Вам также может понравиться
- Year in U.S. Occupational Health & Safety - 2019Документ72 страницыYear in U.S. Occupational Health & Safety - 2019Celeste Monforton100% (2)
- NAHB Et Al Lawsuit Challenging OSHA Recordkeeping Rule - Filed January 2017Документ31 страницаNAHB Et Al Lawsuit Challenging OSHA Recordkeeping Rule - Filed January 2017Celeste MonfortonОценок пока нет
- OHS Section 2021 Awards Program BookletДокумент12 страницOHS Section 2021 Awards Program BookletCeleste MonfortonОценок пока нет
- OHS Yearbook 2020Документ68 страницOHS Yearbook 2020Celeste MonfortonОценок пока нет
- CSTE - APHA - Public Citizen DC Circuit - OSHA Reporting Rule - July 2018Документ10 страницCSTE - APHA - Public Citizen DC Circuit - OSHA Reporting Rule - July 2018Celeste MonfortonОценок пока нет
- Hughson Heights CovenantsДокумент4 страницыHughson Heights CovenantsCeleste MonfortonОценок пока нет
- Garrett Brown - CSR Articles and Reports - Jan-Feb 2019Документ8 страницGarrett Brown - CSR Articles and Reports - Jan-Feb 2019Celeste MonfortonОценок пока нет
- More Pain Less Gain Report - Greater MN Worker CenterДокумент21 страницаMore Pain Less Gain Report - Greater MN Worker CenterCeleste MonfortonОценок пока нет
- Garrett - Brown CSR Articles and Reports - March-June 2019Документ14 страницGarrett - Brown CSR Articles and Reports - March-June 2019Celeste MonfortonОценок пока нет
- CDL Letter To Sanderson Farms - October - 1 - 2018Документ2 страницыCDL Letter To Sanderson Farms - October - 1 - 2018Celeste MonfortonОценок пока нет
- AOEC Work and Diabetes Expert Group - 2016Документ31 страницаAOEC Work and Diabetes Expert Group - 2016Celeste MonfortonОценок пока нет
- Baytown Lawsuit Against Mahoney May 2018Документ5 страницBaytown Lawsuit Against Mahoney May 2018Celeste MonfortonОценок пока нет
- Tree Care Industry Assoc - Letter To Cal - OSHA Wood Chippers - 2019Документ3 страницыTree Care Industry Assoc - Letter To Cal - OSHA Wood Chippers - 2019Celeste MonfortonОценок пока нет
- Fatality Investigation NY Wood Chipper FACE Report - 2018Документ10 страницFatality Investigation NY Wood Chipper FACE Report - 2018Celeste MonfortonОценок пока нет
- Year in US Occupational Health and Safety Fall 2017-Summer 2018Документ72 страницыYear in US Occupational Health and Safety Fall 2017-Summer 2018Celeste Monforton100% (1)
- OSHA Status Report 4 To District Court On Injury Reporting Reg - July 2018Документ3 страницыOSHA Status Report 4 To District Court On Injury Reporting Reg - July 2018Celeste MonfortonОценок пока нет
- TSAFF News Release Jul 1218Документ1 страницаTSAFF News Release Jul 1218Celeste MonfortonОценок пока нет
- Mahoney Favorable Decision WC Jan 2018Документ14 страницMahoney Favorable Decision WC Jan 2018Celeste MonfortonОценок пока нет
- TSAFF Letter To City of Baytown May 2018Документ1 страницаTSAFF Letter To City of Baytown May 2018Celeste MonfortonОценок пока нет
- Garrett Brown - CSR Articles & Reports - May-June 2018 - FINALДокумент11 страницGarrett Brown - CSR Articles & Reports - May-June 2018 - FINALCeleste MonfortonОценок пока нет
- Public Citizen - APHA - Motion To Intervene March 2017Документ4 страницыPublic Citizen - APHA - Motion To Intervene March 2017Celeste MonfortonОценок пока нет
- Mahoney Response City of Baytown May 31 2018Документ2 страницыMahoney Response City of Baytown May 31 2018Celeste MonfortonОценок пока нет
- Hal Rogers Et Al To MSHA - CPDM - Rock Dust Oct 2015Документ2 страницыHal Rogers Et Al To MSHA - CPDM - Rock Dust Oct 2015Celeste MonfortonОценок пока нет
- Jury Verdict - McKiver V Murphy BrownДокумент3 страницыJury Verdict - McKiver V Murphy BrownCeleste MonfortonОценок пока нет
- Aap Acog Apha - Tsca Cbi - Epa HQ Oppt 2017Документ8 страницAap Acog Apha - Tsca Cbi - Epa HQ Oppt 2017Celeste MonfortonОценок пока нет
- Chart 4 - March 2018 - Summary Chart - CSHOs - Garrett BrownДокумент3 страницыChart 4 - March 2018 - Summary Chart - CSHOs - Garrett BrownCeleste MonfortonОценок пока нет
- Chart 3 - DOSH Enforcement Staffing Summary Chart - August 2017 - Garrett BrownДокумент2 страницыChart 3 - DOSH Enforcement Staffing Summary Chart - August 2017 - Garrett BrownCeleste MonfortonОценок пока нет
- Chart 1 - Cal - OSHA Lost CSHO Positions - 2017-18 - Garrett BrownДокумент1 страницаChart 1 - Cal - OSHA Lost CSHO Positions - 2017-18 - Garrett BrownCeleste MonfortonОценок пока нет
