Академический Документы
Профессиональный Документы
Культура Документы
Clinical Implications of PTEN Loss in Prostate Cancer
Загружено:
medp7060Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Clinical Implications of PTEN Loss in Prostate Cancer
Загружено:
medp7060Авторское право:
Доступные форматы
REVIEWS
Clinical implications of PTEN loss in
prostate cancer
Tamara Jamaspishvili1,2, David M. Berman1,2, Ashley E. Ross3, Howard I. Scher4,
Angelo M. De Marzo5,6, Jeremy A. Squire7, and Tamara L. Lotan5,6
Abstract | Genomic aberrations of the PTEN tumour suppressor gene are among the most common
in prostate cancer. Inactivation of PTEN by deletion or mutation is identified in ~20% of primary
prostate tumour samples at radical prostatectomy and in as many as 50% of castration-resistant
tumours. Loss of phosphatase and tensin homologue (PTEN) function leads to activation of the
PI3K–AKT (phosphoinositide 3‑kinase–RAC-alpha serine/threonine-protein kinase) pathway and is
strongly associated with adverse oncological outcomes, making PTEN a potentially useful genomic
marker to distinguish indolent from aggressive disease in patients with clinically localized tumours.
At the other end of the disease spectrum, therapeutic compounds targeting nodes in the PI3K–
AKT–mTOR (mechanistic target of rapamycin) signalling pathway are being tested in clinical trials
for patients with metastatic castration-resistant prostate cancer. Knowledge of PTEN status might
be helpful to identify patients who are more likely to benefit from these therapies. To enable the
use of PTEN status as a prognostic and predictive biomarker, analytically validated assays have
been developed for reliable and reproducible detection of PTEN loss in tumour tissue and in blood
liquid biopsies. The use of clinical-grade assays in tumour tissue has shown a robust correlation
between loss of PTEN and its protein as well as a strong association between PTEN loss and adverse
pathological features and oncological outcomes. In advanced disease, assessing PTEN status in
liquid biopsies shows promise in predicting response to targeted therapy. Finally, studies have
shown that PTEN might have additional functions that are independent of the PI3K–AKT pathway,
including those affecting tumour growth through modulation of the immune response and tumour
microenvironment.
Prostate cancer is the most commonly diagnosed cancer the disease have been established. The phosphatase and
and the third leading cause of cancer-related death in tensin homologue (PTEN) tumour suppressor on chro-
men in the United States1. However, the vast majority mosome 10 and the phosphoinositide 3‑kinase (PI3K)
of patients diagnosed with prostate cancer will not die signalling axis it restrains are among the most com-
from the disease1. This conundrum results in a need monly altered pathways in primary prostate cancer 3,4.
to improve clinical risk stratification to identify which Furthermore, animal models and correlative biomarker
patients can be safely treated by active surveillance (AS), studies in humans have overwhelmingly nominated
which patients can be cured by therapies directed solely PTEN loss as a critical pathway to disease progression in
at the prostate, and which patients require the integra- hormone naive and castration-resistant prostate cancer
tion of systemic therapy. Although clinicopathological (CRPC). In CRPC, improved mechanistic understand-
variables are useful for risk stratification, as many as 30% ing and identification of the oncogenic drivers of tumour
of men considered to be eligible for AS based on these growth and reciprocal feedback in this signalling path-
variables are found to already harbour or progress to way have led to the design of biologically informed stud-
advanced disease and require intervention2, highlight- ies in which patient benefit is being demonstrated. In
ing the unmet need for more informative determinants this setting, PTEN might be an important biomarker to
Correspondence to T.L.L. of prognosis. Next-generation sequencing has elucidated predict the likelihood of therapeutic response. Here, we
tlotan1@jhmi.edu many molecular alterations and molecular subclasses review the biology of the PTEN tumour suppressor and
doi:10.1038/nrurol.2018.9 in prostate cancer; however, aside from the androgen its relationship to prostate cancer. We further discuss the
Published online 20 Feb 2018 receptor (AR) signalling axis, few molecular drivers of validation and clinical utility of PTEN as a prognostic
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 1
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Key points substrate AKT. Active phosphorylated AKT modulates
a number of downstream targets, including mTOR sig-
• Large-scale next-generation genetic analyses of prostate cancer emphasize the nalling, that have key roles in the regulation of apoptosis,
frequent occurrence and importance of focal genomic deletions inactivating PTEN cell cycle progression, cellular proliferation, metabolism,
• Phosphatase and tensin homologue (PTEN) loss in radical prostatectomy samples is differentiation, and invasion6. In its role as a lipid phos-
often concurrent with genomic rearrangements involving the ETS family phatase, PTEN modulates an enormous number of
transcription factors cellular processes, including cell polarity and motility,
• PTEN loss is reproducibly associated with adverse oncological outcomes by itself or in cellular senescence, and modulation of the tumour
combination with other biomarkers and helps distinguish indolent tumours from microenvironment 6. In addition, the phosphatase activ-
those likely to progress ity of PTEN seems to mediate aspects of both innate and
• PTEN might be a useful prognostic biomarker to distinguish potentially aggressive adaptive immunity 7,8.
