Вам также может понравиться
- DLL in Math (July 10-14, 2017)Документ7 страницDLL in Math (July 10-14, 2017)Florecita CabañogОценок пока нет
- Detailed Lesson Plan (Mixture Characteristics)Документ8 страницDetailed Lesson Plan (Mixture Characteristics)Kevin De GuzmanОценок пока нет
- Matrix of Curriculum Standards (Competencies), With Corresponding Recommended Flexible Learning Delivery Mode and Materials Per Grading PeriodДокумент3 страницыMatrix of Curriculum Standards (Competencies), With Corresponding Recommended Flexible Learning Delivery Mode and Materials Per Grading PeriodEvan Maagad LutchaОценок пока нет
- Music Melcs Grade 1Документ3 страницыMusic Melcs Grade 1Vincent Pol AsioОценок пока нет
- Attendance Sheet ELLN LACДокумент6 страницAttendance Sheet ELLN LACpina2014Оценок пока нет
- DLL - Mapeh 6 - Q3 - W4Документ4 страницыDLL - Mapeh 6 - Q3 - W4Lesli Daryl Antolin SanMateo100% (1)
- DLL Mapeh 3Документ41 страницаDLL Mapeh 3MarxPascualBlancoОценок пока нет
- Mapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesДокумент8 страницMapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesNICOLE ALANA100% (1)
- Describes The Nature and Background of 2. Undertakes Physical Activity and PhysicalДокумент2 страницыDescribes The Nature and Background of 2. Undertakes Physical Activity and PhysicalSerLem WellОценок пока нет
- Mapeh DLL Week 4Документ4 страницыMapeh DLL Week 4Darwin SolanoyОценок пока нет
- MATH 5 DLL - Q1 - Visualizes Multiplication of Fractions Using ModelsДокумент5 страницMATH 5 DLL - Q1 - Visualizes Multiplication of Fractions Using ModelsMary Ann Pontillas100% (1)
- The Nature, Structure, and Content of The K To 12 Science CurriculumДокумент23 страницыThe Nature, Structure, and Content of The K To 12 Science CurriculumJhenn Mhen Yhon0% (1)
- K To 12 Sped Transition Curriculum Functional Academics DescriptionДокумент14 страницK To 12 Sped Transition Curriculum Functional Academics DescriptionClaudineRamosSupnet100% (2)
- Activity 10 - Developing An Effective Classroom Science ProgramДокумент2 страницыActivity 10 - Developing An Effective Classroom Science ProgramAdrian NenengОценок пока нет
- Lesson Plan in Science 6Документ9 страницLesson Plan in Science 6Alexander Pamulagan BaternaОценок пока нет
- RUBRIC Sa Paggawa NG Color Wheel Arts Ptask 3Документ2 страницыRUBRIC Sa Paggawa NG Color Wheel Arts Ptask 3kayerencaole0% (1)
- q1 Test in Science Grade 4 Two ColumnДокумент4 страницыq1 Test in Science Grade 4 Two ColumnMagnolia Nicandro AutencioОценок пока нет
- LMC (Grade 3)Документ11 страницLMC (Grade 3)Renge TañaОценок пока нет
- Secondperiodicaltestenglishgrade3 141011072305 Conversion Gate02 PDFДокумент5 страницSecondperiodicaltestenglishgrade3 141011072305 Conversion Gate02 PDFelsa catacutanОценок пока нет
- Lesson Exemplar in MAPEH VI Elements and Principles Applied in Comic ArtДокумент5 страницLesson Exemplar in MAPEH VI Elements and Principles Applied in Comic Artmetalhead_025Оценок пока нет
- Grade 6 DLL SCIENCE 6 Q3 Week 5Документ7 страницGrade 6 DLL SCIENCE 6 Q3 Week 5Mark neil a. GalutОценок пока нет
- Math PT and Tos 4th GradingДокумент4 страницыMath PT and Tos 4th GradingSharizzaSumbing100% (1)
- Budget of Work in Music, Arts, Physical Education, Health (Mapeh) 2Документ5 страницBudget of Work in Music, Arts, Physical Education, Health (Mapeh) 2KeyrenОценок пока нет
