Вам также может понравиться
- Avoiding Common Problems Associated With Intravenous Fluid TherapyДокумент13 страницAvoiding Common Problems Associated With Intravenous Fluid TherapyDeepak AnОценок пока нет
- Perio PBM J FluidsДокумент6 страницPerio PBM J Fluidsjamiro345Оценок пока нет
- Adverse Effects of Crystalloid and Colloid Fluids: ReviewsДокумент6 страницAdverse Effects of Crystalloid and Colloid Fluids: Reviewsdhania husnainiОценок пока нет
- Perioperative Uid Management: Science, Art or Random Chaos?Документ5 страницPerioperative Uid Management: Science, Art or Random Chaos?pradeep danielОценок пока нет
- Could Patient Controlled Thirst Driven Fluid Administration 2018 British JouДокумент7 страницCould Patient Controlled Thirst Driven Fluid Administration 2018 British JouSeveNОценок пока нет
- Sepsis Fluidoterapia Revision Por EvidenciasДокумент4 страницыSepsis Fluidoterapia Revision Por EvidenciasGabriel Andrés Pérez BallenaОценок пока нет
- Br. J. Anaesth.-2002-Holte-622-32Документ11 страницBr. J. Anaesth.-2002-Holte-622-32Syauqi DarussalamОценок пока нет
- Fluid Overload Post OpДокумент11 страницFluid Overload Post OpAbdullah RababaahОценок пока нет
- Terapi CairanДокумент5 страницTerapi CairanZikry SitaniaОценок пока нет
- Minto. GDT and Monitoring Needs Within ERAS.Документ15 страницMinto. GDT and Monitoring Needs Within ERAS.kenjiОценок пока нет
- Perioperative Fluid Management: Zubin M. Bamboat, M.D. and Liliana Bordeianou, M.DДокумент6 страницPerioperative Fluid Management: Zubin M. Bamboat, M.D. and Liliana Bordeianou, M.DluluksОценок пока нет
- 00009Документ9 страниц00009Rezki Maulana DalimuntheОценок пока нет
- HemodialysisДокумент13 страницHemodialysisNova PututОценок пока нет
- Perioperativefluid Therapy: Denise Fantoni,, Andre C. ShihДокумент12 страницPerioperativefluid Therapy: Denise Fantoni,, Andre C. ShihDaniela BenavidesОценок пока нет
- Fluid Challenge RevisitedДокумент5 страницFluid Challenge RevisitedNinda DevitaОценок пока нет
- The Third Space Fact or FictionДокумент13 страницThe Third Space Fact or FictionShamini ShanmugalingamОценок пока нет
- 4 Phases of IV Fluid Therapy FinalДокумент29 страниц4 Phases of IV Fluid Therapy FinalLuqmanul Hakim Junaidden100% (1)
- Senam OtakДокумент15 страницSenam OtakDewi WulandariОценок пока нет
- Review Article Permissive Hypotensive Resuscitation - An Evolving Concept in TraumaДокумент3 страницыReview Article Permissive Hypotensive Resuscitation - An Evolving Concept in TraumareioctabianoОценок пока нет
- Articulo NefroДокумент11 страницArticulo NefroRoberto Lugo GuadarramaОценок пока нет
- Crystalloid and Colloid TherapyДокумент11 страницCrystalloid and Colloid TherapyAlexa UGОценок пока нет
- Fluid and Electrolyte Management For The Surgical PatientДокумент17 страницFluid and Electrolyte Management For The Surgical PatientFery López NavedaОценок пока нет
- Bundle 3 Hour Step4 FluidsДокумент4 страницыBundle 3 Hour Step4 FluidsgythrieОценок пока нет
- How To Avoid Flud OverloadДокумент7 страницHow To Avoid Flud OverloadEward Rod SalОценок пока нет
- Hemodialysis PDFДокумент14 страницHemodialysis PDFerikazoku moОценок пока нет
- Dry Weight in HemodialysisДокумент12 страницDry Weight in HemodialysisAnik PriyaniОценок пока нет
- Sja 12 311Документ7 страницSja 12 311edwuaroscarmillaangelesОценок пока нет
