Вам также может понравиться
- Facts and Fiction On E-Cigs: What Are They?Документ6 страницFacts and Fiction On E-Cigs: What Are They?maria5basОценок пока нет
- Add 12659Документ10 страницAdd 12659Tim HoweОценок пока нет
- Harm Reduction Position Paper - Final 2Документ19 страницHarm Reduction Position Paper - Final 2G LekОценок пока нет
- Ethical Considerations of E-Cigarette Use For Tobacco Harm ReductionДокумент9 страницEthical Considerations of E-Cigarette Use For Tobacco Harm ReductiondianaОценок пока нет
- The Unique Contribution of E-Cigarettes For Tobacco Harm Reduction in Supporting Smoking Relapse PreventionДокумент7 страницThe Unique Contribution of E-Cigarettes For Tobacco Harm Reduction in Supporting Smoking Relapse PreventionBernadette OcampoОценок пока нет
- Real-World Effectiveness of E-Cigarettes When Used To Aid Smoking CessationДокумент10 страницReal-World Effectiveness of E-Cigarettes When Used To Aid Smoking CessationAsd EfgОценок пока нет
- Electronic Cigarettes and Vaping: A New Challenge in Clinical Medicine and Public Health. A Literature ReviewДокумент21 страницаElectronic Cigarettes and Vaping: A New Challenge in Clinical Medicine and Public Health. A Literature ReviewJohn Wilmer Dela CernaОценок пока нет
- Who Cop9 Oct 2021 (Letter)Документ11 страницWho Cop9 Oct 2021 (Letter)Brent StaffordОценок пока нет
- Vaping and E-Cigarettes Within The Evolving TobaccoДокумент12 страницVaping and E-Cigarettes Within The Evolving TobaccoVictor Gabriel Araújo AlexandreОценок пока нет
- Farsalinos December 2021 - FlavoursДокумент91 страницаFarsalinos December 2021 - FlavoursBrent StaffordОценок пока нет
- Knowledge and Attitudes Towards E-Cigarette Use in Lebanon and Their Associated FactorsДокумент18 страницKnowledge and Attitudes Towards E-Cigarette Use in Lebanon and Their Associated Factorsriska ameliaОценок пока нет
- T E T B P S: HE Ffects of Axes and Ans On Assive MokingДокумент38 страницT E T B P S: HE Ffects of Axes and Ans On Assive MokingBill HanneganОценок пока нет
- Ijerph 17 01971Документ22 страницыIjerph 17 01971Ancuta PatiОценок пока нет
- CHAPTER 2 CompressedДокумент9 страницCHAPTER 2 CompressedLyren Aerey GuevarraОценок пока нет
- Which Is The Role of Electronic Cigarettes in The Fight Against SmokingДокумент3 страницыWhich Is The Role of Electronic Cigarettes in The Fight Against SmokingHerald Scholarly Open AccessОценок пока нет
- Brown 2014Документ6 страницBrown 2014Carlos Herrera MezaОценок пока нет
- Pacek Et Al 2018 Conceptual Framework For Understanding Tobaco UseДокумент10 страницPacek Et Al 2018 Conceptual Framework For Understanding Tobaco UseTania Karina Álvarez MendozaОценок пока нет
- UKVIA 2021 Regs Position PaperДокумент32 страницыUKVIA 2021 Regs Position PaperBrent StaffordОценок пока нет
- The Effects of Cigarette Smoking To The Health of Automotive Grade 11 and Grade 12 Students in Computer Reseacrh Network, INC Background of The StudyДокумент9 страницThe Effects of Cigarette Smoking To The Health of Automotive Grade 11 and Grade 12 Students in Computer Reseacrh Network, INC Background of The StudyRuel OrculloОценок пока нет
