Вам также может понравиться
- Native Data Sheet Asme b73.1Документ4 страницыNative Data Sheet Asme b73.1Akhmad Faruq Alhikami100% (1)
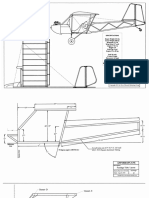
- Plans PDFДокумент49 страницPlans PDFEstevam Gomes de Azevedo85% (34)
- Sample Mixed Method ResearchДокумент106 страницSample Mixed Method ResearchchristophermaqОценок пока нет
- If T Sensory Science Part I IДокумент21 страницаIf T Sensory Science Part I Ifatehatun noorОценок пока нет
- Savitz David A. Wellenius Gregory A - Interpreting Epidemiologic Evidence Connecting Research To AДокумент241 страницаSavitz David A. Wellenius Gregory A - Interpreting Epidemiologic Evidence Connecting Research To ATurjya LaskarОценок пока нет
- 2018 ESMO Handbook of Interpreting Oncological Study PublicationsДокумент219 страниц2018 ESMO Handbook of Interpreting Oncological Study PublicationsAlex Lugli100% (1)
- BMC Psychiatry: An Animated Depiction of Major Depression EpidemiologyДокумент6 страницBMC Psychiatry: An Animated Depiction of Major Depression Epidemiologyklysmanu93Оценок пока нет
- Research Methods in Human DevelopmentДокумент408 страницResearch Methods in Human DevelopmentElvie KalawОценок пока нет
- Biophoton RevolutionДокумент3 страницыBiophoton RevolutionVyavasayaha Anita BusicОценок пока нет
- Naming Hydrocarbons Worksheet1 Key 12 26 08 PDFДокумент2 страницыNaming Hydrocarbons Worksheet1 Key 12 26 08 PDFMarilyn Castro Laquindanum100% (1)
- Epidemiology in EmergenciesДокумент18 страницEpidemiology in EmergenciessmartisaacОценок пока нет
- Francesca Filbey - The Neuroscience of Addiction-Cambridge University Press (2019) PDFДокумент208 страницFrancesca Filbey - The Neuroscience of Addiction-Cambridge University Press (2019) PDFBrujoucm100% (1)
- Healty Foods in WorldДокумент2 страницыHealty Foods in Worldsathishsep18Оценок пока нет
- (Strategies For Social Inquiry) John Gerring - Case Study Research - Principles and Practices-Cambridge University Press (2017)Документ359 страниц(Strategies For Social Inquiry) John Gerring - Case Study Research - Principles and Practices-Cambridge University Press (2017)Viviana HurtadoОценок пока нет
- JC Series Jaw Crusher PDFДокумент8 страницJC Series Jaw Crusher PDFgarrybieber100% (1)
- Brian L Strom Stephen e Kimmel Sean Hennessy Textbook 2021Документ557 страницBrian L Strom Stephen e Kimmel Sean Hennessy Textbook 2021Oscar DawsonОценок пока нет
- Coconut OilДокумент2 страницыCoconut Oildimo100% (1)
- (Martyn Denscombe) The Good Research GuideДокумент389 страниц(Martyn Denscombe) The Good Research GuideAris Yunandar100% (4)
- Teacher-Made Instructional Material MODULE IN PSY196/Field Methods in PsychologyДокумент74 страницыTeacher-Made Instructional Material MODULE IN PSY196/Field Methods in PsychologyMa. Nenita L. MagallanesОценок пока нет
- EpidemiologyДокумент89 страницEpidemiologyKrishnaveni MurugeshОценок пока нет
- Immy Holloway - Qualitative Research in Health Care-Open University Press (2005)Документ320 страницImmy Holloway - Qualitative Research in Health Care-Open University Press (2005)mohammedОценок пока нет
- Level of Prevention FinalДокумент27 страницLevel of Prevention FinalRakersh PatidarОценок пока нет
- ملف الوبائيات بعد التعديلДокумент3 страницыملف الوبائيات بعد التعديلMustafa KhudhairОценок пока нет
- EpiCross SectionalstudyДокумент10 страницEpiCross Sectionalstudyapi-3858544Оценок пока нет
- EpidemiologyДокумент1 страницаEpidemiologySandeep KumarОценок пока нет
- Virgin Coconut OilДокумент3 страницыVirgin Coconut OilEd CasasОценок пока нет
- Epidemiology: Transmission of The Dengue VirusДокумент4 страницыEpidemiology: Transmission of The Dengue Viruschiquilon749Оценок пока нет
- EpidemiologyДокумент36 страницEpidemiologyhendra2darmawan50% (2)
- 2 Epidemiology TerminologyДокумент33 страницы2 Epidemiology Terminologynithin shenoiОценок пока нет
- Epidemiology BooksДокумент5 страницEpidemiology BooksAdrin Ma'rufОценок пока нет
- Basic EpidemiologyДокумент54 страницыBasic EpidemiologyJennifer Dotado MaderazoОценок пока нет
- History of EpidemiologyДокумент48 страницHistory of EpidemiologyHaseeb AhmadОценок пока нет
