Вам также может понравиться
- Pulmonary Hypertension in Hemodialysis PatientsДокумент5 страницPulmonary Hypertension in Hemodialysis PatientsDr. Jatin GargОценок пока нет
- Complementary and Alternative Medical Lab Testing Part 4: VascularОт EverandComplementary and Alternative Medical Lab Testing Part 4: VascularОценок пока нет
- Pi Is 0272638616302645Документ9 страницPi Is 0272638616302645Eko PrasОценок пока нет
- Exercise Stress Test As An Antidote For Anxiety Ne PDFДокумент2 страницыExercise Stress Test As An Antidote For Anxiety Ne PDFmehrshad Farahpour Gp5Оценок пока нет
- Clinical Study: The Association Between Intradialytic Hypertension and Metabolic Disorders in End Stage Renal DiseaseДокумент9 страницClinical Study: The Association Between Intradialytic Hypertension and Metabolic Disorders in End Stage Renal Diseasecynthia nataliaОценок пока нет
- Special Situations: Intradialytic Hypertension/chronic Hypertension and Intradialytic HypotensionДокумент8 страницSpecial Situations: Intradialytic Hypertension/chronic Hypertension and Intradialytic HypotensionDavid SantosoОценок пока нет
- Hypertension in End-Stage Renal Disease: Eview RticleДокумент6 страницHypertension in End-Stage Renal Disease: Eview RticleGaema MiripОценок пока нет
- Predictors of Intradialytic Hypertension in Chronic End Stage Renal Dialysis Patients in A Tertiary Government Hospital in Davao CДокумент13 страницPredictors of Intradialytic Hypertension in Chronic End Stage Renal Dialysis Patients in A Tertiary Government Hospital in Davao CSari ChaerunisahОценок пока нет
- 1998 - Zager Et Al. - 'U' Curve Association of Blood Pressure and Mortality in Hemodialysis PatientsДокумент9 страниц1998 - Zager Et Al. - 'U' Curve Association of Blood Pressure and Mortality in Hemodialysis PatientsKTKL RSABОценок пока нет
- Intradialitic HypotensionДокумент7 страницIntradialitic HypotensionanitaОценок пока нет
- Intradialytic Hypertension in End Stage Renal Disease Patient: Prevalence and Clinical CharacteristicДокумент6 страницIntradialytic Hypertension in End Stage Renal Disease Patient: Prevalence and Clinical CharacteristicAmalОценок пока нет
- HipertensiДокумент37 страницHipertensiValentina PujiОценок пока нет
- Hipertension TranshemodialisisДокумент10 страницHipertension TranshemodialisisMonica HerreraОценок пока нет
- Comparison of Inflammatory Markers in HTNДокумент6 страницComparison of Inflammatory Markers in HTNDan JohnstonОценок пока нет
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionДокумент7 страницMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesОценок пока нет
- Cost Effectiveness and Resource AllocationДокумент7 страницCost Effectiveness and Resource AllocationSarah AmeliaОценок пока нет
- Hypertension Control, Apparent Treatment Resistance, and Outcomes in The Elderly Population With Chronic Kidney DiseaseДокумент12 страницHypertension Control, Apparent Treatment Resistance, and Outcomes in The Elderly Population With Chronic Kidney Diseasetika_876267153Оценок пока нет
- Hypertension Management in Transition From CKD A ERDS 2016Документ7 страницHypertension Management in Transition From CKD A ERDS 2016hemer hadyn calderon alvitesОценок пока нет
- Tgs Jurnal 1Документ7 страницTgs Jurnal 1suciОценок пока нет
- Diabetes Mellitus and Heart Failure 2017 The American Journal of MedicineДокумент11 страницDiabetes Mellitus and Heart Failure 2017 The American Journal of MedicineAlina PopaОценок пока нет