- Impact of Electronic Cigarettes On Oral Health: A Review: Mahmoud Rouabhia, PHDДокумент8 страницImpact of Electronic Cigarettes On Oral Health: A Review: Mahmoud Rouabhia, PHDاحمد الزهرانيОценок пока нет
- Addressing Common Myths About Vaping ASH UK Aug 2023 BriefДокумент14 страницAddressing Common Myths About Vaping ASH UK Aug 2023 BriefakinpuddyОценок пока нет
- Thesis About Cigarette AddictionДокумент8 страницThesis About Cigarette Addictionjenniferreitherspringfield100% (1)
- Cheracteristic, PerseivedДокумент18 страницCheracteristic, Perseivedagung gusnandarОценок пока нет
- Integrating Smoking Cessation and Alcohol Use Treatment in Homeless Populations Study Protocol For A Randomized Controlled TrialДокумент12 страницIntegrating Smoking Cessation and Alcohol Use Treatment in Homeless Populations Study Protocol For A Randomized Controlled TriallabebuОценок пока нет
- Moneybass 2Документ4 страницыMoneybass 2api-285224924Оценок пока нет
- Vaping Among Youth and Young AДокумент8 страницVaping Among Youth and Young Amikeb92556Оценок пока нет
- Wilson Et Al., 2019Документ11 страницWilson Et Al., 2019امجد هليل السابلОценок пока нет
- Comparison of Biomarkers of Exposure Among US Adult Smokers, Users of ENDS, Dual Users and Nonusers 2018 - 2019Документ11 страницComparison of Biomarkers of Exposure Among US Adult Smokers, Users of ENDS, Dual Users and Nonusers 2018 - 2019akinpuddyОценок пока нет
- M ZankoДокумент6 страницM ZankoAram OtherОценок пока нет
- Review Related LiteratureДокумент7 страницReview Related Literaturehannah enopiaОценок пока нет
- Consideration of Vaping Products As An Alternative To Adult Smoking A Narrative Reviewsubstance Abuse Treatment Prevention and PolicyДокумент10 страницConsideration of Vaping Products As An Alternative To Adult Smoking A Narrative Reviewsubstance Abuse Treatment Prevention and PolicyAinin SofiaОценок пока нет
- Research Paper About Secondhand SmokeДокумент4 страницыResearch Paper About Secondhand Smokeafeaxdhwl100% (1)
- E-Cigarettes Literature ReviewДокумент5 страницE-Cigarettes Literature Reviewaflskkcez100% (1)
- BMC Public HealthДокумент25 страницBMC Public HealtharunceОценок пока нет
- Experts Call On WHO To Embrace E-Cigarettes As Tobacco Harm ReductionДокумент7 страницExperts Call On WHO To Embrace E-Cigarettes As Tobacco Harm ReductionJoan van DykОценок пока нет
- Gerry Stimson - A Tale of Two EpidemicsДокумент11 страницGerry Stimson - A Tale of Two EpidemicsmatОценок пока нет
- Ajph 2021 306416Документ12 страницAjph 2021 306416Christian F. SipinОценок пока нет
- Greehilletal Adolescenteciguse FinalacceptedversionДокумент30 страницGreehilletal Adolescenteciguse FinalacceptedversionlydОценок пока нет
- The Effectiveness of Tobacco Control Television Advertisements in Increasing The Prevalence of Smoke-Free HomesДокумент11 страницThe Effectiveness of Tobacco Control Television Advertisements in Increasing The Prevalence of Smoke-Free HomesIgnacio NuñezОценок пока нет
- Smoking Cessation Nursing InterventionsДокумент12 страницSmoking Cessation Nursing Interventionsapi-741272284Оценок пока нет
- Vaping StudyДокумент25 страницVaping StudyEve LesterОценок пока нет
- Running Head: Tobacco Addiction Challenge 1Документ7 страницRunning Head: Tobacco Addiction Challenge 1ericОценок пока нет
