Вам также может понравиться
- Uk MSДокумент6 страницUk MScode212Оценок пока нет
- Knee LectureДокумент35 страницKnee Lecturecode212Оценок пока нет
- Cell Organization in Epithelial Tissue 2013Документ71 страницаCell Organization in Epithelial Tissue 2013code212Оценок пока нет
- Osteogenesis ImperfectaДокумент27 страницOsteogenesis Imperfectacode212Оценок пока нет
- Management of Early-Onset ScoliosisДокумент5 страницManagement of Early-Onset Scoliosiscode212Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
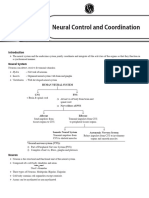
- CH - 21 Neural Control and Coordination DPP XI 26Документ26 страницCH - 21 Neural Control and Coordination DPP XI 26Riya MondalОценок пока нет
- Properties of Nerve FibersДокумент4 страницыProperties of Nerve FibersExamville.com100% (4)
- Chapter 1 Sensations and ResponsesДокумент8 страницChapter 1 Sensations and Responsessajith kumar VariathОценок пока нет
- Woreta Health Science and Business College Anatomy and Physiology of Nervous SystemДокумент55 страницWoreta Health Science and Business College Anatomy and Physiology of Nervous SystemEyachew TewabeОценок пока нет
- Multiple Sclerosis Medical-Surgical NursingДокумент5 страницMultiple Sclerosis Medical-Surgical NursingNoelyn BaluyanОценок пока нет
- 0521899427Документ591 страница0521899427osteonectin92% (13)
- Formal Examination Period: Session 1, June 2019Документ18 страницFormal Examination Period: Session 1, June 2019Lynstel NoronhaОценок пока нет
- Guillain-Barré Syndrome: I. Anatomical and Physiological BackgroundДокумент8 страницGuillain-Barré Syndrome: I. Anatomical and Physiological BackgroundSteve ColbertОценок пока нет
- Neural Control and Coordination Grade 11Документ30 страницNeural Control and Coordination Grade 11Dr. Remya RanjithОценок пока нет
- 2.2 Nerve Cell 2.2.1 The Main Parts of The Nerve CellДокумент4 страницы2.2 Nerve Cell 2.2.1 The Main Parts of The Nerve CellRoberta GabrielaОценок пока нет
- The Biological Perspective 1Документ18 страницThe Biological Perspective 1Radhey SurveОценок пока нет
- Thieme E-Journals - Seminars in Neurology - Full TextДокумент1 страницаThieme E-Journals - Seminars in Neurology - Full TextLeandro SebastianОценок пока нет
- Nerves, Neuroglia, and Neurotransmission: With Thad WilsonДокумент17 страницNerves, Neuroglia, and Neurotransmission: With Thad WilsonVathana SorОценок пока нет
- 652ee54506eb96001861e88a - ## - Neural Control and Coordination Part 1 Short NotesДокумент3 страницы652ee54506eb96001861e88a - ## - Neural Control and Coordination Part 1 Short Notesjai maa Durga aadi parashakti100% (1)
- 1.1 Fundamentals of The Nervous SystemДокумент18 страниц1.1 Fundamentals of The Nervous Systemno nameОценок пока нет
- PL3102 NotesДокумент8 страницPL3102 NotesKatriel HeartsBigbangОценок пока нет
- David S. Butler - Mobilisation of The Nervous System (1991, Churchill Livingstone) - Libgen - LiДокумент288 страницDavid S. Butler - Mobilisation of The Nervous System (1991, Churchill Livingstone) - Libgen - LiCetin Demircan100% (1)
- CH 7 Nervous Tissue PDFДокумент6 страницCH 7 Nervous Tissue PDFIbra TutorОценок пока нет
- Anatomy Chapter 14 Lecture-Nervous Tissue - Student VersionДокумент53 страницыAnatomy Chapter 14 Lecture-Nervous Tissue - Student VersionĐăng Khoa NguyễnОценок пока нет
- Acupuncture and MeridianДокумент8 страницAcupuncture and MeridianRichard SiahaanОценок пока нет
- St. Luke's College of Medicine - William H. Quasha Memorial: Block 1Документ9 страницSt. Luke's College of Medicine - William H. Quasha Memorial: Block 1Mavic Villanueva100% (1)
- Quiz PhysiologyДокумент46 страницQuiz PhysiologyMedShare78% (9)
- Differences Between Upper Limb and Lower Limb Choice Reaction TimeДокумент12 страницDifferences Between Upper Limb and Lower Limb Choice Reaction TimeKurt VogelОценок пока нет
- Multiple SclerosisДокумент13 страницMultiple SclerosisGEETA MOHANОценок пока нет
- 23 Nervous System: Encounter The PhenomenonДокумент5 страниц23 Nervous System: Encounter The PhenomenonJasmine AlsheikhОценок пока нет
- 11 - Histology Lecture - Structure of Nervous TissueДокумент50 страниц11 - Histology Lecture - Structure of Nervous TissueAMIRA HELAYEL100% (1)
- NeurodynamicsДокумент37 страницNeurodynamicsArielSchillaci100% (1)
- Unit 10 - Nervous SystemДокумент5 страницUnit 10 - Nervous Systemlola.konjevicОценок пока нет
- Física Do Corpo Humano: Prof. Adriano Mesquita Alencar Dep. Física Geral Instituto de Física Da USPДокумент31 страницаFísica Do Corpo Humano: Prof. Adriano Mesquita Alencar Dep. Física Geral Instituto de Física Da USPMariaSuzanaDiazОценок пока нет
- Test Bank For The Human Body in Health and Disease 7th Edition by PattonДокумент22 страницыTest Bank For The Human Body in Health and Disease 7th Edition by Pattonstephaniemendozagamobckjqf100% (15)