- Chart 2 - Cal - OSHA Field Positions & Lost Resources - Garrett BrownДокумент2 страницыChart 2 - Cal - OSHA Field Positions & Lost Resources - Garrett BrownCeleste MonfortonОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Material Properties L2 Slides and NotesДокумент41 страницаMaterial Properties L2 Slides and NotesjohnОценок пока нет
- CCT AsqДокумент12 страницCCT Asqlcando100% (1)
- Difference Between OS1 and OS2 Single Mode Fiber Cable - Fiber Optic Cabling SolutionsДокумент2 страницыDifference Between OS1 and OS2 Single Mode Fiber Cable - Fiber Optic Cabling SolutionsDharma Teja TanetiОценок пока нет
- Tata Group's Global Expansion and Business StrategiesДокумент23 страницыTata Group's Global Expansion and Business Strategiesvgl tamizhОценок пока нет
- Compilation of CasesДокумент121 страницаCompilation of CasesMabelle ArellanoОценок пока нет
- Bob Duffy's 27 Years in Database Sector and Expertise in SQL Server, SSAS, and Data Platform ConsultingДокумент26 страницBob Duffy's 27 Years in Database Sector and Expertise in SQL Server, SSAS, and Data Platform ConsultingbrusselarОценок пока нет
- EWAIRДокумент1 страницаEWAIRKissy AndarzaОценок пока нет
- 6vortex 20166523361966663Документ4 страницы6vortex 20166523361966663Mieczysław MichalczewskiОценок пока нет
- Jurisdiction On Criminal Cases and PrinciplesДокумент6 страницJurisdiction On Criminal Cases and PrinciplesJeffrey Garcia IlaganОценок пока нет
- Engine Controls (Powertrain Management) - ALLDATA RepairДокумент4 страницыEngine Controls (Powertrain Management) - ALLDATA Repairmemo velascoОценок пока нет
- Lister LRM & SRM 1-2-3 Manual and Parts List - Lister - Canal WorldДокумент4 страницыLister LRM & SRM 1-2-3 Manual and Parts List - Lister - Canal Worldcountry boyОценок пока нет
- 158 Oesmer Vs Paraisa DevДокумент1 страница158 Oesmer Vs Paraisa DevRobelle Rizon100% (1)
- EFM2e, CH 03, SlidesДокумент36 страницEFM2e, CH 03, SlidesEricLiangtoОценок пока нет
- Diagnostic Information For Database Replay IssuesДокумент10 страницDiagnostic Information For Database Replay IssuesjjuniorlopesОценок пока нет
- SyllabusДокумент4 страницыSyllabusapi-105955784Оценок пока нет
- Collaboration Live User Manual - 453562037721a - en - US PDFДокумент32 страницыCollaboration Live User Manual - 453562037721a - en - US PDFIvan CvasniucОценок пока нет
- Mayor Byron Brown's 2019 State of The City SpeechДокумент19 страницMayor Byron Brown's 2019 State of The City SpeechMichael McAndrewОценок пока нет
- 28 Government Service Insurance System (GSIS) vs. Velasco, 834 SCRA 409, G.R. No. 196564 August 7, 2017Документ26 страниц28 Government Service Insurance System (GSIS) vs. Velasco, 834 SCRA 409, G.R. No. 196564 August 7, 2017ekangОценок пока нет
- 04 Dasmarinas Vs Reyes GR No 108229Документ2 страницы04 Dasmarinas Vs Reyes GR No 108229Victoria Melissa Cortejos PulidoОценок пока нет
- Photoshop Tools and Toolbar OverviewДокумент11 страницPhotoshop Tools and Toolbar OverviewMcheaven NojramОценок пока нет
- Fundamentals of Corporate Finance Canadian Canadian 8th Edition Ross Test Bank 1Документ36 страницFundamentals of Corporate Finance Canadian Canadian 8th Edition Ross Test Bank 1jillhernandezqortfpmndz100% (22)
- John GokongweiДокумент14 страницJohn GokongweiBela CraigОценок пока нет
- Growatt SPF3000TL-HVM (2020)Документ2 страницыGrowatt SPF3000TL-HVM (2020)RUNARUNОценок пока нет
- Emperger's pioneering composite columnsДокумент11 страницEmperger's pioneering composite columnsDishant PrajapatiОценок пока нет
- Sop EcuДокумент11 страницSop Ecuahmed saeedОценок пока нет
- Trinath Chigurupati, A095 576 649 (BIA Oct. 26, 2011)Документ13 страницTrinath Chigurupati, A095 576 649 (BIA Oct. 26, 2011)Immigrant & Refugee Appellate Center, LLCОценок пока нет
- Teleprotection Terminal InterfaceДокумент6 страницTeleprotection Terminal InterfaceHemanth Kumar MahadevaОценок пока нет
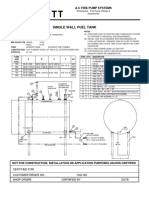
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsДокумент1 страницаSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoОценок пока нет
- Milton Hershey's Sweet StoryДокумент10 страницMilton Hershey's Sweet Storysharlene sandovalОценок пока нет
- Craft's Folder StructureДокумент2 страницыCraft's Folder StructureWowОценок пока нет