- JASN SDHD Paper 2005Документ11 страницJASN SDHD Paper 2005Carlos EghiОценок пока нет
- HTN Guidelines 1Документ12 страницHTN Guidelines 1lakshminivas PingaliОценок пока нет
- DNB Vol25 No2 142Документ7 страницDNB Vol25 No2 142Apsopela SandiveraОценок пока нет
- Go 2006Документ12 страницGo 2006my accountОценок пока нет
- Art Enfermedad Renal CronicaДокумент8 страницArt Enfermedad Renal CronicaLisset FernandezОценок пока нет
- Journal Reading PsikosisДокумент21 страницаJournal Reading PsikosisApsopela SandiveraОценок пока нет
- Research Article: Elevated Heparin-Induced Antibodies Are More Common in Diabetic Patients With Vascular DiseaseДокумент6 страницResearch Article: Elevated Heparin-Induced Antibodies Are More Common in Diabetic Patients With Vascular DiseaseAntony Boston MichaelОценок пока нет
- Arterial Hypertension e Clinical Trials Update 2021Документ11 страницArterial Hypertension e Clinical Trials Update 2021Dana MОценок пока нет
- Jurnal Int 2Документ14 страницJurnal Int 2rike aprilianaОценок пока нет
- Journal of Hypertension: Open Access: Hypertension-A Challenge To Modern MedicineДокумент2 страницыJournal of Hypertension: Open Access: Hypertension-A Challenge To Modern MedicineReiner ImranОценок пока нет
- Blood Pressure Management in Children On DialysisДокумент12 страницBlood Pressure Management in Children On DialysisinaОценок пока нет
- JCH 13 523Документ6 страницJCH 13 523Bunga dewanggi NugrohoОценок пока нет
- Ipri 36 1499588Документ6 страницIpri 36 1499588fani rudiyantiОценок пока нет
- CKD HT 3Документ8 страницCKD HT 3Peer TutorОценок пока нет
- Low Systemic Vascular ResistanceДокумент7 страницLow Systemic Vascular ResistanceMuhammad BadrushshalihОценок пока нет
- 228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Документ2 страницы228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Yulianty Saulina FransiscaОценок пока нет
- Nikhil Thesis AbstractДокумент28 страницNikhil Thesis AbstractNikhil KalasareОценок пока нет
- Cardiovascular Manifestations in Hyperthyroidism: Research ArticleДокумент7 страницCardiovascular Manifestations in Hyperthyroidism: Research Articlenurharyanti darmaningtyasОценок пока нет
- Management of Hypertension According To JNC 7: by Sandar Kyi, MDДокумент27 страницManagement of Hypertension According To JNC 7: by Sandar Kyi, MDDiana Da SilvaОценок пока нет
- Georgio Poul Ou 2010Документ16 страницGeorgio Poul Ou 2010ireneaureliaОценок пока нет
- Hubungan Neutrophyl To Lymphocyte Ratio Dengan Derajat Disfungsi Diastolik Pada Pasien HipertensiДокумент7 страницHubungan Neutrophyl To Lymphocyte Ratio Dengan Derajat Disfungsi Diastolik Pada Pasien HipertensiLutfhi ArshaldoОценок пока нет
- Epidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionДокумент8 страницEpidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionshaheershayanqaziОценок пока нет
- FCVM 09 860322Документ7 страницFCVM 09 860322Muh SutraОценок пока нет
- Management of HypertensionДокумент8 страницManagement of HypertensionJoe SingleОценок пока нет
- Association of Orthostatic Hypotension WithДокумент11 страницAssociation of Orthostatic Hypotension WithAulia Whiratama PutraОценок пока нет
- HHS Public Access: Pathophysiology and Implications of Intradialytic HypertensionДокумент13 страницHHS Public Access: Pathophysiology and Implications of Intradialytic HypertensionSari ChaerunisahОценок пока нет
- Prognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsДокумент11 страницPrognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDefriyan RamziОценок пока нет