Grade Group 1 or 2 tumours, which might make patients poor candidates for active Beyond its role as a lipid phosphatase, PTEN has
surveillance programmes established protein phosphatase activity, leading to
• Robust clinical assays using immunohistochemistry and fluorescence in situ functions that are independent of PI3K–AKT sig-
hybridization (FISH) have been developed to reproducibly measure PTEN protein nalling. Study of PTEN mutations that have lost lipid
and gene loss using diagnostic tissue biopsies and circulating tumour cells
phosphatase but retain protein phosphatase activity
from plasma
in cell lines has revealed numerous novel protein sub-
• PTEN loss is associated with suppression of androgen receptor (AR) transcriptional
strates of PTEN and diverse functions in regulating
output, and phosphoinositide 3‑kinase (PI3K) inhibitors activate AR signalling,
cell adhesions via focal adhesion kinase 1 (FAK; also
suggesting potential efficacy of combination therapies targeting the PI3K and AR
signalling pathways known as FADK1)9 and non-receptor proto-oncogene
tyrosine-protein kinase SRC 10. This protein phos-
• Emerging studies indicate that PTEN loss is associated with alterations to cellular
interferon responses in the tumour microenvironment — tumours with loss of PTEN phatase activity might modulate many of the nuclear
are more likely to have an immunosuppressive microenvironment, suggesting that functions of PTEN, including cell cycle regulation11, as
advanced prostate cancers with PTEN loss might be amenable to immune-based nuclear PIP3 pools are relatively insensitive to PTEN
therapies lipid phosphatase12. In addition, ample evidence sup-
ports a role for PTEN in the nucleus that is entirely
PI3K‑independent. PTEN localizes to centromeres,
biomarker in localized prostate cancer and consider and PTEN mutations that disrupt this interaction lead
progress towards realizing the potential of PTEN as a to centromeric instability. PTEN-null cells demon-
predictive biomarker in advanced metastatic CRPC. strate spontaneous DNA double-strand breaks, prob-
ably owing to PTEN-mediated regulation of DNA
Biology of the PTEN tumour suppressor repair protein RAD51 homologue 1 (RAD51) expres-
PTEN acts as a dual-specificity phosphatase, convert- sion13,14. Sumoylation might regulate nuclear localiza-
ing phosphatidylinositol 3,4,5‑trisphosphate (PI(3,4,5) tion of PTEN and contribute to its role in DNA damage
P3 or PIP3) into phosphatidylinositol 4,5‑bisphosphate repair 14. These studies have formed the basis for clinical
(PI(4,5)P2 or PIP2)5. In this manner, PTEN functions trials evaluating poly(ADP-ribose) polymerase (PARP)
as a direct antagonist of the activity of class I PI3K, a inhibitors to treat prostate cancer with PTEN loss.
family of enzymes that convert PIP2 to PIP3, resulting
in the activation of the downstream RAC-α serine/ Characteristics of PTEN inactivation
threonine-protein kinase (AKT) and mechanistic target PTEN genomic deletion in prostate cancer was first
of rapamycin (mTOR) signalling cascades (FIG. 1). Loss identified almost 2 decades ago15–17, and subsequent
and/or inactivating mutation of PTEN result in un sequencing studies have demonstrated that PTEN is the
opposed activity of PI3Ks and accumulation of PIP3 on most commonly lost tumour suppressor gene in primary
the cell membrane, which leads to recruitment and acti- disease3,18,19. The vast majority of prostate tumours with
vation of proteins containing pleckstrin homology (PH) PTEN loss inactivate PTEN by genomic deletion3,18,19
domains, including the 3‑phosphoinositide-dependent (FIG. 2). However, depending on the type of cohort exam-
protein kinase 1 (PDK1; also known as PDPK1) and its ined and the assay used to determine PTEN status, the
reported rate of PTEN gene deletions in prostate cancer
varies (TABLE 1). This variation is probably partly due to
Author addresses the fact that the frequency of PTEN deletion is highly
correlated with increasing Gleason score and tumour
1
Division of Cancer Biology and Genetics, Cancer Research Institute,
Queen’s University, Kingston, Ontario, Canada.
stage20–22. However, the fact that few analytically vali-
2
Department of Pathology and Molecular Medicine, Queen’s University, Kingston, dated assays have been performed to determine PTEN
Ontario, Canada. status has also contributed to this variability, which is
3
Department of Urology, Johns Hopkins University, Baltimore, MD, USA. a key consideration to keep in mind when reviewing
4
Genitourinary Oncology Service, Department of Medicine, Memorial Sloan Kettering the data.