- Tobacco Use Literature ReviewДокумент9 страницTobacco Use Literature Reviewea7j5ys3100% (1)
- BMC Public Health: Patterns of Motivations and Ways of Quitting Smoking Among Polish Smokers: A Questionnaire StudyДокумент9 страницBMC Public Health: Patterns of Motivations and Ways of Quitting Smoking Among Polish Smokers: A Questionnaire StudyFilip RalucaОценок пока нет
- Literature Review On Passive SmokingДокумент4 страницыLiterature Review On Passive Smokingc5p0cd99100% (1)
- Smoking Dissertation TopicsДокумент5 страницSmoking Dissertation TopicsWriteMyBusinessPaperSingapore100% (1)
- The Opinions of Adults About The Ban On Cigarette Sales To MinorsДокумент10 страницThe Opinions of Adults About The Ban On Cigarette Sales To MinorsTanveer SultanОценок пока нет
- E Cigarettes 1Документ22 страницыE Cigarettes 1teacherlureinОценок пока нет
- Impact of Plain Packaging of Tobacco Products On Smoking in Adults and Children: An Elicitation of International Experts' EstimatesДокумент13 страницImpact of Plain Packaging of Tobacco Products On Smoking in Adults and Children: An Elicitation of International Experts' EstimatesEliza DNОценок пока нет
- Introduction, Conclusions, and Historical Background Relative To E-CigarettesДокумент24 страницыIntroduction, Conclusions, and Historical Background Relative To E-CigarettesScherylle Jeanne Martinez AbarcarОценок пока нет
- Health Effects of TobaccoДокумент6 страницHealth Effects of TobaccoStavan RathodОценок пока нет
- Tobacco Cessation in India: Labani Satyanarayana, Smita Asthana, Sumedha Mohan, Gourav PopliДокумент3 страницыTobacco Cessation in India: Labani Satyanarayana, Smita Asthana, Sumedha Mohan, Gourav PopliHakim ShaikhОценок пока нет
- Which Is Better in Smoking Using Vape oДокумент17 страницWhich Is Better in Smoking Using Vape oTata Duero LachicaОценок пока нет
- Fred Hsieh - To Vape or Not To VapeДокумент2 страницыFred Hsieh - To Vape or Not To VapeKalpikОценок пока нет
- E Cigarette AwarenessДокумент18 страницE Cigarette Awarenessr4adenОценок пока нет
- Thesis On e CigarettesДокумент8 страницThesis On e Cigarettessamanthajonessavannah100% (3)
- AN20201127-479 FinalДокумент7 страницAN20201127-479 FinalcinthiasОценок пока нет
- Literature Review On Tobacco UseДокумент7 страницLiterature Review On Tobacco Usefut0mipujeg3100% (1)
- Nihms 1506688 PDFДокумент29 страницNihms 1506688 PDFNicole Patricia Lawrence RiquelmeОценок пока нет
- Journal Reading DR Arief DAДокумент26 страницJournal Reading DR Arief DATaro RahmatiaОценок пока нет
- Jve 2 27Документ5 страницJve 2 27Taro RahmatiaОценок пока нет
- Arthropod BitesДокумент60 страницArthropod BitesTaro RahmatiaОценок пока нет
- Potensi Cabai Sebagai Anti-Aterosklerosis: Fakultas Kedokteran Universitas LampungДокумент6 страницPotensi Cabai Sebagai Anti-Aterosklerosis: Fakultas Kedokteran Universitas LampungTaro RahmatiaОценок пока нет
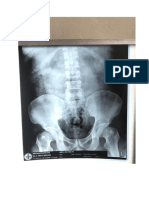
- Basic Musculoskeletal Radiologic InterpretationДокумент2 страницыBasic Musculoskeletal Radiologic InterpretationTaro RahmatiaОценок пока нет
- Adrenal Medulla: PheochromocytomaДокумент7 страницAdrenal Medulla: PheochromocytomaTaro RahmatiaОценок пока нет
