Вам также может понравиться
- The Role of Doxycycline in The Management of CRSWPДокумент6 страницThe Role of Doxycycline in The Management of CRSWPLeonОценок пока нет
- Pediatric Chronic Sinusitis Diagnosis and ManagementДокумент10 страницPediatric Chronic Sinusitis Diagnosis and ManagementcaromoradОценок пока нет
- NebulizerДокумент4 страницыNebulizerHerryAsu-songkoОценок пока нет
- JCM 12 03605 v2Документ14 страницJCM 12 03605 v2IgnacioCortésFuentesОценок пока нет
- Predictive Value of Computed Tomography in The Recurrence of Chronic Rhinosinusitis With Nasal PolypsДокумент8 страницPredictive Value of Computed Tomography in The Recurrence of Chronic Rhinosinusitis With Nasal PolypsyohanasmjtОценок пока нет
- The Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyДокумент6 страницThe Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyArizkamhОценок пока нет
- Article Review Topical Corticosteroid Irrigations in Chronic RhinosinusitisДокумент7 страницArticle Review Topical Corticosteroid Irrigations in Chronic Rhinosinusitisgifar ihsanОценок пока нет
- Aair 11 482 PDFДокумент16 страницAair 11 482 PDFRegina Dwindarti DarostyОценок пока нет
- Ni Hms 765708Документ5 страницNi Hms 765708endahiuОценок пока нет
- HHS Public Access: Recent Evidence On The Management of BronchiolitisДокумент12 страницHHS Public Access: Recent Evidence On The Management of Bronchiolitissyahrizon thomasОценок пока нет
- Buonsenso Et Al-2018-Pediatric PulmonologyДокумент9 страницBuonsenso Et Al-2018-Pediatric Pulmonologywawa chenОценок пока нет
- Long-Term NIV Therapies in Children A Scoping ReviewДокумент11 страницLong-Term NIV Therapies in Children A Scoping ReviewMarcos ViDaОценок пока нет
- Chitsuthipakorn 2021Документ12 страницChitsuthipakorn 2021Diko KoestantyoОценок пока нет
- 834 3093 1 PB PDFДокумент5 страниц834 3093 1 PB PDFRegina Dwindarti DarostyОценок пока нет
- SepДокумент7 страницSepyuyuОценок пока нет
- Chronic Rhinosinusitis SteroidДокумент9 страницChronic Rhinosinusitis SteroidHan's ChristianОценок пока нет
- Articulos BronquiolitisДокумент18 страницArticulos BronquiolitisLaura López Del Castillo LalydelcaОценок пока нет
- Jurding RhinosinusistisДокумент26 страницJurding RhinosinusistisIhdina Hanifa Hasanal IbrahimОценок пока нет
- Implementation of An Evidence-Based NIRSДокумент10 страницImplementation of An Evidence-Based NIRSJhonny MarquezОценок пока нет
- Chronic Rhinosinusitis - An Overview: N.V Deepthi, U.K. Menon, K. MadhumitaДокумент6 страницChronic Rhinosinusitis - An Overview: N.V Deepthi, U.K. Menon, K. MadhumitaMilanisti22Оценок пока нет
- Journal Yolanda 2 - Trends in The Management of Peritonsillar Abscess in Children A Nationwide Population-Based Study in TaiwanДокумент6 страницJournal Yolanda 2 - Trends in The Management of Peritonsillar Abscess in Children A Nationwide Population-Based Study in TaiwanfrediОценок пока нет
- Oral Therapeutics For Rhinosinusitis With Nasal PoyposisДокумент10 страницOral Therapeutics For Rhinosinusitis With Nasal PoyposismilaОценок пока нет
- Kjped 57 479Документ5 страницKjped 57 479Vincent LivandyОценок пока нет
- Acute and Chronic Rhinosinusitis in Adults PSO-HNS 2016Документ12 страницAcute and Chronic Rhinosinusitis in Adults PSO-HNS 2016Angela TakedaОценок пока нет
- Jurnal Anak RirinДокумент10 страницJurnal Anak RirinDexter BluesОценок пока нет
- Efficacy and Safety of Normal Saline Instillation and PaediatricДокумент7 страницEfficacy and Safety of Normal Saline Instillation and PaediatricHanif Miftahul'Iza De'patheОценок пока нет
- 10.1007@s12070 014 0766 7Документ9 страниц10.1007@s12070 014 0766 7girish_s777Оценок пока нет
- Efficacy of Sinusitis UltrasoundДокумент7 страницEfficacy of Sinusitis UltrasoundYazid MultazamОценок пока нет