Cancer Center and Weill Cornell Medical College, New York, NY, USA. In early studies using microsatellite analysis, loss of
5
Department of Pathology, Johns Hopkins University, Baltimore, MD, USA. heterozygosity (LOH) at the PTEN locus was reported
6
Department of Oncology, Johns Hopkins University, Baltimore, MD, USA. in 10–55% of primary and advanced tumours from sur-
7
Department of Pathology and Legal Medicine, University of Sao Paulo, Campus gical cohorts15,17,23–26. In studies using fluorescence in situ
Universitario Monte Alegre, Ribeirão Preto, Brazil.
hybridization (FISH), loss of at least one PTEN allele has
2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Growth factor receptor tumours, of which many have hemizygous deletions
involving the second allele18,19,39,40,50. The majority of
mutations are truncating, with relatively few missense
mutations. Epigenetic inactivation, in which loss of
PIP3 PI3K PIP2
PTEN protein is a result of promoter methylation, has
PIP3 PDK1
PIP2
been described in other tumour types, such as breast
AKT PTEN cancer 51,52. Few contemporary studies have investigated
PIP2 P Lipid phosphatase PIP2 PTEN hypermethylation in primary prostate cancers,
and most have reported negative results53.
• Cell growth Protein Other potential PTEN inactivation mechanisms
• Proliferation FAK, phosphatase
SRC
PTEN include microRNA (miRNA) and noncoding RNA
• Survival
• Migration (ncRNA). Several mRNAs, including the PTEN pseudo
mTOR
activation gene PTENP1, might have growth-suppressive and
Centromere stability tumour-suppressive properties and can act as competing
PTEN endogenous RNAs (ceRNAs) to miRNAs that can regu
Double-strand break repair late PTEN levels54. PTEN-targeting miRNAs are aber-
Figure 1 | The diverse cellular roles of PTEN. Phosphatase and tensin homologue rantly overexpressed in human prostate tumours and are
(PTEN) acts as lipid phosphatase, converting phosphatidylinositol 3,4,5‑trisphosphate
Nature Reviews | Urology capable of initiating prostate tumorigenesis in vitro and
(PIP3) into phosphatidylinositol 4,5‑bisphosphate (PIP2). In this capacity, PTEN antagonizes in vivo55. Finally, PTEN is post-translationally regulated
the function of class I phosphoinositide 3‑kinase (PI3K) activity, which converts PIP2 to by phosphorylation, ubiquitylation, oxidation, acetyla-
PIP3. This lipid phosphatase activity of PTEN suppresses the activation of the downstream tion, proteasomal degradation, and subcellular localiza-
oncogenic RAC-alpha serine/threonine-protein kinase (AKT) and mechanistic target of tion and by its interactions with other proteins56. Among
rapamycin (mTOR) signalling cascades. However, PTEN also has several other
these inactivation mechanisms, post-translational mod-
noncanonical functions, including weak protein phosphatase activity with known kinase
ifications, such as phosphorylation and ubiquitylation,
substrates such as focal adhesion kinase 1 (FAK) and proto-oncogene tyrosine-protein
kinase SRC. Finally, PTEN probably functions in the nucleus in a PI3K‑independent have been shown to decrease PTEN protein levels,
manner to promote chromosome stability and DNA repair. PDK1, 3‑phosphoinositide- whereas oxidation and acetylation reduce PTEN activ-
dependent protein kinase 1. ity 57. However, the frequency with which such inactiva-
tion events occur in human prostate tumours remains
unclear.
been reported in up to 68% of primary tumours from Most evidence indicates that PTEN inactivation
various historical surgical cohorts20,27–35. Subsequent occurs in primary tumours before they metastasize.
studies have been reporting PTEN deletion in around Sequencing studies have demonstrated that PTEN dele-
15–20% of surgically treated men 3,22,36,37(TABLE 1) . tion typically occurs identically in at least a subset of
Consistent with the strong correlation with tumour tumour cells from the primary and all or most sampled
stage, PTEN loss is more common in prostate cancer metastases38,58,59. However, in contrast to TMPRSS2–ERG
metastases than in primary tumours, with most studies rearrangements (the most common gene rearrangement
reporting rates of loss near 40%4,17,33,38,39 (TABLE 1). Data in prostate cancer), PTEN deletion is frequently hetero
from a CRPC cohort published in 2015 showed deep geneous within the primary tumour, suggesting that it
(likely homozygous) deletions in ~30% of patients, with usually occurs after ERG rearrangement 34,60,61 (FIG. 3).
truncating mutations and gene fusions in an additional This heterogeneity, occurring in up to 40% of primary
10%40. Racial ancestry might also affect the frequency tumours with PTEN loss36,37,62, is an important chal-
of PTEN loss. Primary prostate tumours arising in lenge for detection of PTEN status in diagnostic biopsy
African-American men have lower rates of PTEN loss specimens. The relatively late loss of PTEN in primary
than tumours arising in matched patients of European- tumours is consistent with low rates of PTEN loss
American ancestry 41–44. However, the association of observed in isolated prostatic intraepithelial neoplasia
PTEN loss with poor prognosis seems to be independent (PIN), which is widely believed to represent a precursor
of racial ancestry 42. to invasive prostate cancer 63–65.