- Observation Designs in EpidemiologyДокумент20 страницObservation Designs in EpidemiologyChristian JeffersonОценок пока нет
- Campbell Systematic Reviews - 2017 - Schmucker - Sexual Offender Treatment For Reducing Recidivism Among Convicted SexДокумент78 страницCampbell Systematic Reviews - 2017 - Schmucker - Sexual Offender Treatment For Reducing Recidivism Among Convicted SexCamila SorianoОценок пока нет
- Ars Alb Study KeralaДокумент129 страницArs Alb Study KeralaAdriana Carrillo MendozaОценок пока нет
- 3 Study DesignДокумент60 страниц3 Study DesignNour KoraneОценок пока нет
- Table of ContentsДокумент2 страницыTable of ContentsVincent PosadasОценок пока нет
- Epidemiological Studies - A Practical GuideДокумент256 страницEpidemiological Studies - A Practical GuideCUCUTA JUAN DIEGO HERNANDEZ LALINDEОценок пока нет
- Sujoy Da FinalДокумент67 страницSujoy Da FinalArtist Sujoy TontubayОценок пока нет
- Transitional Care For Adolescents With HIV: Characteristics and Current Practices of The Adolescent Trials Network Systems of CareДокумент133 страницыTransitional Care For Adolescents With HIV: Characteristics and Current Practices of The Adolescent Trials Network Systems of CarePatricia Ribeiro MartinsОценок пока нет
- Lect3 DescriptiveEpiPhD2021Документ30 страницLect3 DescriptiveEpiPhD2021Kanwal KhanОценок пока нет
- Epidemiology An Introduction PrintableДокумент32 страницыEpidemiology An Introduction PrintableAmanda RutllantОценок пока нет
- Lect3-Introduction To Study Designs Desciptive StudiesДокумент30 страницLect3-Introduction To Study Designs Desciptive StudiesKanwal KhanОценок пока нет
- Important Factors For Changing Plastic Consumption Among HighlyДокумент78 страницImportant Factors For Changing Plastic Consumption Among HighlyKristine Joy KatigbakОценок пока нет
- Adult Infectious DiseasesДокумент65 страницAdult Infectious DiseasesMohammedОценок пока нет
- Burger Allen Exercises pdf1Документ133 страницыBurger Allen Exercises pdf1lucky 116Оценок пока нет
- Biomed SD 2021-22Документ95 страницBiomed SD 2021-22Adelaida Pallas NomenОценок пока нет
- Making Rapid Response Real: Change Management and Organizational Learning in Critical Patient CareОт EverandMaking Rapid Response Real: Change Management and Organizational Learning in Critical Patient CareОценок пока нет
- FULLTEXT01Документ111 страницFULLTEXT01Ana Xiomara CortésОценок пока нет
- Assessing Frequency of Migraine It's Associated Factors Among The Undergraduate Students of Gajju Khan Medical College, SwabiДокумент46 страницAssessing Frequency of Migraine It's Associated Factors Among The Undergraduate Students of Gajju Khan Medical College, Swabiammar hussain darОценок пока нет
- AmmarДокумент45 страницAmmarammar hussain darОценок пока нет
- Christian Research WorkДокумент71 страницаChristian Research WorkJamesОценок пока нет
- Morris2022 ARAP1D Dissertation OSFДокумент94 страницыMorris2022 ARAP1D Dissertation OSFFink ThanchanokОценок пока нет
- Final For-Soft BindingДокумент101 страницаFinal For-Soft BindingangelieshaynnmtalagtagОценок пока нет
- Final Report UEA-MORI Risk Survey 2002Документ60 страницFinal Report UEA-MORI Risk Survey 2002Daniel VenablesОценок пока нет
- Oklahoma Notes SurgeryДокумент200 страницOklahoma Notes SurgeryyasinoОценок пока нет
- Using Acupuncture To Treat Depression A FeasibilitДокумент6 страницUsing Acupuncture To Treat Depression A FeasibilitErika ChavesОценок пока нет
- Recovery, Relapse, and Episodes of Default in The Management of Acute Malnutrition in Children in Humanitarian Emergencies: A Systematic ReviewДокумент38 страницRecovery, Relapse, and Episodes of Default in The Management of Acute Malnutrition in Children in Humanitarian Emergencies: A Systematic ReviewOxfamОценок пока нет
- 4937442Документ92 страницы4937442john488Оценок пока нет
- Randomized TrialsДокумент45 страницRandomized TrialsSyed Sanan shahОценок пока нет
- Concordance Adherence and Compliance in Medicine Taking PDFДокумент311 страницConcordance Adherence and Compliance in Medicine Taking PDFAlexandrahautaОценок пока нет
- Topic Research DesignДокумент51 страницаTopic Research Designsultana rajeaОценок пока нет