- The Use of Inhaled NaceДокумент7 страницThe Use of Inhaled NaceYondi Piter PapulungОценок пока нет
- Rhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral BronchiolitisДокумент7 страницRhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral Bronchiolitismariane bezerraОценок пока нет
- 2021 Factors Affecting Upper Airway Control ofNSAID Exacerbated Respiratory DiseaseДокумент10 страниц2021 Factors Affecting Upper Airway Control ofNSAID Exacerbated Respiratory Diseasexiongmao2389Оценок пока нет
- CRS 1Документ26 страницCRS 1Anita AmaliaОценок пока нет
- Technical Aspects of Treatment in Relation To Treatment OutcomeДокумент14 страницTechnical Aspects of Treatment in Relation To Treatment OutcomekochikaghochiОценок пока нет
- Ventilator Associated Pneumonia in ChildrenДокумент7 страницVentilator Associated Pneumonia in ChildrendarlingcarvajalduqueОценок пока нет
- Ent-Hns Clinical Practice Guidelines: Acute Bacterial RhinosinusitisДокумент11 страницEnt-Hns Clinical Practice Guidelines: Acute Bacterial RhinosinusitisClarice VillanuevaОценок пока нет
- Crs in ChildrenДокумент6 страницCrs in ChildrenSyafalikha DwizahraОценок пока нет
- Review Article: Chronic Rhinosinusitis in ChildrenДокумент6 страницReview Article: Chronic Rhinosinusitis in Childrenopi akbarОценок пока нет
- Treatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical SteroidsДокумент37 страницTreatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical SteroidsA.Оценок пока нет
- Grisaru SoenДокумент6 страницGrisaru SoenciciОценок пока нет
- Der Kay 2018Документ5 страницDer Kay 2018Giovanni HenryОценок пока нет
- Wright Et Al 2022 PDFДокумент9 страницWright Et Al 2022 PDFRadu CiprianОценок пока нет
- Genetic Deteriminat of Asthma Acute Therapy in ChildrenДокумент8 страницGenetic Deteriminat of Asthma Acute Therapy in ChildrenTiar OktavianОценок пока нет
- Gastroentritis AcuteДокумент10 страницGastroentritis AcuteYN Eyin VelinОценок пока нет
- Medi 94 E1642Документ8 страницMedi 94 E1642Rudolph GameОценок пока нет
- Recurrent Acute Rhinosinusitis Prevention by Azithromycin in Children With Nonallergic RhinitisДокумент7 страницRecurrent Acute Rhinosinusitis Prevention by Azithromycin in Children With Nonallergic RhinitisKeselek BakiakОценок пока нет
- Use of Indicators For Good Infection Control PracticeДокумент2 страницыUse of Indicators For Good Infection Control PracticeZY YanОценок пока нет
- 10 1016@j Ijporl 2020 110139Документ28 страниц10 1016@j Ijporl 2020 110139Gregoria choque floresОценок пока нет
- Patogenesis Polip NasalДокумент30 страницPatogenesis Polip NasalFelicia SutarliОценок пока нет
- A Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisДокумент11 страницA Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisErwin YanthoОценок пока нет
- J.jemermed.2020.10.011 Copy 2Документ6 страницJ.jemermed.2020.10.011 Copy 2Amaliah HakimОценок пока нет
- World Allergy Organization JournalДокумент8 страницWorld Allergy Organization JournalUlayya Ghina NabillaОценок пока нет
- Sitasi 2Документ7 страницSitasi 2Silvia ManurungОценок пока нет
- Medi 101 E29940Документ5 страницMedi 101 E29940Bella FebriantiОценок пока нет
- Causes and Outcomes of Respiratory Distress in NeonatesДокумент8 страницCauses and Outcomes of Respiratory Distress in NeonatesMohammad AlmuhaiminОценок пока нет
- PARS Reader's Digest - Feb 2013Документ12 страницPARS Reader's Digest - Feb 2013info8673Оценок пока нет
- Clinical Practice Guideline Adult Sinusi PDFДокумент32 страницыClinical Practice Guideline Adult Sinusi PDFفاطمه ستاری محمودیОценок пока нет
- E013796 FullДокумент12 страницE013796 FullNabilatur rodiyahОценок пока нет
- Epinephrine and Dexamethasone in Children With BronchiolitisДокумент11 страницEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisОценок пока нет