- Understanding Personal Health IssuesДокумент5 страницUnderstanding Personal Health IssuesCathlyn Joy GanadenОценок пока нет
- Competency 8.1 WK4 Day1Документ3 страницыCompetency 8.1 WK4 Day1Rainel ManosОценок пока нет
- Least Learned MAPEH Competencies Obillo ElementaryДокумент4 страницыLeast Learned MAPEH Competencies Obillo ElementaryRaulJunioRamos100% (1)
- Electron and Quantum TheoryДокумент14 страницElectron and Quantum TheoryasОценок пока нет
- DLL - Science 6 - Q2 - W6Документ10 страницDLL - Science 6 - Q2 - W6Geoffrey Tolentino-UnidaОценок пока нет
- Lesson Exemplar in Science 1 (Melc)Документ6 страницLesson Exemplar in Science 1 (Melc)jal bayaniОценок пока нет
- The Four-Pronged Approach To Teaching ReadingДокумент15 страницThe Four-Pronged Approach To Teaching ReadingJonuel Escolano100% (2)
- Grade 1 Arts: Exploring Lines, Shapes, Colors and Textures Through Drawing, Painting and PrintmakingДокумент87 страницGrade 1 Arts: Exploring Lines, Shapes, Colors and Textures Through Drawing, Painting and Printmakingjanwill ocampoОценок пока нет
- Department of Education: Narrative Report in Helping Struggling ReadersДокумент3 страницыDepartment of Education: Narrative Report in Helping Struggling ReadersAdelaida BobadillaОценок пока нет
- English Lesson Exemplar Cot 2Документ3 страницыEnglish Lesson Exemplar Cot 2Fred Ryan Canoy DeañoОценок пока нет
- Lesson LogДокумент13 страницLesson LogJill Ann LogmaoОценок пока нет
- Teaching Strategies in PEДокумент58 страницTeaching Strategies in PEGilbert LopezОценок пока нет
- Elementary school lesson plan on number sequences and patternsДокумент2 страницыElementary school lesson plan on number sequences and patternsFrancia Yalung Jimenez Galang100% (1)
- MUSIC MELCs Grade 3 PDFДокумент4 страницыMUSIC MELCs Grade 3 PDFMarcelina EllarОценок пока нет
- Kinder 2Документ2 страницыKinder 2api-266484104Оценок пока нет
- Subtask in MTB 2 Ist CG 2019 2020Документ4 страницыSubtask in MTB 2 Ist CG 2019 2020Ginalyn Matildo Afable100% (1)
- DLL - Science 6 - Q2 - W1Документ10 страницDLL - Science 6 - Q2 - W1Erika ShoppeeОценок пока нет
- DETAILED LESSON PLAN IN MATHEMATICS IV - Docx (Identifying and Describing Different Quadrilaterals)Документ5 страницDETAILED LESSON PLAN IN MATHEMATICS IV - Docx (Identifying and Describing Different Quadrilaterals)KREZELLE JANE MIGUELОценок пока нет
- Exploring Useful and Harmful Materials in Science (Grade 5)Документ5 страницExploring Useful and Harmful Materials in Science (Grade 5)timothy castilloОценок пока нет
- D. Issues in Teaching and Learning Multicultural Literacy in The PHДокумент9 страницD. Issues in Teaching and Learning Multicultural Literacy in The PHClind Angel ConcepcionОценок пока нет
- Final Lesson Plan Multigrade AMOMA JOY LYN SДокумент9 страницFinal Lesson Plan Multigrade AMOMA JOY LYN SDencie CabarlesОценок пока нет
- Health 6 Q1 Mod2 Self-Management-Skills v2Документ22 страницыHealth 6 Q1 Mod2 Self-Management-Skills v2Gessle GamirОценок пока нет
- Table of Specification: First Grading (Mapeh 7)Документ1 страницаTable of Specification: First Grading (Mapeh 7)Mark Jim ToreroОценок пока нет
- K To 12 Curriculum Guide: Mother TongueДокумент149 страницK To 12 Curriculum Guide: Mother TongueBinsent12Оценок пока нет
