Вам также может понравиться
- The Effectiveness of Oxymetazoline Plus Intranasal Steroid in The Treatment of Chronic Rhinitis: A Randomised Controlled TrialДокумент9 страницThe Effectiveness of Oxymetazoline Plus Intranasal Steroid in The Treatment of Chronic Rhinitis: A Randomised Controlled TrialFaris LahmadiОценок пока нет
- VIVA Training in ENTДокумент8 страницVIVA Training in ENTOpi PippoОценок пока нет
- Chen 2018Документ11 страницChen 2018ayunda rinataОценок пока нет
- Efficacy and Side Effects of Antibiotics in The Treatment ofДокумент7 страницEfficacy and Side Effects of Antibiotics in The Treatment ofmgvbОценок пока нет
- Jurnal THTДокумент14 страницJurnal THTLaras Asri FatahaniОценок пока нет
- 1945892419851312Документ10 страниц1945892419851312kasandraharahapОценок пока нет
- Stolovitzky Et Al 2021 Effect of Radiofrequency Neurolysis On The Symptoms of Chronic Rhinitis A Randomized ControlledДокумент7 страницStolovitzky Et Al 2021 Effect of Radiofrequency Neurolysis On The Symptoms of Chronic Rhinitis A Randomized ControlledfrischaОценок пока нет
- Cryotherapy For The Treatment of Chronic Rhinitis A Qualitative Systematic ReviewДокумент11 страницCryotherapy For The Treatment of Chronic Rhinitis A Qualitative Systematic ReviewAnneОценок пока нет
- 23.06.24 - 2021-Chin J Integr Med.27 (2) .83 - Allergic Rhinitis - Acu GuidelineДокумент8 страниц23.06.24 - 2021-Chin J Integr Med.27 (2) .83 - Allergic Rhinitis - Acu Guidelinehj4gpphdysОценок пока нет
- Intranasal Corticosteroids in Management of Acute Sinusitis: A Systematic Review and Meta-AnalysisДокумент9 страницIntranasal Corticosteroids in Management of Acute Sinusitis: A Systematic Review and Meta-AnalysisBudi KhangОценок пока нет
- Comparison of Different Biologics For Treating Chronic Rhinosinusitis With Nasal Polyps: A Network AnalysisДокумент18 страницComparison of Different Biologics For Treating Chronic Rhinosinusitis With Nasal Polyps: A Network AnalysisZha Zha Nurul ZahraОценок пока нет
- 2ARandomizedControlledVol24No2 3june Sep2006P97Документ7 страниц2ARandomizedControlledVol24No2 3june Sep2006P97I Made AryanaОценок пока нет
- MDR TBДокумент1 страницаMDR TBIrma Nur Rizka HanifahОценок пока нет
- Fphar 12 731201Документ12 страницFphar 12 731201I Made AryanaОценок пока нет
- Chitsuthipakorn 2021Документ12 страницChitsuthipakorn 2021Diko KoestantyoОценок пока нет
- 0 - Ceor 10 747Документ13 страниц0 - Ceor 10 747Ika RohaetiОценок пока нет
- Articol Coacaz Negru PDFДокумент5 страницArticol Coacaz Negru PDFManu MandaОценок пока нет
- Rudolf Steiner - The Warmth Course The Theory of HeatДокумент11 страницRudolf Steiner - The Warmth Course The Theory of HeatmedellincolombiaОценок пока нет
- MRSA Chronic Bacterial Laryngitis: A Growing Problem: Patrick S. Carpenter, MD Katherine A. Kendall, MDДокумент5 страницMRSA Chronic Bacterial Laryngitis: A Growing Problem: Patrick S. Carpenter, MD Katherine A. Kendall, MDIntan Nur HijrinaОценок пока нет
- Grasso 2018Документ5 страницGrasso 2018Nia DefinisiОценок пока нет
- Ordi-Ros J, Et Al, 2017.Документ8 страницOrdi-Ros J, Et Al, 2017.Suhenri SiahaanОценок пока нет
- Consensus Guidance of Nebulizer Therapy For Acute RhinosinusitisДокумент7 страницConsensus Guidance of Nebulizer Therapy For Acute RhinosinusitisYassir ElemamОценок пока нет
- Recurrent Acute Rhinosinusitis Prevention by Azithromycin in Children With Nonallergic RhinitisДокумент7 страницRecurrent Acute Rhinosinusitis Prevention by Azithromycin in Children With Nonallergic RhinitisKeselek BakiakОценок пока нет
- The Comparison of Nasaleze and Mometasone Nasal Spray To Control The Symptoms of Allergic RhinitisДокумент5 страницThe Comparison of Nasaleze and Mometasone Nasal Spray To Control The Symptoms of Allergic RhinitisCarlos Alberto Aliaga DulantoОценок пока нет
- Saline Nasal Irrigations For Chronic Rhinosinusitis: From Everyday Practice To Evidence-Based Medicine. An UpdateДокумент6 страницSaline Nasal Irrigations For Chronic Rhinosinusitis: From Everyday Practice To Evidence-Based Medicine. An UpdatehanarОценок пока нет