- Pierre Robin Sequence: An Evidence-Based Treatment ProposalДокумент7 страницPierre Robin Sequence: An Evidence-Based Treatment ProposalAdrian UmbriaОценок пока нет
- Eye ManualДокумент56 страницEye Manualbashir019Оценок пока нет
- Water Colored Splashes PowerPoint TemplateДокумент36 страницWater Colored Splashes PowerPoint TemplateAna Carmela DomingoОценок пока нет
- The Open Ophthalmology JournalДокумент5 страницThe Open Ophthalmology JournalFenny Duma SariОценок пока нет
- Abstrack Delibrate PracticeДокумент2 страницыAbstrack Delibrate PracticetopОценок пока нет
- Slit LampbiomicrosДокумент18 страницSlit LampbiomicrostopОценок пока нет
- Kertas Resep YudiДокумент1 страницаKertas Resep YuditopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Differential DiagnosesДокумент2 страницыPediatric Non-Hodgkin Lymphoma Differential DiagnosestopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologyДокумент11 страницPediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologytopОценок пока нет
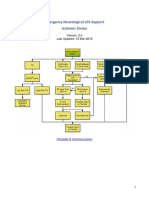
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Документ22 страницыEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationsДокумент15 страницPediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationstopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesДокумент5 страницPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopОценок пока нет
- Felting Fabulous Flowers Templates PDFДокумент3 страницыFelting Fabulous Flowers Templates PDFtop67% (3)
- Eye TraumaДокумент19 страницEye TraumatopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma MedicationДокумент8 страницPediatric Non-Hodgkin Lymphoma MedicationtopОценок пока нет
- Total ModalДокумент1 страницаTotal ModaltopОценок пока нет
- Role of PET/CT in Malignant Pediatric Lymphoma: Original ArticleДокумент11 страницRole of PET/CT in Malignant Pediatric Lymphoma: Original ArticletopОценок пока нет
- Pediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationДокумент3 страницыPediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationtopОценок пока нет
- CSS Jurnal DR IdratДокумент8 страницCSS Jurnal DR IdrattopОценок пока нет
- Jurnal Asli CSS - Khalida Khairunnisa - DR - ErniДокумент7 страницJurnal Asli CSS - Khalida Khairunnisa - DR - ErnitopОценок пока нет
- Role of Limited Whole-BodyДокумент9 страницRole of Limited Whole-BodytopОценок пока нет
- Poster Publik & Poster IlmiahДокумент10 страницPoster Publik & Poster Ilmiahtop100% (1)
- Materi Lat DesignДокумент27 страницMateri Lat DesigntopОценок пока нет
- Presentation 1Документ8 страницPresentation 1topОценок пока нет
- Radiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomasДокумент26 страницRadiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomastopОценок пока нет
- Guideline AoeДокумент25 страницGuideline AoetopОценок пока нет
- Antihistamines For Treating RhinosinusitisДокумент6 страницAntihistamines For Treating RhinosinusitistopОценок пока нет
- Antibiotics in Chronic RhinosinusitisДокумент5 страницAntibiotics in Chronic RhinosinusitistopОценок пока нет
- Role of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitisДокумент5 страницRole of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitistopОценок пока нет
- Anatomy and Physiology Nasal ObstructionДокумент13 страницAnatomy and Physiology Nasal ObstructiontopОценок пока нет
- Seven Golden Steps To Successful SearchingДокумент16 страницSeven Golden Steps To Successful SearchingDIANA PATRICIA MOLANO PEREZОценок пока нет
- Necessity of A Bed-Sensor in A Smart Digital HomeДокумент5 страницNecessity of A Bed-Sensor in A Smart Digital HomeEmilio CánepaОценок пока нет
- Using Google Scholar For Systematic ReviewДокумент6 страницUsing Google Scholar For Systematic ReviewCitra SuciptaОценок пока нет