- 52554Документ44 страницы52554fatehatun noorОценок пока нет
- CH 16 Digestion and Absorption Part 3Документ3 страницыCH 16 Digestion and Absorption Part 3fatehatun noorОценок пока нет
- In A Novel Cabinet Dryer: Yasmin, S., Hasan, M., Sohany, M. and Sarker, M.S.HДокумент9 страницIn A Novel Cabinet Dryer: Yasmin, S., Hasan, M., Sohany, M. and Sarker, M.S.Hfatehatun noorОценок пока нет
- FermentationДокумент14 страницFermentationfatehatun noorОценок пока нет
- There Are Many Different Types of Music in The World TodayДокумент1 страницаThere Are Many Different Types of Music in The World Todayfatehatun noor100% (1)
- Index: Serial No. Subject Page NoДокумент2 страницыIndex: Serial No. Subject Page Nofatehatun noorОценок пока нет
- Chemical Hazards Chemical Hazards: 4.1 ExposureДокумент20 страницChemical Hazards Chemical Hazards: 4.1 Exposurefatehatun noorОценок пока нет
- Introduction To Global Health: DR Yoga NathanДокумент50 страницIntroduction To Global Health: DR Yoga Nathanfatehatun noorОценок пока нет
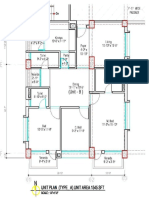
- Design Shopnonagar 2Документ3 страницыDesign Shopnonagar 2fatehatun noorОценок пока нет
- Is 5838 1970Документ12 страницIs 5838 1970fatehatun noorОценок пока нет
- S TR GEN ID (Component Marking) (Rev 3 2009) - AN Marked UpДокумент6 страницS TR GEN ID (Component Marking) (Rev 3 2009) - AN Marked UpsnclgsraoОценок пока нет
- Mean Variance Portfolio TheoryДокумент85 страницMean Variance Portfolio TheoryEbenezerОценок пока нет
- Significance of GodboleДокумент5 страницSignificance of GodbolehickeyvОценок пока нет
- Improve On-Time DeliveriesДокумент24 страницыImprove On-Time DeliveriesUdayОценок пока нет
- Lec 4 - 4th WeekДокумент40 страницLec 4 - 4th Weekrajpoot aliОценок пока нет
- Determinants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Документ3 страницыDeterminants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Apurv ChitranshОценок пока нет
- Top Ten Myths About The BrainДокумент5 страницTop Ten Myths About The BrainfayazalamaligОценок пока нет
- NAT-REVIEWER-IN-PHYSICAL EDUCATIONДокумент4 страницыNAT-REVIEWER-IN-PHYSICAL EDUCATIONMira Rochenie CuranОценок пока нет
- AssessmentДокумент3 страницыAssessmentpalflaxОценок пока нет
- Electricity NotesДокумент35 страницElectricity Notesapi-277818647Оценок пока нет
- Week 1 - NATURE AND SCOPE OF ETHICSДокумент12 страницWeek 1 - NATURE AND SCOPE OF ETHICSRegielyn CapitaniaОценок пока нет
- Presentation On 4G TechnologyДокумент23 страницыPresentation On 4G TechnologyFresh EpicОценок пока нет
- Fully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019Документ20 страницFully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019lazareviciОценок пока нет
- 3-History Rock Cut MonumentДокумент136 страниц3-History Rock Cut MonumentkrishnaОценок пока нет
- Elements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesДокумент8 страницElements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesSadman Shaid SaadОценок пока нет
- 3rd Quarter Exam (Statistics)Документ4 страницы3rd Quarter Exam (Statistics)JERALD MONJUANОценок пока нет
- The Light Fantastic by Sarah CombsДокумент34 страницыThe Light Fantastic by Sarah CombsCandlewick PressОценок пока нет
- Parts Catalogue of Foton: (TC2A504-034K)Документ132 страницыParts Catalogue of Foton: (TC2A504-034K)МаксимОценок пока нет
- HCPL 316J 000eДокумент34 страницыHCPL 316J 000eElyes MbarekОценок пока нет
- Math COT 3Документ18 страницMath COT 3Icy Mae SenadosОценок пока нет
- Design and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Документ5 страницDesign and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Saravanan ViswakarmaОценок пока нет
- 4 Force & ExtensionДокумент13 страниц4 Force & ExtensionSelwah Hj AkipОценок пока нет
- DOC-20161226-WA0009 DiagramaДокумент61 страницаDOC-20161226-WA0009 DiagramaPedroОценок пока нет
- Food Taste Panel Evaluation Form 2Документ17 страницFood Taste Panel Evaluation Form 2Akshat JainОценок пока нет
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Документ18 страниц300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoОценок пока нет