Although biallelic deletion is the most common
reason for PTEN inactivation, it can also be silenced PTEN interactions during tumorigenesis
by alternative genetic and epigenetic mechanisms in a Mouse models have been useful to elucidate inter
minority of cases. Genomic rearrangements have been actions between PTEN loss and other genes and sig-
reported to involve and inactivate PTEN and nearby nalling pathways commonly altered in human prostate
genes45–47. The frequency with which PTEN is inacti- cancer. In mice, monoallelic Pten loss (Pten +/−) is
vated by mutations or methylation seems to be quite sufficient to induce PIN but does not lead to inva-
low, at <10% of cases (TABLE 1). Results of early Sanger sive prostatic carcinoma 66–69. By contrast, biallelic
sequencing studies reported a high rate of mutations in ablation of Pten in mice (Pten−/−) results in relatively
the PTEN promoter region, but some of these studies slow progression to locally microinvasive disease
were confounded by the existence of a PTEN pseudo and, much more rarely to micrometastatic prostate
gene (PTENP1) that harbours a high rate of such altera- carcinoma, the kinetics of which apparently depend,
tions48,49. Data from exon sequencing studies have shown at least in part, on the background strain of mouse
PTEN mutation rates hovering around 5% in primary used66,70,71. In mice, evidence supports the role of Pten
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 3
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
a b c d
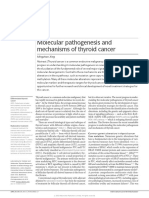
Figure 2 | Prostate cancer samples with variable PTEN protein expression by IHC and corresponding PTEN | Urology
Nature Reviews
FISH. a | Prostate tumour with intact phosphatase and tensin homologue (PTEN) identified with immunohistochemistry
(IHC) with two intact PTEN alleles detected using fluorescence in situ hybridization (FISH). PTEN IHC demonstrates intact
PTEN (top) and a four-colour FISH image from an adjacent section (bottom) shows two intact PTEN alleles (red) with two
intact copies of flanking genes, WAPAL (green) and FAS (aqua) as well as chromosome 10 centromeres (purple).
b | Prostate tumour showing PTEN expression using IHC with hemizygous PTEN deletion using FISH. PTEN IHC
demonstrates intact PTEN protein (top), with four-colour FISH image (bottom) from an adjacent section showing a
hemizygous PTEN deletion with loss of one PTEN gene (one red signal). As both centromeres (purple) and the WAPAL
(green) and FAS (aqua) probes that flank either side of PTEN are retained, this hemizygous deletion is likely to be
interstitial and restricted to the PTEN region. c | Prostate tumour showing absence of PTEN expression by IHC with
homozygous PTEN gene deletion detected in intraductal tumour by FISH. PTEN IHC image (top) shows loss of PTEN in
tumour glands. Four-colour FISH image from an adjacent section (bottom) shows a homozygous deletion with loss of
both PTEN genes. The retention of the centromeres (purple) and both WAPAL genes (green), but the presence of only one
copy of FAS (aqua), indicates that one of the deletions involved both PTEN and FAS. d | Prostate tumour showing PTEN
protein loss by IHC with hemizygous PTEN gene deletion by FISH. PTEN IHC demonstrates complete PTEN loss (top), with
four-colour FISH image (bottom) from an adjacent section showing a hemizygous PTEN deletion with loss of one PTEN
gene (red) along with flanking genes WAPAL (green) and FAS (aqua). This tumour demonstrates complex hemizygous
PTEN deletion, in which PTEN is deleted along with adjacent genes (WAPAL and FAS) located on both sides of PTEN.
Figure adapted from REF. 36, Macmillan Publishers Limited.
gene dosage in prostatic tumorigenesis 66; however, Additional genomic aberrations enhance prostate
whether this role of PTEN applies in human prostate tumorigenesis in the Pten-null mouse prostate78. ERG
cancer remains unclear. Patients with PTEN hemi (V-Ets Avian Erythroblastosis Virus E26 Oncogene
zygous tumours have intermediate outcomes between Related; also known as KCNH2) expression and Pten
those with wild-type PTEN and those with biallelic loss synergize to accelerate prostate carcinogenesis
loss; however, this effect could be due to inactivating in mouse models79,80. In the context of Pten loss, ERG
epigenetic or point mutations of the second allele, expression restores AR transcription in mouse models
which are not detectable by FISH36. Mouse prostate and human samples, providing a potential mechanism
tumours with Pten loss are notably less sensitive to for the common co‑occurrence of these two alterations81.