- Elia Jennifer Perioperative Fluid Management andДокумент19 страницElia Jennifer Perioperative Fluid Management andSiddhartha PalaciosОценок пока нет
- A Rational Approach To Perioperative Fluid ManagementДокумент18 страницA Rational Approach To Perioperative Fluid ManagementmarselamgeОценок пока нет
- Fluid and Hemodynamic Management in ERASДокумент13 страницFluid and Hemodynamic Management in ERASandreeaОценок пока нет
- Intravenous Fluid Therapy in Adults and ChildrenДокумент16 страницIntravenous Fluid Therapy in Adults and Childrenannisa hayati100% (1)
- Pi Is 0039610912000163Документ17 страницPi Is 0039610912000163Hend Al-DreesОценок пока нет
- Evidence and Triggers For The Transfusion of Blood and Blood ProductsДокумент9 страницEvidence and Triggers For The Transfusion of Blood and Blood Productscahaya tinggiОценок пока нет
- Protocolizedresuscitation Ofburnpatients: Leopoldo C. Cancio,, Jose Salinas,, George C. KramerДокумент12 страницProtocolizedresuscitation Ofburnpatients: Leopoldo C. Cancio,, Jose Salinas,, George C. KramerDitha FadhilaОценок пока нет
- Fluidtherapyinlung Disease: Elizabeth Rozanski,, Alex LynchДокумент10 страницFluidtherapyinlung Disease: Elizabeth Rozanski,, Alex LynchrianperoОценок пока нет
- Hypervolemia Increases Release of Atrial Natriuretic Peptide and Shedding of The Endothelial GlycocalyxДокумент8 страницHypervolemia Increases Release of Atrial Natriuretic Peptide and Shedding of The Endothelial GlycocalyxbayanganОценок пока нет
- Effect of Intraoperative Fluid Management On Outcome After Intraabdominal SurgeryДокумент8 страницEffect of Intraoperative Fluid Management On Outcome After Intraabdominal Surgeryade_liaОценок пока нет
- Managing Obstetric HemorrhageДокумент11 страницManaging Obstetric HemorrhageClara VerlinaОценок пока нет
- Hemorrhagic Shock in The Pediatric Patient - New Therapies and PracticeДокумент6 страницHemorrhagic Shock in The Pediatric Patient - New Therapies and Practicefitrah fajrianiОценок пока нет
- Fluid & Blood Therapy Key ConceptsДокумент31 страницаFluid & Blood Therapy Key ConceptsMohammad Pino HakimОценок пока нет
- Shock Hipo 3Документ11 страницShock Hipo 3AdeliaОценок пока нет
- Intraoperative Fluid Management in Open Gastro-Intestinal Surgery: Goal-Directed Versus RestrictiveДокумент7 страницIntraoperative Fluid Management in Open Gastro-Intestinal Surgery: Goal-Directed Versus Restrictiveade_liaОценок пока нет
- Dose and Type of Crystalloid Fluid Therapy in Adult Hospitalized PatientsДокумент10 страницDose and Type of Crystalloid Fluid Therapy in Adult Hospitalized PatientsAnis Rita PratiwiОценок пока нет
- Massive Transfusion ProtocolДокумент11 страницMassive Transfusion ProtocolAlaa Abdelmoaty OmranОценок пока нет
- Seminars 2019 PDFДокумент200 страницSeminars 2019 PDFpaingmyintОценок пока нет
- Fluid Use 24 11 CorregidoДокумент10 страницFluid Use 24 11 CorregidoCarlos Enrique Almonte MarínОценок пока нет
- DrHSMurthy HiPECДокумент11 страницDrHSMurthy HiPECReddyОценок пока нет
- Blood Conservation in Pediatric Cardiac SurgeryДокумент5 страницBlood Conservation in Pediatric Cardiac Surgerymohanakrishna007Оценок пока нет
- Noninvasive Monitoring 2016Документ6 страницNoninvasive Monitoring 2016Maria LaiaОценок пока нет
- BloodTransfus2010_Vol8_Issue_2_082-088_122-09Документ7 страницBloodTransfus2010_Vol8_Issue_2_082-088_122-09jesyoltzinОценок пока нет