- Forced Motion ForcesДокумент25 страницForced Motion ForcesLorieОценок пока нет
- Learning Plan in MAPEH Week 2 (3rd Quarter)Документ9 страницLearning Plan in MAPEH Week 2 (3rd Quarter)june kathleen v. bautistaОценок пока нет
- DLP in Mathematics 4 Quarter 4Документ11 страницDLP in Mathematics 4 Quarter 4Lorina GallegoОценок пока нет
- Daily English Lesson Focuses on Story ComprehensionДокумент5 страницDaily English Lesson Focuses on Story Comprehensionjoangeg5Оценок пока нет
- Separating Mixtures DLPДокумент5 страницSeparating Mixtures DLPEllize Mariae0% (1)
- Least Learned Skills Grades2 3 4 QuarterДокумент2 страницыLeast Learned Skills Grades2 3 4 QuarterGeneven Hermosa OlasimanОценок пока нет
- Bullying 3Документ4 страницыBullying 3Regine VelascoОценок пока нет
- Mapeh (Health) : Pamamahala NG Mga Isyung Kaakibat NG Pagdadalaga at PagbibinataДокумент9 страницMapeh (Health) : Pamamahala NG Mga Isyung Kaakibat NG Pagdadalaga at PagbibinataSally DelfinОценок пока нет
- Grades 1 to 12 School ecosystem interactionsДокумент12 страницGrades 1 to 12 School ecosystem interactionsRhoda Pagtalunan Lemorinas75% (4)
- Division Memorandum No. 048, S. 2024Документ12 страницDivision Memorandum No. 048, S. 2024purplegraphics24Оценок пока нет
- QUARTER 1 - English Grade 3Документ173 страницыQUARTER 1 - English Grade 3Jo MeiОценок пока нет
- Healthy Mind and Body: Mental, Physical WellnessДокумент3 страницыHealthy Mind and Body: Mental, Physical WellnessTin TinОценок пока нет
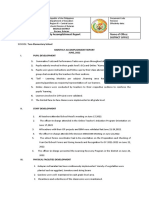
- Monthly Accomplishment Report District OfficeДокумент2 страницыMonthly Accomplishment Report District OfficeMaria Victoria Malonzo AcostaОценок пока нет
- Request Form137Документ1 страницаRequest Form137Maria Victoria Malonzo AcostaОценок пока нет
- 2019jul22rhia1111pds2018PDS - REVISEDДокумент14 страниц2019jul22rhia1111pds2018PDS - REVISEDMaria Victoria Malonzo AcostaОценок пока нет
- BlankSHN Form 021 District Nutritional Status ReportДокумент1 страницаBlankSHN Form 021 District Nutritional Status ReportMaria Victoria Malonzo AcostaОценок пока нет
- Criiria. CHIFdocxДокумент1 страницаCriiria. CHIFdocxMaria Victoria Malonzo AcostaОценок пока нет
- Improve Reading Fluency with Repeated ReadingДокумент7 страницImprove Reading Fluency with Repeated ReadingMaria Victoria Malonzo AcostaОценок пока нет
- The Analytic Method of Teaching - RyanДокумент25 страницThe Analytic Method of Teaching - RyanMaria Victoria Malonzo AcostaОценок пока нет
- Table of Specification: Learning CompetenciesДокумент2 страницыTable of Specification: Learning CompetenciesChristian Ace Dequito RomeroОценок пока нет
- Low Carbohydrate DietДокумент38 страницLow Carbohydrate DietEsther SiraitОценок пока нет
- Diesel Dad 100 - v1.0Документ20 страницDiesel Dad 100 - v1.0Vikas Reddy100% (2)
- High Intensity Interval Training HIIT Program PDFДокумент2 страницыHigh Intensity Interval Training HIIT Program PDFNikolaОценок пока нет
- Dance Aerobics Workout for All AgesДокумент6 страницDance Aerobics Workout for All AgesPratima ShrivastavaОценок пока нет
- RA 8976 or The Food Fortification LawДокумент4 страницыRA 8976 or The Food Fortification LawLovely Rose SoriaoОценок пока нет