- The Prognostic Role of Anemia in Heart Failure PatientsДокумент7 страницThe Prognostic Role of Anemia in Heart Failure PatientsAnonymous rprdjdFMNzОценок пока нет
- 2359 4802 Ijcs 34 04 0400.x98175Документ9 страниц2359 4802 Ijcs 34 04 0400.x98175leo leioaОценок пока нет
- Nota 2Документ8 страницNota 2Hector GuzmanОценок пока нет
- Hypertension ThesisДокумент31 страницаHypertension ThesisNavin AdhikariОценок пока нет
- Relation Between Vascular Risk Factors and Cognition at Age 75Документ7 страницRelation Between Vascular Risk Factors and Cognition at Age 75Fajar Rudy QimindraОценок пока нет
- Intradialytic Hypertension and The Association WitДокумент9 страницIntradialytic Hypertension and The Association WitMimi MuhammidaОценок пока нет
- Diagnosis Dan Tatalaksana Terkini Penyakit Jantung HipertensiДокумент8 страницDiagnosis Dan Tatalaksana Terkini Penyakit Jantung HipertensidhyassОценок пока нет
- The Dynamics of Haemostatic Parameters in Acute Psychotic Patients: A One-Year Prospective StudyДокумент8 страницThe Dynamics of Haemostatic Parameters in Acute Psychotic Patients: A One-Year Prospective StudyApsopela SandiveraОценок пока нет
- Transfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaДокумент41 страницаTransfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineОценок пока нет
- Plasma Lipids: Optimal Levels for HealthОт EverandPlasma Lipids: Optimal Levels for HealthAmerican Health FoundationОценок пока нет
- The Prevalence of ArterialДокумент8 страницThe Prevalence of ArterialInternational Medical PublisherОценок пока нет
- The Prevalence of Resistant Hypertension Among TypДокумент7 страницThe Prevalence of Resistant Hypertension Among TypProfessor Kamel AjlouniОценок пока нет
- Surviving Sepsis Hour 1 Bundle InfographДокумент1 страницаSurviving Sepsis Hour 1 Bundle InfographLaura PutriОценок пока нет
- Guidelines On Chronic Kidney Disease: (NKF K/Doqi)Документ32 страницыGuidelines On Chronic Kidney Disease: (NKF K/Doqi)Laura PutriОценок пока нет
- Morning Report Monday, 5 February 2018: Dept of Neurology G29Документ21 страницаMorning Report Monday, 5 February 2018: Dept of Neurology G29Laura PutriОценок пока нет
- Optical Prescription Details August 20XXДокумент3 страницыOptical Prescription Details August 20XXLaura PutriОценок пока нет
- Print FriendlyДокумент14 страницPrint FriendlyLaura PutriОценок пока нет
- Colloidsdengue 11 1 C RДокумент21 страницаColloidsdengue 11 1 C RLaura PutriОценок пока нет
- Protein Uri AДокумент12 страницProtein Uri ALaura PutriОценок пока нет
- 2005 Lipid Lowering DrugsДокумент22 страницы2005 Lipid Lowering DrugsLaura PutriОценок пока нет
- Penatalaksanaan: Amirah Muhammad AДокумент8 страницPenatalaksanaan: Amirah Muhammad ALaura PutriОценок пока нет
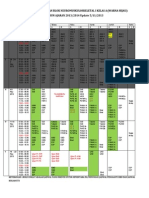
- Jadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Документ3 страницыJadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Laura PutriОценок пока нет
- 2121-Article Text-9456-1-10-20230131Документ8 страниц2121-Article Text-9456-1-10-20230131Çağdaş BaytarОценок пока нет
- Giant Bowen's Disease On The Face: Case Report and Review of The LiteratureДокумент4 страницыGiant Bowen's Disease On The Face: Case Report and Review of The LiteraturezoeyОценок пока нет
- Case Files PedsДокумент54 страницыCase Files PedsSam ZeezОценок пока нет