castration than those without Pten loss, suggesting a However, human data have generally not supported the
link between PTEN loss and castration resistance72–74. hypothesis that PTEN deletion and ERG rearrangement
In mouse models, the mechanism of this effect seems synergize in terms of poor oncological outcomes (see
to be downregulation of AR levels owing to recipro- below). Concomitant loss of Pten and Tp53 results in
cal feedback between PI3K activation and AR75; some aggressive tumour growth in the mouse prostate, which
evidence of this feedback has also been observed in is not observed with Tp53 deficiency alone71,82,83. Loss of
human prostate cancers75–77. These studies have been Tp53 might be associated with LOH of Pten, which facil-
the basis for numerous ongoing clinical trials testing itates hormone-refractory disease and bypasses cellular
combinations of androgen deprivation therapy (ADT) senescence71. Combined deletion of Pten, Rb1, and Tp53
and PI3K inhibitors. in the mouse prostate is associated with development of
4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Table 1 | Studies of PTEN status in contemporary prostate cancer cohorts
Technique Tissue type PTEN loss (%) Study
PTEN deletion a
Incidental tumour 17% (56/322) Reid et al., 2010 (REF. 99)
(two-colour FISH) (TURP)
PTEN deletion • Prostate cancer • 37.5% (112/298) Yoshimoto et al., 2012 (REF. 118)
(four-colour FISH) • CRPC • 62% (20/32)
PTEN deletion Prostate cancer 20% (458/2266) Krohn et al., 2012 (REF. 21)
(two-colour FISH)
PTEN mutation • Prostate cancer • 10.1% (1/11) Grasso et al., 2012 (REF. 39)
(sequence) • mCRPC • 8% (4/50)
PTEN copy number loss (arrays) Same cohort • 46% (5/11) Grasso et al., 2012 (REF. 39)
• 40% (20/50)
PTEN • Prostate cancer • 15% (42/282) Leinonen et al., 2013 (REF. 115)
immunohistochemistryb • CRPC • 45% (55/122)
• mCRPC • 61% (19/31)
PTEN deletion Incidental tumour 16% (104/643) Cuzick et al., 2013 (REF. 168)
(two-colour FISH) (TURP)
PTEN Same cohort 18% (119/675) Cuzick et al., 2013 (REF. 168)
immunohistochemistry
PTEN copy number and mutation mCRPC 40.7% (61/150) Robinson et al., 2015 (REF. 40)
(sequence)
PTEN mutation Prostate cancer 2% (7/333) TCGA et al., 2015 (REF. 3)
(sequence)
PTEN copy number loss (arrays) Same cohort 15% (50/333) TCGA et al., 2015 (REF. 3)
PTEN Prostate cancer 16% (166/1044) Ahearn et al., 2015 (REF. 37)
immunohistochemistry
PTEN deletion Prostate cancer 18% (112/612) Troyer et al., 2015 (REF. 22)
(four-colour FISH)
PTEN Same cohort 22% (158/731) Lotan et al., 2016 (REFS 36,62)
immunohistochemistry
PTEN Prostate cancer 24.2% (1890/7813) Lotan et al., 2017 (REF. 169)
immunohistochemistry Same cohort as REF. 21
CRPC, castration-resistant prostate cancer; FISH, fluorescence in situ hybridization; mCRPC, metastatic CRPC; PTEN, phosphatase and tensin homologue; TURP,
transurethral resection of the prostate. aTotal number of PTEN deletions (homozygous and hemizygous deletions combined). bOnly cases with absence of PTEN
protein are shown.
metastatic tumours demonstrating lineage plasticity 84, prostate organoids88. Similarly, CHD1, a chromatin
and human tumours with loss of these three tumour sup- helicase DNA-binding factor, is rarely lost in PTEN-
pressor genes are extremely aggressive and frequently null tumours, and combined loss of these tumour sup-
show neuroendocrine differentiation 85,86. Similarly, pressors is synthetic lethal in vitro and in vivo owing
combined loss of Pten and overexpression of the MYC to PTEN-deficiency-induced stabilization of CHD1,
proto-oncogene protein synergize to result in highly which is required for transcription of nuclear factor-κB
penetrant and aggressive androgen-insensitive tumours (NF‑κB) target genes89.