- Management of HemorrhageДокумент11 страницManagement of Hemorrhagemerin sunilОценок пока нет
- 2020 MONITORING COHERENCE Hemodynamic Coherence and The Rationale For MONITORING PDFДокумент13 страниц2020 MONITORING COHERENCE Hemodynamic Coherence and The Rationale For MONITORING PDFLUIS CARLOS MAYAОценок пока нет
- Fluid Resuscitation in Trauma Patients What Should We KnowДокумент7 страницFluid Resuscitation in Trauma Patients What Should We Knowekaseptiani312Оценок пока нет
- 7: Effective Transfusion in Surgery and Critical CareДокумент16 страниц7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomОценок пока нет
- Intraoperative Fluids: How Much Is Too Much?: Editor's Key PointsДокумент11 страницIntraoperative Fluids: How Much Is Too Much?: Editor's Key PointsRicardoОценок пока нет
- 9) Fluid and HemodynamicsДокумент13 страниц9) Fluid and HemodynamicsPablo MartinezОценок пока нет
- Dapus 3Документ7 страницDapus 3Dhea NadhilaОценок пока нет
- Manejo Del ResangradoДокумент13 страницManejo Del ResangradoRudy J CoradoОценок пока нет
- Management of Hemostasis and Coagulopathies for Surgical and Critically Ill Patients: An Evidence-Based ApproachОт EverandManagement of Hemostasis and Coagulopathies for Surgical and Critically Ill Patients: An Evidence-Based ApproachРейтинг: 5 из 5 звезд5/5 (1)
- The Effects of Pre Anesthetic, Single-Dose Dexmedetomidine On Ion Hemodynamic and Cardiovascular ParametersДокумент6 страницThe Effects of Pre Anesthetic, Single-Dose Dexmedetomidine On Ion Hemodynamic and Cardiovascular ParametersjcaegОценок пока нет
- Pre MedicationДокумент4 страницыPre MedicationjcaegОценок пока нет
- Pharmacology of Sedative Analgesic Agents DexmedetomidineДокумент19 страницPharmacology of Sedative Analgesic Agents DexmedetomidinejcaegОценок пока нет
- Monitoring Endocrine FunctionДокумент10 страницMonitoring Endocrine FunctionjcaegОценок пока нет
- Perioperative Fluid TherapyДокумент3 страницыPerioperative Fluid Therapyjcaeg100% (1)
- Hypothalamic - Pituitary - Adrenal FuntionДокумент4 страницыHypothalamic - Pituitary - Adrenal FuntionjcaegОценок пока нет
- Hormonal and Metabolic Responses To TraumaДокумент3 страницыHormonal and Metabolic Responses To TraumajcaegОценок пока нет
- Dexmedetomidine As Sole Sedative For Awake Ion in Management of The Critical AirwayДокумент4 страницыDexmedetomidine As Sole Sedative For Awake Ion in Management of The Critical AirwayjcaegОценок пока нет
- Anaesthesia For NeurosurgeryДокумент4 страницыAnaesthesia For NeurosurgeryjcaegОценок пока нет
- Clinical Aspects of EndocrinologyДокумент4 страницыClinical Aspects of EndocrinologyjcaegОценок пока нет
- Pre MedicationДокумент4 страницыPre MedicationjcaegОценок пока нет
- Neonatal ResuscitationДокумент5 страницNeonatal Resuscitationabdirahiim ahmedОценок пока нет
- Measuring Central Venous Pressure FinalДокумент6 страницMeasuring Central Venous Pressure FinalPatel HimaniОценок пока нет
- Tracheostomy E Tool 1Документ3 страницыTracheostomy E Tool 1Dennis MagdaraogОценок пока нет
- 2018-Academic Emergency MedicineДокумент278 страниц2018-Academic Emergency MedicinederrickОценок пока нет
- Osce Pro III Trial AnswerДокумент69 страницOsce Pro III Trial AnswerDr Onn Azli Puade100% (3)
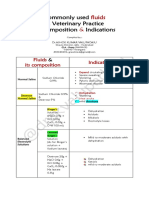
- Common IV Fluids at Composition & IndicationsДокумент2 страницыCommon IV Fluids at Composition & IndicationsNilesh SuryawanshiОценок пока нет
