Вам также может понравиться
- Clinical StudyДокумент9 страницClinical StudyNurul Dwi LestariОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- OsdiДокумент2 страницыOsdiFairuz PaiОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Clinical StudyДокумент9 страницClinical StudyNurul Dwi LestariОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Learning Journal Hari Ke 7Документ1 страницаLearning Journal Hari Ke 7Nurul Dwi LestariОценок пока нет
- ASA Classifications 4-09Документ2 страницыASA Classifications 4-09FaridahMaksumОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- # Diabetes, Triglyceride Levels, and Other Risk Factors For Glaucoma in The National Health and Nutrition Examination Survey 2005-2008Документ6 страниц# Diabetes, Triglyceride Levels, and Other Risk Factors For Glaucoma in The National Health and Nutrition Examination Survey 2005-2008fitriahendricoОценок пока нет
- Etiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyДокумент9 страницEtiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyNurul Dwi LestariОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Etiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyДокумент9 страницEtiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyNurul Dwi LestariОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Association of Kidney FunctionДокумент22 страницыAssociation of Kidney FunctionNurul Dwi LestariОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- CT scan reveals brain injury detailsДокумент31 страницаCT scan reveals brain injury detailsNurul Dwi LestariОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Pathophysiology and Treatment of Glaucoma PDFДокумент22 страницыThe Pathophysiology and Treatment of Glaucoma PDFNurul Dwi LestariОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Kjo 32 172Документ10 страницKjo 32 172Nurul Dwi LestariОценок пока нет
- Antibiotics and Urinary Tract InfectionsДокумент153 страницыAntibiotics and Urinary Tract InfectionsVhery Feather FriendsCommunityОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Bab 24 Dasar Dasar Penyakit Akibat KerjaДокумент2 страницыBab 24 Dasar Dasar Penyakit Akibat KerjaLim MichaelОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Effect of Dengue Hemorrhagic Fever on Thrombomodulin LevelДокумент5 страницEffect of Dengue Hemorrhagic Fever on Thrombomodulin LevelNurul Dwi LestariОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Bab 10 Pemeriksaan Fisis Umum PDFДокумент17 страницBab 10 Pemeriksaan Fisis Umum PDFNurul Dwi LestariОценок пока нет
- Length/height-For-Age BOYS: Birth To 5 Years (Z-Scores)Документ1 страницаLength/height-For-Age BOYS: Birth To 5 Years (Z-Scores)Malisa LukmanОценок пока нет
- Association Between Interleukin8 and Severity of DSSДокумент5 страницAssociation Between Interleukin8 and Severity of DSSmarsyaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Neil M. Borden - 3D Angiographic Atlas of Neurovascular Anatomy and Pathology (2006) PDFДокумент285 страницNeil M. Borden - 3D Angiographic Atlas of Neurovascular Anatomy and Pathology (2006) PDFNurul Dwi Lestari100% (1)
- New File 03.17.2018Документ7 страницNew File 03.17.2018Nurul Dwi LestariОценок пока нет
- Ipd UiДокумент2 страницыIpd UiDewi Felayati GusniОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Goal-Directed Fluid Therapy Does Not Reduce Primary Postoperative Ileus After Elective Laparoscopic Colorectal SurgeryДокумент14 страницGoal-Directed Fluid Therapy Does Not Reduce Primary Postoperative Ileus After Elective Laparoscopic Colorectal SurgeryNurul Dwi LestariОценок пока нет
- Bab 12 Sendi PDFДокумент58 страницBab 12 Sendi PDFNurul Dwi LestariОценок пока нет
- Text Book Reading "Review of 3D Angiographic Atlas of Neurovascular Anatomy and Pathology Book "Документ64 страницыText Book Reading "Review of 3D Angiographic Atlas of Neurovascular Anatomy and Pathology Book "Nurul Dwi LestariОценок пока нет
- 0-00015Документ8 страниц0-00015Nurul Dwi LestariОценок пока нет
- WHO Pain LadderДокумент1 страницаWHO Pain LadderBagus Burhan MuhammadОценок пока нет
- Goal-Directed Fluid Therapy Does Not Reduce Primary Postoperative Ileus After Elective Laparoscopic Colorectal SurgeryДокумент14 страницGoal-Directed Fluid Therapy Does Not Reduce Primary Postoperative Ileus After Elective Laparoscopic Colorectal SurgeryNurul Dwi LestariОценок пока нет