with a high rate of metastasis not observed with either
aberration on its own87. Mice with MYC overexpression PTEN as a prognostic biomarker
in addition to Pten and Tp53 loss also exhibit aggressive The introduction and widespread use of serum PSA in the
tumours with frequent local metastasis71,82. late 1980s led to a considerable increase in prostate can-
PTEN loss is typically mutually exclusive with sev- cer incidence and resulted in the overtreatment of many
eral other genomic alterations in human prostate can- clinically insignificant prostate tumours90. However, dis-
cer, including SPOP mutation and CHD1 loss, and study tinguishing indolent from aggressive prostate tumours
of these alterations in mouse and xenograft models has remains a challenge. Determination of which patients
helped to improve understanding of the biology that are eligible for AS is variable between institutions and
underlies these findings. Recurrent SPOP mutations are is largely based on biopsy pathology variables (Gleason
the most common mutations in primary prostate can- score, number of biopsy cores, maximum percentage
cer, occurring in close to 10% of cases. Although SPOP of core involvement) and serum PSA levels91. However,
mutation alone is insufficient to drive tumorigenesis in even in the most restrictive protocols, as many as 30% of
mouse models, it is sufficient to activate PI3K–mTOR men selected for AS programmes using these parameters
signalling on its own and uncouples the negative will be found to already harbour or to progress to high-
feedback between PI3K and AR signalling in human grade disease and require intervention2. Those men who
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 5
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
a PTEN ERG biomarkers might have the advantage of being more
stable, and, therefore, less prone to variation in pre-
analytic parameters such as tissue fixation conditions
and tissue age. Among prognostic DNA biomarkers
P
P that have emerged from the sequencing of thousands of
P
prostate cancers, PTEN gene loss is arguably one of the
most promising. PTEN inactivation in prostate tumours
is a nearly universal and highly replicable finding and is
N P associated with adverse oncological outcomes such as
increased tumour grade and stage, earlier biochemical
N
recurrence after radical prostatectomy, metastasis, pros-
tate-cancer-specific death, and androgen-independent
progression20,22,27,32,36,37,60,97. A meta-analysis of seven
previously published studies confirmed a strong corre-
b lation of PTEN genomic deletion with increased Gleason
score or increased likelihood of extraprostatic extension
in patients with surgically treated localized prostate can-
cer 98. PTEN loss is clearly associated with an increased
N risk of biochemical recurrence after prostatectomy in
N
P
N several large studies21,22,36. Perhaps most importantly,
PTEN was found to be an independent prognostic indi-
cator of prostate-cancer-specific death in patients treated
N either conservatively or surgically 37,99.
By taking advantage of the close association between
N
PTEN loss and increasing Gleason score, PTEN might
be useful as a prognostic biomarker in localized pros-
tate cancer. In this context, testing PTEN status could
potentially improve on current risk stratification pro-
Figure 3 | Heterogeneous immunohistochemical expression of ERG and PTEN in tocols when Gleason score is inaccurate, particularly in
prostate tumours. a | Heterogeneous phosphatase and tensin homologue (PTEN)
Nature Reviews loss is
| Urology
low-risk and low-to-intermediate risk groups, in which
observed in some tumour glands (N), with intact staining in other tumour glands (P),
whereas the same areas are uniformly positive for ERG expression, indicating that clonal clinical and pathological risk stratification can be in
ERG genomic rearrangement is probably present with subsequent subclonal PTEN loss. accurate. PTEN inactivation is generally about twice
b | Heterogeneous PTEN loss is seen in some tumour glands (N), with intact staining in as common in Gleason score 7 (Grade Group 2–3) dis-
other tumour glands (P), whereas the same areas are uniformly negative for ERG ease as in Gleason score 6 (Grade Group 1) disease at
expression (ERG genomic rearrangement is absent). radical prostatectomy when the true Gleason score is
known36,37. Accordingly, PTEN loss in Gleason pattern
3 tissue sampled from Gleason score 7 (Grade Group
demonstrated more aggressive disease within 1–2 years 2/3) tumours is substantially more frequent than PTEN
of initial diagnosis were probably misclassified, owing loss in Gleason pattern 3 tissue sampled from Gleason
to problems with blind biopsy sampling, and improved score 6 (Grade Group 1) tumours100. Consistent with
targeting of biopsies using MRI guidance has shown these data, PTEN loss in Gleason score 6 (Grade
promise for risk stratification in this context 92,93. Among Group 1) biopsies predicts upgrading to Gleason score
biopsy parameters, Gleason score is the most prog 7 (Grade Group 2/3) or higher in the radical prostatec-
nostic, and changes to the Gleason grading system have tomy specimen101,102. In Gleason 3 + 4 = 7 (Grade Group
further refined it 94. Gleason score describes the degree 2) tumour biopsies, PTEN loss is independently asso-
of morphological differentiation in the tumour based on ciated with a twofold increase in risk of extraprostatic
histological examination of tumour architecture. When extension after prostatectomy 103. The first study of the
determined on biopsy, the final Gleason score comprises utility of PTEN in an AS cohort of Gleason 6 (Grade
the score attributed to the most common architectural Group 1) tumours at biopsy showed that PTEN loss
pattern or grade (ranging from grade 3 to grade 5) and was associated with an increased risk of subsequent
the second most common or highest grade pattern94. biopsy upgrading, discontinuation of AS, and adverse
Updates to approaches to tumour scoring in the past few histopathological features at radical prostatectomy 104.
years mean that Gleason scores have been categorized Finally, several studies examining PTEN status in
into five discrete and highly prognostic grade groups95. biopsies have used more concrete oncological end
However, despite these updates, the limit of what infor- points such as metastasis or death. In one small study,
mation can be inferred using tumour morphology is PTEN loss in the biopsy sample predicted increased
reaching its limit, and validated, tissue-based prognostic risk of CRPC, metastasis, and prostate-cancer-specific
biomarkers to identify potentially aggressive prostate mortality in surgically treated patients105.
tumours are needed. Until further studies are published using metastasis
Although several RNA-based commercial assays have or death as clinical end points, the available data support
shown potential utility in this context 96, DNA-based the use of PTEN loss as an early marker of aggressive
6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
prostate cancer in clinical biopsy samples that are deter- needle biopsy is associated with underlying high-grade
mined to be Grade Group 1 or potentially low-volume invasive carcinoma in the prostate >90% of cases110,111.
