyДокумент7 страницThe Strategy For Vaginal Rejuvenation CO2 Laser or VaginoplastyАркадий ЖивицаОценок пока нет
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentОт EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentОценок пока нет
- Table of Content AsthmaДокумент1 страницаTable of Content AsthmaRizka YusraОценок пока нет
- Table of Content AsthmaДокумент1 страницаTable of Content AsthmaRizka YusraОценок пока нет
- Core Module 8: Antenatal Care: Learning OutcomesДокумент8 страницCore Module 8: Antenatal Care: Learning OutcomesRizka YusraОценок пока нет
- Daftar pustaka-OKДокумент12 страницDaftar pustaka-OKRizka YusraОценок пока нет
- Inkontinensia Urin Pascapersalinan Dan Faktor-Faktor Risiko Yang MemengaruhinyaДокумент8 страницInkontinensia Urin Pascapersalinan Dan Faktor-Faktor Risiko Yang MemengaruhinyaRizka YusraОценок пока нет
- JejeuryДокумент5 страницJejeuryRizka YusraОценок пока нет
- Distosia BahuДокумент25 страницDistosia BahuDini IrianiОценок пока нет
- Asphyxia, Neurologic Morbidity, and Perinatal Mortality in Early-Term and Postterm BirthДокумент11 страницAsphyxia, Neurologic Morbidity, and Perinatal Mortality in Early-Term and Postterm BirthRizka YusraОценок пока нет
- Antenatal Care (ANC)Документ77 страницAntenatal Care (ANC)tareОценок пока нет
- Maskote WB Zinc Stop-OffДокумент7 страницMaskote WB Zinc Stop-OffbondsivamaniОценок пока нет
- DIY Toolkit Arabic Web VersionДокумент168 страницDIY Toolkit Arabic Web VersionAyda AlshamsiОценок пока нет
- Behavior Intervention MenuДокумент56 страницBehavior Intervention Menuapi-479527084100% (4)
- DADTCO Presentation PDFДокумент34 страницыDADTCO Presentation PDFIngeniería Industrias Alimentarias Itsm100% (1)
- 2017LR72 - SUMMARY REPORT Final 03052020Документ72 страницы2017LR72 - SUMMARY REPORT Final 03052020Dung PhamОценок пока нет
- 00022443the Application of A Continuous Leak Detection System To Pipelines and Associated EquipmentДокумент4 страницы00022443the Application of A Continuous Leak Detection System To Pipelines and Associated EquipmentFaizal AbdullahОценок пока нет
- Class InsectaДокумент4 страницыClass InsectaLittle Miss CeeОценок пока нет
- Essay On Stem CellsДокумент4 страницыEssay On Stem CellsAdrien G. S. WaldОценок пока нет
- Dragons ScaleДокумент13 страницDragons ScaleGuilherme De FariasОценок пока нет
- Simple Enzymes Kinetics and Kinetics ModelДокумент14 страницSimple Enzymes Kinetics and Kinetics ModelSidra-tul MuntahaОценок пока нет
- MSDS Leadframe (16 Items)Документ8 страницMSDS Leadframe (16 Items)bennisg8Оценок пока нет
- All Nobel Prizes in LiteratureДокумент16 страницAll Nobel Prizes in LiteratureMohsin IftikharОценок пока нет
- Chain: SRB Series (With Insulation Grip)Документ1 страницаChain: SRB Series (With Insulation Grip)shankarОценок пока нет
- 2nd Second Sun of Advent (B)Документ4 страницы2nd Second Sun of Advent (B)Max PolakОценок пока нет
- VERGARA - RPH Reflection PaperДокумент2 страницыVERGARA - RPH Reflection PaperNezer Byl P. VergaraОценок пока нет
- Zillah P. Curato: ObjectiveДокумент1 страницаZillah P. Curato: ObjectiveZillah CuratoОценок пока нет
- Te-Chemical Sem5 CPNM-CBCGS Dec19Документ2 страницыTe-Chemical Sem5 CPNM-CBCGS Dec19Mayank ShelarОценок пока нет
- Arc Hydro - Identifying and Managing SinksДокумент35 страницArc Hydro - Identifying and Managing SinkskbalОценок пока нет
- Chapter 9Документ28 страницChapter 9Aniket BatraОценок пока нет
- Big Brother Naija and Its Impact On Nigeria University Students 2 PDFДокумент30 страницBig Brother Naija and Its Impact On Nigeria University Students 2 PDFIlufoye Tunde100% (1)
- Gold Loan Application FormДокумент7 страницGold Loan Application FormMahesh PittalaОценок пока нет
- Circuit Construction: Assignment 3Документ45 страницCircuit Construction: Assignment 3ali morisyОценок пока нет
- Kingroon ConfiguracoesДокумент3 страницыKingroon ConfiguracoesanafrancaОценок пока нет
- Embedded Software Development ProcessДокумент34 страницыEmbedded Software Development ProcessAmmar YounasОценок пока нет
- Book Chapter 11 SubmissionДокумент18 страницBook Chapter 11 Submissioncristine_2006_g5590Оценок пока нет
- Brochure - OasisДокумент24 страницыBrochure - OasisVivek RОценок пока нет