- Advanced Clinical Pharmacology and Toxicology, TherapeuticsДокумент2 страницыAdvanced Clinical Pharmacology and Toxicology, Therapeuticsscience world publishingОценок пока нет
- Early Treatment of Perennial Rhinitis With Budesonide or Cetirizine and Its Effect On Long-Term OutcomeДокумент7 страницEarly Treatment of Perennial Rhinitis With Budesonide or Cetirizine and Its Effect On Long-Term Outcomeselvi aklailia rosaОценок пока нет
- Journal 2 Steven Hartanto Kurniawan - A Comparative Study To Assess The Efficacy of Fluticasone and Mometasone in Allergic RhinitisДокумент5 страницJournal 2 Steven Hartanto Kurniawan - A Comparative Study To Assess The Efficacy of Fluticasone and Mometasone in Allergic Rhinitissteven hkОценок пока нет
- Antituberculosis Drug Associated DRESS A Case SeriesДокумент8 страницAntituberculosis Drug Associated DRESS A Case SeriesVivi MaifitrizaОценок пока нет
- Yasmeen 2020Документ16 страницYasmeen 2020Rafaela Queiroz MascarenhasОценок пока нет
- Research ArticleДокумент6 страницResearch ArticleReffy AdhaОценок пока нет
- Allergology InternationalДокумент9 страницAllergology Internationalvijay dagdiОценок пока нет
- Acfrogcmuqv1z T0qaucxvbfwtfin2xu Xkrzp4ddeso7qwbd Fha38sq6mihfw2aozwxn5r0mxgmgmkvemhr46tntlwea3quddq9w2pmvyn6by5wqcyi7ge8gmmnzlzhis 1dzejbeghuvr9bapДокумент7 страницAcfrogcmuqv1z T0qaucxvbfwtfin2xu Xkrzp4ddeso7qwbd Fha38sq6mihfw2aozwxn5r0mxgmgmkvemhr46tntlwea3quddq9w2pmvyn6by5wqcyi7ge8gmmnzlzhis 1dzejbeghuvr9bapFareed KhanОценок пока нет
- Gómez-García 2016Документ10 страницGómez-García 2016Rafaela Queiroz MascarenhasОценок пока нет
- Treatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical SteroidsДокумент37 страницTreatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical SteroidsA.Оценок пока нет
- Jurnal Rinitis Vasomotor 2 PDFДокумент14 страницJurnal Rinitis Vasomotor 2 PDFNasikhatulОценок пока нет
- Xu 2020Документ10 страницXu 2020Risky PerdanaОценок пока нет
- 16 RaДокумент10 страниц16 RaNitish TankОценок пока нет
- Association of Facial Exercise With The AppearanceДокумент4 страницыAssociation of Facial Exercise With The AppearanceintenselightОценок пока нет
- NSI in Pediatric Rhinosinusitis PDFДокумент19 страницNSI in Pediatric Rhinosinusitis PDFtopОценок пока нет
- American Journal of Otolaryngology - Head and Neck Medicine and SurgeryДокумент4 страницыAmerican Journal of Otolaryngology - Head and Neck Medicine and SurgerySyalara FatharaniОценок пока нет
- The Use of Inhaled NaceДокумент7 страницThe Use of Inhaled NaceYondi Piter PapulungОценок пока нет
- BMJ j3887 FullДокумент10 страницBMJ j3887 FullRiri Maisytoh PutriОценок пока нет
- Intranasal CorticosteroidДокумент9 страницIntranasal CorticosteroidIRAОценок пока нет
- Ed 58Документ8 страницEd 58Luís CorreiaОценок пока нет
- Mucoactive Agents in The Therapy of Upper Respiratory Airways Infections: Fair To Describe Them Just As Mucoactive?Документ9 страницMucoactive Agents in The Therapy of Upper Respiratory Airways Infections: Fair To Describe Them Just As Mucoactive?Korry Meliana PangaribuanОценок пока нет
- 3Документ9 страниц3Niken KuncorowatiОценок пока нет
- The Antimicrobial Activity of Nanoparticles Presen PDFДокумент23 страницыThe Antimicrobial Activity of Nanoparticles Presen PDFArun KumarrvОценок пока нет
- Catgutpuntura Rinitis AlérgicaДокумент11 страницCatgutpuntura Rinitis AlérgicaDubichelОценок пока нет
- A Comparative Study To Determine The Accuracy of Direct Susceptibility Testing With Conventional Antimicrobial Susceptibility TestingДокумент7 страницA Comparative Study To Determine The Accuracy of Direct Susceptibility Testing With Conventional Antimicrobial Susceptibility TestingIJAR JOURNALОценок пока нет
- NAyakДокумент15 страницNAyakstanleyОценок пока нет
- Article Review Topical Corticosteroid Irrigations in Chronic RhinosinusitisДокумент7 страницArticle Review Topical Corticosteroid Irrigations in Chronic Rhinosinusitisgifar ihsanОценок пока нет