Grade Group 2. In these cases, PTEN status could sub- In keeping with its association with underlying high-
stantially improve the prognostic information contained grade invasive carcinoma, intraductal carcinoma of the
in the Gleason grade and might improve stratification prostate commonly shows PTEN loss, whereas this is
of patient therapy — for example, the fact that patients extraordinarily uncommon in PIN63–65,112. Thus, PTEN
with PTEN loss might be inappropriate for AS proto- status assessment can help to distinguish these lesions
cols (FIG. 4). Like many molecular markers, the high and to clarify the patient prognosis in the setting of
frequency of PTEN loss heterogeneity in the setting of intraepithelial proliferations113.
primary tumours can make it challenging to accurately
assess PTEN status in a small biopsy sample. At least one PTEN in combination with ERG
study has suggested that PTEN testing in a minimum PTEN loss is enriched twofold to fivefold among local-
of two cores with cancer foci is necessary to accurately ized tumours with ERG gene rearrangement compared
assess PTEN status in the context of random needle with those without this alteration30,33,36,37,60,79,80. By itself,
biopsies106. In the future, improved prostate imaging ERG gene rearrangement does not portend an altered
modalities, such as multiparametric MRI, might also prognosis in most surgical cohorts114. Dissecting the
help to ensure sampling of the dominant tumour nodule, interaction of PTEN and ERG with respect to onco
in which PTEN status might be most clinically relevant. logical outcomes in prostate cancer has been complex.
Another emerging area in which PTEN could be Based on animal models demonstrating synergy between
used as a biomarker is in the context of differential PTEN and ERG for tumour progression and early stud-
diagnosis of intraepithelial lesions in prostate biopsies. ies of the interaction of PTEN and ERG with respect to
Intraductal carcinoma of the prostate and high-grade biochemical recurrence, patients with combined ERG
PIN are the two main intraepithelial neoplastic lesions rearrangement and PTEN inactivation were initially
occurring in the prostate; they exist along a morpho- thought to be likely to have the worst prognosis of all
logical spectrum107. PIN is frequently an isolated find- patient groups30,115,116. However, additional, larger studies
ing, occurring in biopsies without invasive carcinoma using biochemical recurrence as an outcome measure
and is generally not associated with an increased risk have found that patients with PTEN loss also did poorly,
of cancer diagnosis on a subsequent biopsy 108,109. By regardless of ERG status21,35,36. When lethal prostate
contrast, the presence of intraductal carcinoma on cancer rather than the surrogate outcome measure of
High PSA, abnormal DRE
Biopsy
Grade IHC
No cancer Group 1 or PTEN intact PTEN partial loss PTEN ambiguous PTEN complete loss
2 cancer (IHC) (IHC) (IHC) (IHC)
Grade
Group >2
Perform PTEN FISH
cancer
No loss Hemi loss Homo loss
(PTEN+/+) (PTEN–/+) (PTEN–/–)
Prognosis reflects Prognosis reflects PTEN status
clinicopathological variables and clinicopathological variables
Figure 4 | Algorithm for when to determine PTEN status on diagnostic biopsy material using IHC and FISH. Prostate
biopsy is indicated to confirm or exclude cancer in patients with elevated serum PSA levels and/or Nature Reviews
abnormal | Urology
digital rectal
exam (DRE). Patients with persistent PSA elevation might require repeat biopsy. If cancer is detected and is low‑to‑
intermediate risk (Grade Group 1 or 2; Gleason score 3 + 3 or 3 + 4), phosphatase and tensin homologue (PTEN) status can
be ascertained using immunohistochemistry (IHC) staining. If PTEN protein expression is intact, the prognosis reflects the
patient’s clinicopathological variables (for example, Grade Group, PSA, age, DRE). If IHC demonstrates complete PTEN
loss, biomarker status should be considered in the patient’s prognosis along with clinicopathological variables and
fluorescence in situ hybridization (FISH) is not necessary. However, if PTEN loss is incomplete or ambiguous (for example,
negative PTEN staining in cancer glands along with negative PTEN expression in internal control, such as benign glands
and/or stroma), FISH is recommended and bears similar connotations to PTEN loss determined by IHC. If cancer is
detected and is high risk (Grade Group 3, 4 and 5; Gleason score 4 + 3 and 4 + 4, ≥4 + 5), PTEN status does not need to be
determined because the prognosis will be strongly driven by clinicopathological variables.