- Corneal Degeneration: By-Shweta Santosh Maurya 2 Year B. Optometry Institute For Technology and ManagementДокумент43 страницыCorneal Degeneration: By-Shweta Santosh Maurya 2 Year B. Optometry Institute For Technology and ManagementTaro RahmatiaОценок пока нет
- Treatment Using Ethanolic Extract of Cocoa Beans)Документ5 страницTreatment Using Ethanolic Extract of Cocoa Beans)Hidayah HarahapОценок пока нет
- Herbicide and Fungicide Toxicology 2014Документ34 страницыHerbicide and Fungicide Toxicology 2014Taro RahmatiaОценок пока нет
- Namdaemun Market Location:: Exit From Line 4 - Hoehyeon StationДокумент3 страницыNamdaemun Market Location:: Exit From Line 4 - Hoehyeon StationTaro RahmatiaОценок пока нет
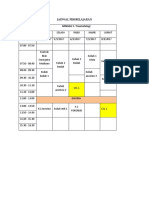
- Jadwal Minggu I Blok EmergencyДокумент1 страницаJadwal Minggu I Blok EmergencyTaro RahmatiaОценок пока нет
- Abdul RohimДокумент1 страницаAbdul RohimTaro RahmatiaОценок пока нет
- Ukuran BurnazinДокумент2 страницыUkuran BurnazinTaro RahmatiaОценок пока нет
- Qwertyuiop LatihannnnДокумент2 страницыQwertyuiop LatihannnnTaro RahmatiaОценок пока нет
- Niken ByssinosisДокумент23 страницыNiken ByssinosisTaro RahmatiaОценок пока нет
- Viral Skin InfectionДокумент23 страницыViral Skin InfectionTaro RahmatiaОценок пока нет
- Review Article: The Use of Stem Cells in Burn Wound Healing: A ReviewДокумент9 страницReview Article: The Use of Stem Cells in Burn Wound Healing: A ReviewTaro RahmatiaОценок пока нет
- Facial Fractures: Sylvia Aparicio Harvard Medical School Year IVДокумент0 страницFacial Fractures: Sylvia Aparicio Harvard Medical School Year IVRumah Kost Kontrakan AntapaniОценок пока нет
- 22 Varicella Pink BookДокумент24 страницы22 Varicella Pink BookMohamad Syaikhul IslamОценок пока нет
- Chronic Bronchitis in West Sweden A Matter of Smoking and Social ClassДокумент10 страницChronic Bronchitis in West Sweden A Matter of Smoking and Social ClassTaro RahmatiaОценок пока нет
- Pesticide PoisoningДокумент34 страницыPesticide PoisoningappealingashishОценок пока нет
- 22 Varicella Pink BookДокумент24 страницы22 Varicella Pink BookMohamad Syaikhul IslamОценок пока нет
- Pesticide Illness: Recognition, Diagnosis, ManagementДокумент31 страницаPesticide Illness: Recognition, Diagnosis, Managementكسلان اكتب اسميОценок пока нет
- Family Eco Map Bapak ZulkiДокумент1 страницаFamily Eco Map Bapak ZulkiTaro RahmatiaОценок пока нет
- Learning Objectives: Niken Rahmatia 1418011152Документ17 страницLearning Objectives: Niken Rahmatia 1418011152Taro RahmatiaОценок пока нет
- Facial Fractures: Sylvia Aparicio Harvard Medical School Year IVДокумент0 страницFacial Fractures: Sylvia Aparicio Harvard Medical School Year IVRumah Kost Kontrakan AntapaniОценок пока нет
- Penilaian Konsumsi Food Recall NikenДокумент3 страницыPenilaian Konsumsi Food Recall NikenTaro RahmatiaОценок пока нет
- Facial Fractures: Sylvia Aparicio Harvard Medical School Year IVДокумент0 страницFacial Fractures: Sylvia Aparicio Harvard Medical School Year IVRumah Kost Kontrakan AntapaniОценок пока нет
- Cushing SyndromeДокумент17 страницCushing SyndromeTaro RahmatiaОценок пока нет
- State Minimum Cigarette PricingДокумент16 страницState Minimum Cigarette Pricingrio boseОценок пока нет