- Effects of Different Crystalloid Solutions On Hemodynamics, Peripheral Perfusion, and The Microcirculation in Experimental Abdominal SepsisДокумент11 страницEffects of Different Crystalloid Solutions On Hemodynamics, Peripheral Perfusion, and The Microcirculation in Experimental Abdominal SepsisNurul Dwi LestariОценок пока нет
- Journal ReadingДокумент17 страницJournal ReadingNurul Dwi LestariОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- 2019 European League Against Rheumatism American College of Rheumatology Classification Criteria For Systemic Lupus ErythematosusДокумент9 страниц2019 European League Against Rheumatism American College of Rheumatology Classification Criteria For Systemic Lupus Erythematosusnacxit6Оценок пока нет
- Dosage Lec - Unit 2 Drug DiscoveryДокумент8 страницDosage Lec - Unit 2 Drug DiscoveryJohn Lorenz BordadorОценок пока нет
- Bioinformatics in Drug Discovery A ReviewДокумент3 страницыBioinformatics in Drug Discovery A ReviewBONFRINGОценок пока нет
- EAP Reading Worksheet Week 3 - We Are CyborgsДокумент3 страницыEAP Reading Worksheet Week 3 - We Are CyborgsAnh HoàngОценок пока нет
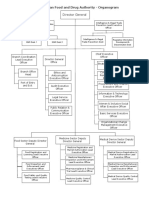
- EFDA Organogram English VersionДокумент6 страницEFDA Organogram English VersionRobsan YasinОценок пока нет
- Aromatherapy in Psychiatric DisordersДокумент24 страницыAromatherapy in Psychiatric Disordersxiuhtlaltzin100% (3)
- Tamiflu Epar Scientific Discussion enДокумент25 страницTamiflu Epar Scientific Discussion ensubhasisknkОценок пока нет
- Unit 5.5 - JCIДокумент38 страницUnit 5.5 - JCILakshmi Sowjanya AkurathiОценок пока нет
- Pharma R&D Pipeline Review 2011Документ12 страницPharma R&D Pipeline Review 2011Koushik BhattacharyyaОценок пока нет
- EvistaДокумент18 страницEvistaBrankoPopovićОценок пока нет
- Marketing and Sales Roles in The Pharmaceutical IndustryДокумент32 страницыMarketing and Sales Roles in The Pharmaceutical Industrymeet2abhayОценок пока нет
- Alzheimers PDFДокумент86 страницAlzheimers PDFThewa ChungwatanakitОценок пока нет
- Greater Washington Research & Development Facilities DirectoryДокумент143 страницыGreater Washington Research & Development Facilities DirectoryM-NCPPCОценок пока нет
- Studies On Tractor Related Injuries inДокумент8 страницStudies On Tractor Related Injuries insln_rjОценок пока нет
- Interprofessional Collaborative Practice TodayДокумент147 страницInterprofessional Collaborative Practice TodayBrittany Dedeaux100% (3)
- List of Thesis Topics in DermatologyДокумент5 страницList of Thesis Topics in Dermatologysarahjimenezriverside100% (2)
- 2020 Queens Awards Enterprise Press BookДокумент126 страниц2020 Queens Awards Enterprise Press BookCrowdfundInsiderОценок пока нет
- Life Sciences Data Hub From Oracle Health Sciences: Enabling Global Regulatory ComplianceДокумент3 страницыLife Sciences Data Hub From Oracle Health Sciences: Enabling Global Regulatory ComplianceSameer PatilОценок пока нет
- Isometric Strength and Its Relationship To Dynamic Performance A Systematic ReviewДокумент10 страницIsometric Strength and Its Relationship To Dynamic Performance A Systematic Reviewlinoco1Оценок пока нет
- Novartis Annual Report 2014 Pipeline InnovationДокумент3 страницыNovartis Annual Report 2014 Pipeline InnovationFauzan FikriОценок пока нет
- Bio Basque Company Directory 2011Документ58 страницBio Basque Company Directory 2011gax1977Оценок пока нет
- Samah Aboulsoud-ResumeДокумент2 страницыSamah Aboulsoud-Resumeapi-400387662Оценок пока нет
- IICRДокумент17 страницIICRMukund SharmaОценок пока нет
- Updated Open Elective For Final 7th Semester (Syllabus)Документ83 страницыUpdated Open Elective For Final 7th Semester (Syllabus)Vikash KumarОценок пока нет
- Clinical Pharmacology IntroductionДокумент24 страницыClinical Pharmacology IntroductionSunilОценок пока нет
- BMS1042 Module 1: Biostatistics BasicsДокумент7 страницBMS1042 Module 1: Biostatistics BasicshafsatutuОценок пока нет
- D-Limonene: Safety and Clinical ApplicationsДокумент6 страницD-Limonene: Safety and Clinical ApplicationsbreakingthesilenceОценок пока нет
- Ethics Public HealthДокумент79 страницEthics Public HealthStalin Edegba EwoigbokhanОценок пока нет
- Your Guide To: Advancing Your Career in BiotechnologyДокумент29 страницYour Guide To: Advancing Your Career in BiotechnologyRanjith KumarОценок пока нет
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (13)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 3.5 из 5 звезд3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОценок пока нет
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (78)