Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Installation and Setup Guide For The Cisco Active Directory Agent, Release 1.0Документ62 страницыInstallation and Setup Guide For The Cisco Active Directory Agent, Release 1.0Madelaine Velasquez Blacutt100% (1)
- Analysis of Excessive Hydrogen Generation in TransformersДокумент8 страницAnalysis of Excessive Hydrogen Generation in TransformersandikaubhОценок пока нет
- BHNS Citation RawДокумент9 страницBHNS Citation Rawfiras frsОценок пока нет
- Anatomy and Physiology MCQ Questions with ExplanationsДокумент19 страницAnatomy and Physiology MCQ Questions with Explanationsfiras frsОценок пока нет
- MalariaДокумент23 страницыMalariafiras frs100% (1)
- Increased Number of Febrile Seizures in Very Preterm ChildrenДокумент8 страницIncreased Number of Febrile Seizures in Very Preterm ChildrenFarin MauliaОценок пока нет
- Pharmacotherapy During Pregnancy, Childbirth and LactationДокумент6 страницPharmacotherapy During Pregnancy, Childbirth and Lactationfiras frsОценок пока нет
- NeuroanatomyДокумент4 страницыNeuroanatomyfiras frsОценок пока нет
- Pathophysiology of Cor Pulmonale: Firazullah H1A015024Документ4 страницыPathophysiology of Cor Pulmonale: Firazullah H1A015024firas frsОценок пока нет
- Sociodemographic Factors To Dengue Hemmorrhagic FeДокумент7 страницSociodemographic Factors To Dengue Hemmorrhagic Fefiras frsОценок пока нет
- International Headache Classification III ICHD III 2013 Beta 1Документ180 страницInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanОценок пока нет
- Development of A Questionnaire On Knowledge Attitude and Practice About Immunization Among Iraqi Parents 11Документ8 страницDevelopment of A Questionnaire On Knowledge Attitude and Practice About Immunization Among Iraqi Parents 11firas frsОценок пока нет
- WWW Mathworks inДокумент7 страницWWW Mathworks inRagini SharmaОценок пока нет
- Electronic Principles IV, 7-8. Military Curriculum Materials For Vocational and Technical Education.Документ571 страницаElectronic Principles IV, 7-8. Military Curriculum Materials For Vocational and Technical Education.SolОценок пока нет
- LC 72322Документ13 страницLC 72322thecanislupusОценок пока нет
- UCE802 Earthquake SyllabusДокумент2 страницыUCE802 Earthquake Syllabuskullu88Оценок пока нет
- GR/KWH, KG/HR or Tons/Month.: ScopeДокумент5 страницGR/KWH, KG/HR or Tons/Month.: ScopeThaigroup CementОценок пока нет
- Dynamic Programming Algorithm Explained in ECE 551 LectureДокумент11 страницDynamic Programming Algorithm Explained in ECE 551 Lectureadambose1990Оценок пока нет
- Datasheet PDFДокумент16 страницDatasheet PDFSergio Daniel BarretoОценок пока нет
- Areas Related To CircleДокумент32 страницыAreas Related To CircleGiorno GiovannaОценок пока нет
- Student's Error Analysis in Finishing Mathematic Word Problem Based Newman AnalysisДокумент11 страницStudent's Error Analysis in Finishing Mathematic Word Problem Based Newman AnalysisguanyitorОценок пока нет
- VT2009B Eng 02 953680Документ2 страницыVT2009B Eng 02 953680gabrieltracto100% (1)
- The Windows Process Journey v6 0 Aug2023 1691726739Документ53 страницыThe Windows Process Journey v6 0 Aug2023 1691726739blakboukiОценок пока нет
- Mechanical Technology Concepts: Applied ThermodynamicsДокумент45 страницMechanical Technology Concepts: Applied ThermodynamicsLe0 GamingОценок пока нет
- Brushless DC Motor Control Using PLCДокумент6 страницBrushless DC Motor Control Using PLCvuluyen6688Оценок пока нет
- Manual Hawk 4000 PDFДокумент158 страницManual Hawk 4000 PDFNebur MtzaОценок пока нет
- Roll Handling Data Form: Company DetailsДокумент1 страницаRoll Handling Data Form: Company DetailsAlfredo MinchezОценок пока нет
- Technology: ControlsДокумент32 страницыTechnology: ControlsAli Hossain AdnanОценок пока нет
- ACI229Документ18 страницACI229Francisco CalderónОценок пока нет
- Training Seminar ON GSM Held at BSNL: Presented By: Charli Bagga Kriti Rastogi (AEI-08)Документ51 страницаTraining Seminar ON GSM Held at BSNL: Presented By: Charli Bagga Kriti Rastogi (AEI-08)Ankita BharadwajОценок пока нет
- Material Data Sheet: Casting Material: Carbon Steel GS60 DIN 1681: GS-60 Cast SteelДокумент3 страницыMaterial Data Sheet: Casting Material: Carbon Steel GS60 DIN 1681: GS-60 Cast SteelShailesh BhanushaliОценок пока нет
- Service Manual Trucks: Fault Codes Tachograph Tac-Dig, Tac-Dig2Документ70 страницService Manual Trucks: Fault Codes Tachograph Tac-Dig, Tac-Dig2Deny Adi IrawanОценок пока нет
- Solid angles in perspective: Ω, have a small but essential role in physics. For example, howДокумент8 страницSolid angles in perspective: Ω, have a small but essential role in physics. For example, howashkarkabeer08Оценок пока нет
- Bayesian Network Approach To Root Cause DiagnosisДокумент17 страницBayesian Network Approach To Root Cause DiagnosisDhinesh GanesanОценок пока нет
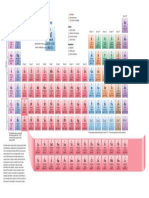
- Periodic TableДокумент1 страницаPeriodic TableChemist MookaОценок пока нет
- Product Guide (English 140702)Документ11 страницProduct Guide (English 140702)Dineshkumar MahedranОценок пока нет
- Alexander DisciplineДокумент7 страницAlexander DisciplinePatricia TagartaОценок пока нет
- Tehandler KatoДокумент15 страницTehandler KatoWalterОценок пока нет
- Danfoss PVE - Series - 7 - Technical - Information PDFДокумент56 страницDanfoss PVE - Series - 7 - Technical - Information PDFJuan Felipe Garza GОценок пока нет
- JavaДокумент20 страницJavaSivasakthi MarimuthuОценок пока нет