- Montelukast With Desloratadine or LevocetirizineДокумент8 страницMontelukast With Desloratadine or LevocetirizineAnonymous so6ZnlKywОценок пока нет
- Effectiveness of Individualized Homeopathic Treatment in Perennial Allergic Rhinitis (PAR)Документ4 страницыEffectiveness of Individualized Homeopathic Treatment in Perennial Allergic Rhinitis (PAR)sai sindhujaОценок пока нет
- Mitomycin C in The Endoscopic Treatment of Laryngotracheal Stenosis Systematic Review and Proportional Meta-AnalysisДокумент12 страницMitomycin C in The Endoscopic Treatment of Laryngotracheal Stenosis Systematic Review and Proportional Meta-AnalysisImam Taqwa DrughiОценок пока нет
- Jurnal THTДокумент7 страницJurnal THTFenti FatonahОценок пока нет
- Could Local Antibiotics Be Included in The Treatment of Acute Anal Fissure?Документ4 страницыCould Local Antibiotics Be Included in The Treatment of Acute Anal Fissure?luis beltranОценок пока нет
- Vol. 5 No. 2 April 2021 Jurnal Ilmiah KohesiДокумент7 страницVol. 5 No. 2 April 2021 Jurnal Ilmiah KohesiadindaОценок пока нет
- Clinical Applications of Nuclear Medicine Targeted TherapyОт EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriОценок пока нет
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationОт EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehОценок пока нет
- Abstrack Delibrate PracticeДокумент2 страницыAbstrack Delibrate PracticetopОценок пока нет
- Water Colored Splashes PowerPoint TemplateДокумент36 страницWater Colored Splashes PowerPoint TemplateAna Carmela DomingoОценок пока нет
- Kertas Resep YudiДокумент1 страницаKertas Resep YuditopОценок пока нет
- Slit LampbiomicrosДокумент18 страницSlit LampbiomicrostopОценок пока нет
- Eye ManualДокумент56 страницEye Manualbashir019Оценок пока нет
- The Open Ophthalmology JournalДокумент5 страницThe Open Ophthalmology JournalFenny Duma SariОценок пока нет
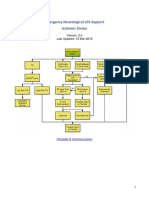
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Документ22 страницыEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationДокумент3 страницыPediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationtopОценок пока нет
- Total ModalДокумент1 страницаTotal ModaltopОценок пока нет
- Eye TraumaДокумент19 страницEye TraumatopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationsДокумент15 страницPediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationstopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma MedicationДокумент8 страницPediatric Non-Hodgkin Lymphoma MedicationtopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesДокумент5 страницPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologyДокумент11 страницPediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologytopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Differential DiagnosesДокумент2 страницыPediatric Non-Hodgkin Lymphoma Differential DiagnosestopОценок пока нет
- Radiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomasДокумент26 страницRadiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomastopОценок пока нет
- Role of PET/CT in Malignant Pediatric Lymphoma: Original ArticleДокумент11 страницRole of PET/CT in Malignant Pediatric Lymphoma: Original ArticletopОценок пока нет
- CSS Jurnal DR IdratДокумент8 страницCSS Jurnal DR IdrattopОценок пока нет
- Role of Limited Whole-BodyДокумент9 страницRole of Limited Whole-BodytopОценок пока нет
- Materi Lat DesignДокумент27 страницMateri Lat DesigntopОценок пока нет
- Presentation 1Документ8 страницPresentation 1topОценок пока нет
- Jurnal Asli CSS - Khalida Khairunnisa - DR - ErniДокумент7 страницJurnal Asli CSS - Khalida Khairunnisa - DR - ErnitopОценок пока нет
- Poster Publik & Poster IlmiahДокумент10 страницPoster Publik & Poster Ilmiahtop100% (1)
- Antibiotics in Chronic RhinosinusitisДокумент5 страницAntibiotics in Chronic RhinosinusitistopОценок пока нет