- Malaysia - Docx by HanДокумент2 страницыMalaysia - Docx by HanHildegard HallasgoОценок пока нет
- SWOT & PESTEL ANALYSIS by Neha and SakshiДокумент21 страницаSWOT & PESTEL ANALYSIS by Neha and SakshisimranОценок пока нет
- Soal Um Bahasa InggrisДокумент9 страницSoal Um Bahasa Inggrismira stmikktbОценок пока нет
- Bat AbacoДокумент85 страницBat AbacoAgustynho Magimba100% (2)
- France's Disposable Vape Ban.Документ5 страницFrance's Disposable Vape Ban.Peter TừОценок пока нет
- Smoking EssayДокумент3 страницыSmoking EssayTrisha PangilinanОценок пока нет
- State of Tobacco Control 2020Документ140 страницState of Tobacco Control 2020Jon SinclairОценок пока нет
- Health Effects of SnusДокумент24 страницыHealth Effects of SnusDRChenMDОценок пока нет
- Extraction Nicotine Sulphate From Samples of Cigarettes: Chemistry Investigatory ProjectДокумент20 страницExtraction Nicotine Sulphate From Samples of Cigarettes: Chemistry Investigatory Projectchannel of dhyana75% (8)
- Alimentare - NealimentareДокумент6 страницAlimentare - NealimentareAndreeaОценок пока нет
- Smoking Among Juveniles: A StudyДокумент40 страницSmoking Among Juveniles: A StudySamTimalsina0% (1)
- Senior CapstoneДокумент6 страницSenior Capstoneapi-313278667Оценок пока нет
- Use of ITK in Plant ProtectionДокумент4 страницыUse of ITK in Plant ProtectionmramagroОценок пока нет
- Smoking - Health Risks: Reviewed byДокумент16 страницSmoking - Health Risks: Reviewed byNeranga Pravin SamaratungeОценок пока нет
- Biology Project File 12thДокумент22 страницыBiology Project File 12thNaveen SharmaОценок пока нет
- Soal Latihan B.INGGRISДокумент6 страницSoal Latihan B.INGGRISFatimah AzzahraОценок пока нет
- Vandolph Thesis2.3Документ254 страницыVandolph Thesis2.3Bernardo Villavicencio VanОценок пока нет
- Epi of Oral CancerДокумент294 страницыEpi of Oral CancerHansa KunduОценок пока нет
- Grade 8 HEALTH Q4 Lesson2 LM AlcoholДокумент29 страницGrade 8 HEALTH Q4 Lesson2 LM Alcoholleomille280% (10)
- The Altadis USA Cigar GuideДокумент10 страницThe Altadis USA Cigar Guideabbie normal100% (1)
- British American TobacooДокумент42 страницыBritish American TobacooShosta VlogОценок пока нет
- ELC501 - Article AnalysisДокумент3 страницыELC501 - Article AnalysisCt Bobot100% (1)
- Effects of SmokingДокумент8 страницEffects of Smokingrispher cherotichОценок пока нет
- 100% Final Last Term Paper On BATДокумент23 страницы100% Final Last Term Paper On BATMohammed HossainОценок пока нет
- Red Orchid - Best PracticesДокумент80 страницRed Orchid - Best PracticeslabiaernestoОценок пока нет
- Positive Effects Yung Nababawasan Ko Yung Pagyosi Ko Mahal Na Kailangan Magbawas Na Mas Pabor Namna Sa Sarili KoДокумент8 страницPositive Effects Yung Nababawasan Ko Yung Pagyosi Ko Mahal Na Kailangan Magbawas Na Mas Pabor Namna Sa Sarili KoAllain GuanlaoОценок пока нет
- Smoking Discursive EssayДокумент1 страницаSmoking Discursive EssayHaniel SohОценок пока нет
- Smokeless Tobacco: The Folklore and Social History of Snuffing, Sneezing, Dipping, and ChewingДокумент9 страницSmokeless Tobacco: The Folklore and Social History of Snuffing, Sneezing, Dipping, and Chewingruben14Оценок пока нет