- Co Q10Документ29 страницCo Q10ags375Оценок пока нет
- Tele NursingДокумент41 страницаTele Nursingcalvin100% (1)
- Responsiveness of Oral Health-Related Quality of Life Questionnaires To Dental Caries Interventions: Systematic Review and Meta-AnalysisДокумент14 страницResponsiveness of Oral Health-Related Quality of Life Questionnaires To Dental Caries Interventions: Systematic Review and Meta-AnalysisQuenntanaОценок пока нет
- Migrant Nurses Ausi Integrative ReviewДокумент7 страницMigrant Nurses Ausi Integrative ReviewBony Yunaria TanuОценок пока нет
- A Systematic Literature Review of Empirical Research in Lean and Six Sigma in HealthcareДокумент22 страницыA Systematic Literature Review of Empirical Research in Lean and Six Sigma in HealthcareDesign KIITОценок пока нет
- Making PubMed Searching SimpleДокумент11 страницMaking PubMed Searching SimpleGinna Paola Saavedra MartinezОценок пока нет
- Synopsis Presentation PPRVV-MSDДокумент9 страницSynopsis Presentation PPRVV-MSDDinesh M S PESU BTОценок пока нет
- An Estimation of The Number of Cells in The Human BodyДокумент11 страницAn Estimation of The Number of Cells in The Human BodysedilotОценок пока нет
- Pub MedДокумент4 страницыPub Medkailas ambadiОценок пока нет
- PICO Method SearchДокумент29 страницPICO Method SearchSamuel LionardiОценок пока нет
- Internet Cool Tools For Physicians PDFДокумент130 страницInternet Cool Tools For Physicians PDFRuxandra SimionОценок пока нет
- SUNRAY Review of Nutrition Research in AfricaДокумент33 страницыSUNRAY Review of Nutrition Research in AfricaAntoine Nabil ZakiОценок пока нет
- Comprehensiveness of PEDro, PTJ 2011Документ8 страницComprehensiveness of PEDro, PTJ 2011Ju ChangОценок пока нет
- Parasitology UST Resource ListДокумент3 страницыParasitology UST Resource ListJennifer HerediaОценок пока нет
- PewsДокумент21 страницаPewsrubertusedyОценок пока нет
- Effectiveness of Hospital Clowns For Symptom Management in Paediatrics: Systematic Review of Randomised and Non-Randomised Controlled TrialsДокумент13 страницEffectiveness of Hospital Clowns For Symptom Management in Paediatrics: Systematic Review of Randomised and Non-Randomised Controlled TrialsMarcela HincapiéОценок пока нет
- Ballard and Perry Et Al 2023Документ11 страницBallard and Perry Et Al 2023Ramiro LlanqueОценок пока нет
- Chapter 1 - Genetics-An Introduction PDFДокумент31 страницаChapter 1 - Genetics-An Introduction PDFEman Jandali100% (1)
- Overview of eRA Commons PDFДокумент94 страницыOverview of eRA Commons PDFcarlos1211805752Оценок пока нет
- Pubmed Boneadhesi SetДокумент1 021 страницаPubmed Boneadhesi SetVanshika JainОценок пока нет
- Introduction, Creating and ManagingДокумент75 страницIntroduction, Creating and ManagingSophia RusliОценок пока нет
- Case Write-Up 2Документ22 страницыCase Write-Up 2Syed TalhaОценок пока нет
- Neurosurgery Clinics of North America - Journal - ElsevierДокумент5 страницNeurosurgery Clinics of North America - Journal - ElsevierEwerson MatiaОценок пока нет
- Data in BriefДокумент3 страницыData in BriefDiretoria Sigma SocietyОценок пока нет
- Bioinformatics AssignmentДокумент10 страницBioinformatics AssignmentPriyanka KasturiaОценок пока нет
- 1.seema Sanghi, "The Handbook of Competency Mapping: Understanding, Designing and Implementing Competency Model in An Organization"Документ24 страницы1.seema Sanghi, "The Handbook of Competency Mapping: Understanding, Designing and Implementing Competency Model in An Organization"Arun AjithОценок пока нет
- Effect of Processing Method On The Dimensional Accuracy and Water Sorption of Acrylic Resin Dentures. - PubMed - NCBIДокумент2 страницыEffect of Processing Method On The Dimensional Accuracy and Water Sorption of Acrylic Resin Dentures. - PubMed - NCBIqwОценок пока нет