- Leunase InjДокумент14 страницLeunase InjLiaWahyuniОценок пока нет
- Remdesivir Injection 100 MG Pharmacy Manual v2 March 2020Документ15 страницRemdesivir Injection 100 MG Pharmacy Manual v2 March 2020Gurpreet SinghОценок пока нет
- Sherydan Urbanek - Chem1701 Case StudyДокумент9 страницSherydan Urbanek - Chem1701 Case Studyapi-491453185Оценок пока нет
- Week 3 - Preparation of Red Blood Cell SuspensionДокумент9 страницWeek 3 - Preparation of Red Blood Cell SuspensionAldwin CabanbanОценок пока нет
- Instillation of Normal Saline in Endotracheal SuctioningДокумент2 страницыInstillation of Normal Saline in Endotracheal SuctioningChiyouaLoverz Tharaztic JRsОценок пока нет
- Ethiopia's Emergency Medicines ListДокумент38 страницEthiopia's Emergency Medicines ListMichael Silva100% (3)
- Hyperglycaemic Emergencies Inpatient Draft-1-3Документ13 страницHyperglycaemic Emergencies Inpatient Draft-1-3Cik JaaОценок пока нет
- Fibrin GlueДокумент3 страницыFibrin Glueاحمد مفرح سالمОценок пока нет
- ACUTE GASTROENTERITIS GUIDEДокумент54 страницыACUTE GASTROENTERITIS GUIDEVincent LaranjoОценок пока нет
- Management DeshidratationДокумент15 страницManagement DeshidratationDani G CeñalОценок пока нет
- Isotonic, Hypotonic, and Hypertonic IV Fluid Solution: Isotonic Solutions: Contains Approximately The SameДокумент1 страницаIsotonic, Hypotonic, and Hypertonic IV Fluid Solution: Isotonic Solutions: Contains Approximately The SamemimОценок пока нет
- IV Solution Cheat Sheet: A Quick Reference Guide On The Different Intravenous SolutionsДокумент2 страницыIV Solution Cheat Sheet: A Quick Reference Guide On The Different Intravenous SolutionsNicole Xyza JunsayОценок пока нет
- Feline Update Spring 2010Документ12 страницFeline Update Spring 2010ابراهيم عبدالله100% (1)
- Treatment of Hypernatremia in Adults - UpToDateДокумент35 страницTreatment of Hypernatremia in Adults - UpToDateJuLio Czar Carmona100% (1)
- Fluids and Electrolytes: Epidemiology/PathophysiologyДокумент27 страницFluids and Electrolytes: Epidemiology/PathophysiologyManna YankiОценок пока нет
- Major Intracellular and Extracellular IonsДокумент20 страницMajor Intracellular and Extracellular IonsTricia RestriveraОценок пока нет
- Endocrine Test Protocols: Medical Investigation Facility Endocrinology & Diabetes UnitДокумент24 страницыEndocrine Test Protocols: Medical Investigation Facility Endocrinology & Diabetes UnitMulyono Aba Athiya100% (2)
- 5 IV Therapy TransesДокумент9 страниц5 IV Therapy TransesKeana Dacayana100% (1)
- Nursing Care Plan For "Fluid and Electrolyte Imbalances"Документ37 страницNursing Care Plan For "Fluid and Electrolyte Imbalances"jhonroks90% (50)
- Pharmacy Technician Medication Orders GuideДокумент31 страницаPharmacy Technician Medication Orders GuideAlan Hao92% (12)
- Overview of The Treatment of HyponatremiaДокумент19 страницOverview of The Treatment of HyponatremiaCamila Francisca Manques MacuadaОценок пока нет
- Pocket Guide to Managing Diabetes in ChildrenДокумент60 страницPocket Guide to Managing Diabetes in ChildrenAndreea Katy100% (1)
- Dose Calculation: 1) Preparation of 1% V/V Tween 80 in Saline: (For 150 ML)Документ3 страницыDose Calculation: 1) Preparation of 1% V/V Tween 80 in Saline: (For 150 ML)Apurba Sarker ApuОценок пока нет
- Intelligent Saline Monitoring SystemДокумент3 страницыIntelligent Saline Monitoring SystemAnonymous izrFWiQОценок пока нет