- Health - Related Physical Fitness Refers To The Overall Well Being of An Individual. Read and Understand Each of ThemДокумент7 страницHealth - Related Physical Fitness Refers To The Overall Well Being of An Individual. Read and Understand Each of ThemSuper AmazingОценок пока нет
- Barangay Nutrition Action Plan for 2023Документ1 страницаBarangay Nutrition Action Plan for 2023Poblacion Zone 1 Del Gallego Camarines SurОценок пока нет
- Insanity Deluxe Workout Calendar Month 1 & 2Документ1 страницаInsanity Deluxe Workout Calendar Month 1 & 2Anonymous sTnEkqy4Оценок пока нет
- Jennifer Boisvert ResumeДокумент2 страницыJennifer Boisvert Resumeapi-241522594Оценок пока нет
- New Expert Recommendations for Preventing and Treating Childhood ObesityДокумент4 страницыNew Expert Recommendations for Preventing and Treating Childhood ObesitySylvia GonzalezОценок пока нет
- TABLE OF CONTENTS Ewc 661Документ5 страницTABLE OF CONTENTS Ewc 661Abdul QayumОценок пока нет
- Benefits of CBD Himalayan Salt Lamps For SleepДокумент2 страницыBenefits of CBD Himalayan Salt Lamps For SleepTarun KumarОценок пока нет
- Macrobolic Nutrition - Priming Your Body To Build MusclesДокумент46 страницMacrobolic Nutrition - Priming Your Body To Build Musclespoet775100% (1)
- Eat Better Start Better1 PDFДокумент86 страницEat Better Start Better1 PDFJessa Mae AndresОценок пока нет
- Most Common Edible Marine Fishes in KeralaДокумент16 страницMost Common Edible Marine Fishes in KeralaAneesh B LalОценок пока нет
- Running Head: CHILDHOOD OBESITY 1Документ8 страницRunning Head: CHILDHOOD OBESITY 1VirginiaОценок пока нет
- Up Your Bench Press 30lbs in 30 DaysДокумент24 страницыUp Your Bench Press 30lbs in 30 DaysCharles SeekОценок пока нет
- The Risk of ObesityДокумент5 страницThe Risk of ObesityMaricel ReyesОценок пока нет
- Jurnal Tentang Laktasi: Diusulkan OlehДокумент10 страницJurnal Tentang Laktasi: Diusulkan OlehAtun AmbawaniОценок пока нет
- Talisay High School: True Home of SuccessДокумент2 страницыTalisay High School: True Home of SuccessRichard CavienteОценок пока нет
- Produk: Forvita: Departemen Ilmu Dan Teknologi Pangan, Fateta-IpbДокумент17 страницProduk: Forvita: Departemen Ilmu Dan Teknologi Pangan, Fateta-IpbIrmayantiОценок пока нет
- The 21minute Peak Performance Body Workout GuideДокумент20 страницThe 21minute Peak Performance Body Workout GuideHugo Mantilla100% (2)
- Individual Bmi Monitoring FormДокумент2 страницыIndividual Bmi Monitoring FormFredimar PatarayОценок пока нет
- Superman 2.weekДокумент5 страницSuperman 2.weekSzvami ItarabОценок пока нет
- I. Data Table Solubility Test: Experiment No. 3 LipidsДокумент3 страницыI. Data Table Solubility Test: Experiment No. 3 LipidsTyn TynОценок пока нет
- Chapter 1: Food, Nutrition, and Health: Nix: Williams' Basic Nutrition & Diet Therapy, 12 EditionДокумент6 страницChapter 1: Food, Nutrition, and Health: Nix: Williams' Basic Nutrition & Diet Therapy, 12 EditionaliОценок пока нет
- Nutritional Needs Preschool To School Age PPT RevisedДокумент55 страницNutritional Needs Preschool To School Age PPT RevisedMakiОценок пока нет
- Perceptions and Health Effects of Electronic Cigarettes Among ColДокумент48 страницPerceptions and Health Effects of Electronic Cigarettes Among Colabigail raccaОценок пока нет
- Insanity - Dig Deeper!: Week 1 6-Jan 7-Jan 8-JanДокумент3 страницыInsanity - Dig Deeper!: Week 1 6-Jan 7-Jan 8-JanCarlos RodriguezОценок пока нет