- Role of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitisДокумент5 страницRole of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitistopОценок пока нет
- Felting Fabulous Flowers Templates PDFДокумент3 страницыFelting Fabulous Flowers Templates PDFtop67% (3)
- NSI in Pediatric Rhinosinusitis PDFДокумент19 страницNSI in Pediatric Rhinosinusitis PDFtopОценок пока нет
- Guideline AoeДокумент25 страницGuideline AoetopОценок пока нет
- Anatomy and Physiology Nasal ObstructionДокумент13 страницAnatomy and Physiology Nasal ObstructiontopОценок пока нет
- Cad Import Catalog 2020 Version3Документ102 страницыCad Import Catalog 2020 Version3Anonymous 0GLtrOMОценок пока нет
- ELPR 101 - WordlistДокумент77 страницELPR 101 - WordlistAreejОценок пока нет
- Understanding of Rhinosinusitis: Complication and Implication of Rhinosinusitis Daily PracticeДокумент43 страницыUnderstanding of Rhinosinusitis: Complication and Implication of Rhinosinusitis Daily PracticeYunita Indah PalupiОценок пока нет
- English Project CovidДокумент4 страницыEnglish Project CovidKhalid RizkyОценок пока нет
- 45 of The Longest Clinical NamesДокумент3 страницы45 of The Longest Clinical NamesEva esperaОценок пока нет
- Pathophysiology and Diagnostic Procedure in Allergic RhinitisДокумент12 страницPathophysiology and Diagnostic Procedure in Allergic RhinitisSaya GantengОценок пока нет
- PEDIA Review TransesДокумент12 страницPEDIA Review TransesJennie KimОценок пока нет
- Health AssessmentДокумент23 страницыHealth AssessmentPORTRAIT OF A NURSEОценок пока нет
- A Comprehensive Acupuncture Points Database: By: Shmuel Halevi PH.DДокумент38 страницA Comprehensive Acupuncture Points Database: By: Shmuel Halevi PH.DPraveen Kumar100% (1)
- Pathophysiology and Management of Gustatory Rhinitis: Literature ReviewДокумент8 страницPathophysiology and Management of Gustatory Rhinitis: Literature ReviewmiraОценок пока нет
- 9 Health IELTS Speaking Topic PDFДокумент17 страниц9 Health IELTS Speaking Topic PDFeng7mohamed7hashimОценок пока нет
- Management of Patients With Upper Respiratory Tract DisordersДокумент93 страницыManagement of Patients With Upper Respiratory Tract DisordersErica Clerigo LandichoОценок пока нет
- Nasal Polyps Treatment MiracleДокумент46 страницNasal Polyps Treatment MiracleRyanNewEra100% (3)
- Nasal Obstruction BookДокумент7 страницNasal Obstruction BookChatradhar ChoudhuryОценок пока нет
- CS Blue Sheet Mnemonics - USMLE Step 2 CSДокумент1 страницаCS Blue Sheet Mnemonics - USMLE Step 2 CSyasir saeedОценок пока нет
- Allergic Rhinitis Is AДокумент89 страницAllergic Rhinitis Is AElena TutunaruОценок пока нет
- Lesson Plan On RhinitisДокумент15 страницLesson Plan On Rhinitiskiran mahal100% (4)
- Soal Kelas 9 Tentang LabelДокумент4 страницыSoal Kelas 9 Tentang Labelsuhartina haynaОценок пока нет
- 13 Natural Remedies For Runny NoseДокумент6 страниц13 Natural Remedies For Runny NoseAneek Kumar100% (1)
- 1 s2.0 S1319016422000652 MainДокумент7 страниц1 s2.0 S1319016422000652 MainNguyễn Diệp Huy PhongОценок пока нет
- Aria Pharm PGДокумент14 страницAria Pharm PGBlack3Fox56Оценок пока нет
- Cerebrospinal Rhinorrhoea and HomoeopathyДокумент9 страницCerebrospinal Rhinorrhoea and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- EntДокумент32 страницыEntaini natasha100% (3)
- Ent PointsДокумент9 страницEnt PointsSaiОценок пока нет
- Elsharnoby Pediatric Made EasyДокумент160 страницElsharnoby Pediatric Made Easyelmaadawy20020% (1)
- Upper Respiratory Tract Infection (Uri)Документ4 страницыUpper Respiratory Tract Infection (Uri)Anna Zhifa AbОценок пока нет
- Aria PoketДокумент8 страницAria PoketNaifmxОценок пока нет
- Case Report-Chronic Rhinosinusitis-Group 15.1.07Документ47 страницCase Report-Chronic Rhinosinusitis-Group 15.1.07Cresti Chandra PradeltaОценок пока нет
- Panadol SinusДокумент4 страницыPanadol SinusNy Ade HanifОценок пока нет
- Otc Practice Lec 3Документ106 страницOtc Practice Lec 3mahgad0% (1)