- ISMP Voluume 15 No 10 Oct 2017-NurseAdviseERR201710Документ4 страницыISMP Voluume 15 No 10 Oct 2017-NurseAdviseERR201710uss uusОценок пока нет
- Bhavishya Arogya ProspectusДокумент7 страницBhavishya Arogya ProspectusHarsh RajОценок пока нет
- .Au Files Dysbiosis ScoreДокумент2 страницы.Au Files Dysbiosis ScorekenetmartinОценок пока нет
- YH-5504SB ManualДокумент17 страницYH-5504SB ManualBill BrownОценок пока нет
- Ontogeny and Phylogeny of Immune SystemДокумент3 страницыOntogeny and Phylogeny of Immune SystemPM Basiloy - AloОценок пока нет
- CLUBFOOT GuidelineДокумент111 страницCLUBFOOT GuidelineNuhiat NahreenОценок пока нет
- Chapter 1: Introduction To Operative DentistryДокумент11 страницChapter 1: Introduction To Operative DentistryMariam AdnanОценок пока нет
- Disorders of The Adrenal Glands: Adrenal Cortical Adenoma and CarcinomaДокумент9 страницDisorders of The Adrenal Glands: Adrenal Cortical Adenoma and Carcinomahussain AltaherОценок пока нет
- Abdul Malik Hassim Lecturer DMA Management & Science UniversityДокумент21 страницаAbdul Malik Hassim Lecturer DMA Management & Science UniversitykimmgizelleОценок пока нет
- Effects of Advanced Carbohydrate Counting On Glucose Control and QolДокумент9 страницEffects of Advanced Carbohydrate Counting On Glucose Control and QollloplОценок пока нет
- TURBT FinalДокумент52 страницыTURBT FinalMuhammad RafiОценок пока нет
- Slide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Документ27 страницSlide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Maulia Wisda Era ChresiaОценок пока нет
- Contact Urticaria Syndrome: Occupational Aspects: Becky S. Li, Iris S. Ale, and Howard I. MaibachДокумент34 страницыContact Urticaria Syndrome: Occupational Aspects: Becky S. Li, Iris S. Ale, and Howard I. MaibachsaskiakonitaОценок пока нет
- Abortion in CattleДокумент6 страницAbortion in CattlekumarpujariОценок пока нет
- Hepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseДокумент12 страницHepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseSarah FaziraОценок пока нет
- Treating Lupus Using Tung PointstДокумент5 страницTreating Lupus Using Tung PointstOmer Binmahfooz100% (4)
- 8 Cns StimulantsДокумент46 страниц8 Cns StimulantslouradelОценок пока нет
- Acute Kidney InjuryДокумент49 страницAcute Kidney InjuryfikasywОценок пока нет
- Emergency Report Thursday:, October 07 2021Документ21 страницаEmergency Report Thursday:, October 07 2021Wilson WijayaОценок пока нет
- CBCT-Scan in DentistryДокумент24 страницыCBCT-Scan in DentistryBilly Sam80% (5)
- Cumulative Trauma DisordersДокумент70 страницCumulative Trauma DisordersBishal BistaОценок пока нет
- Giardia Duodenalis Affect Farmers Child Growth and DevelopmentДокумент2 страницыGiardia Duodenalis Affect Farmers Child Growth and DevelopmentAnitaОценок пока нет
- Frederick Griffith: Bacterial TransformationДокумент4 страницыFrederick Griffith: Bacterial Transformationrasha nada100% (1)
- Failure of Weaning:: According To The European Respiratory Society (ERS) Task ForceДокумент12 страницFailure of Weaning:: According To The European Respiratory Society (ERS) Task ForceAmr El Taher0% (1)
- Colchicine Drug Study For Gouty ArthritisДокумент3 страницыColchicine Drug Study For Gouty ArthritisLeslie PaguioОценок пока нет
- REAL in Nursing Journal (RNJ)Документ8 страницREAL in Nursing Journal (RNJ)Anonymous 8hlR5KvОценок пока нет
- Medical Terms and Definitons Commonly Used in MCNДокумент15 страницMedical Terms and Definitons Commonly Used in MCNjoemel gregoriОценок пока нет