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 7
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
biochemical recurrence is used, it seems that tumours FISH into clinical pathology laboratory workflows have
with PTEN loss that lack ERG rearrangement have the prompted researchers to develop a less expensive and
worst outcomes, after either surgical or conservative time-consuming clinical-grade immunohistochemical
therapies37,99. In fact, only the subset of tumours with assay to detect PTEN loss36,97. In addition, as PTEN
PTEN loss that lack ERG rearrangement has worse onco- loss is commonly subclonal and/or focal in primary
logical outcomes than those tumours with PTEN intact, prostate tumours34,61,77,97, detection of PTEN deletion
suggesting that the two alterations should be assayed — especially focal losses — by FISH can be techni-
together to improve prognostication. This discrepancy cally challenging and is more feasible using IHC than
between results from studies examining biochemical FISH. IHC protocols have been successfully validated
recurrence versus lethal prostate cancer might be due on the Ventana Benchmark platform in a Clinical
to an interaction of PTEN–ERG status with treatments Laboratory Improvement Amendments (CLIA)-
received after biochemical recurrence, such as radiation certified laboratory with high interobserver reproduc-
or hormone therapy. An additional study has shown that ibility in the scoring system36,37. Correlation of PTEN
PTEN loss combined with high immunohistochemical gene loss by FISH and protein loss by IHC are quite
expression of AR, especially in ERG-negative cancers, high36,97,120,121, but some discordance can result from
predicted initiation of secondary treatments, shortened the fact that PTEN loss can theoretically be due to very
disease-specific survival time, and stratified Gleason small genomic deletions or transcriptional or post-
score 7 (Grade Groups 2 and 3) patients into different transcriptional regulation, in which case FISH might
prognostic groups117. Cumulatively, these results suggest show a false negative result. Interestingly, heterogeneous
that PTEN loss is most closely associated with lethal or partial PTEN protein loss was a weaker prognostic
prostate cancer among patients whose tumours have indicator than homogeneous or complete loss, using
not rearranged ERG. Thus, triaging patients by com- either biochemical recurrence or lethal prostate cancer
bining PTEN status with other prognostic biomarkers as the outcome variable, but the reasons for this effect
at the time of biopsy might also help to stratify patients remain unclear 36,37. Compared with FISH, IHC is not as
with localized disease into AS versus definitive therapy sensitive in detecting hemizygous PTEN loss36; however,
cohorts. whether this discrepancy adds prognostic information
remains unclear 22. Overall, the most cost-effective and
Assays to detect PTEN loss time-effective protocol to screen for PTEN loss in human
Although the potential utility of PTEN as a biomarker prostate tissue should include initial screening by IHC,
in localized disease — with or without other molecu- followed by FISH analysis in cases that are ambiguous
lar markers — is well established, very few assays have or indeterminate by IHC (generally comprising <5% of
been analytically validated for clinical use in this setting. cases) and potentially in cases with heterogeneous loss
Analytical validation is an absolute requirement for any of PTEN by IHC, in which FISH can add prognostic
molecular biomarker that is to be used in clinical deci- information36 (FIG. 4).
sion-making. In clinical pathology laboratories, FISH As sensitive and noninvasive measurement of DNA
and immunohistochemistry (IHC) have predominantly biomarkers in blood and urine becomes increasingly
been used to assess patient samples for changes in PTEN feasible with advanced sequencing technologies, inter-
copy number and protein expression (FIG. 2). FISH is a est in detecting PTEN deletion in bodily fluids is grow-
quantitative and highly specific method for determi- ing. Such tests could be particularly useful in patients
nation of gene copy number within interphase cells with advanced metastatic prostate cancer, in which
in tissue sections27. Probe design, sample preparation, PTEN might serve as predictive biomarker (FIG. 5). One
hybridization protocols, and signal scoring criteria are relevant method is detection of PTEN status in circu-
critically important factors for quality assurance. PTEN lating tumour cells (CTCs). Epithelial cell adhesion
FISH assays can be compromised by a high background molecule (EpCAM) and cytokeratin-based enrichment
level of signal losses associated with tangential section- protocols for CTCs are currently the only FDA-approved
ing of nuclei during slide preparation. A number of platform for CTC analysis (CellSearch), but other
new probe designs (typically using two PTEN-flanking methodologies are gaining traction. PTEN status can be
probes for WAPAL (also known as WAPL) and FAS in evaluated in CTCs by FISH using an enrichment-free
addition to the PTEN probe and the centromere con- platform and is also highly concordant with PTEN sta-
trol probe) have been shown to increase the accuracy of tus in matched fresh-frozen tissues122. Cell-free DNA in
FISH deletion assays so that true chromosomal deletions blood might also prove useful to assess PTEN status123
can be readily distinguished from the false signal losses and urine is another accessible sample type that might
caused by sectioning artefacts118,119. be suitable for interrogation of PTEN status via cell-free
Compared with IHC, one advantage of FISH is that DNA124. Most of these studies remain focused on bio-
both hemizygous and homozygous gene loss can be marker development, but additional thorough analytical
detected with high sensitivity. As might be expected validation studies will be required before fluid-based
from gene dosage effects in mice66, hemizygous PTEN DNA biomarker measurements can be used clinically 125.
loss is more weakly associated with adverse outcomes Ongoing clinical trials incorporating CTCs and cell-free
than homozygous loss21,22. However, the relatively high DNA measurements will add to our understanding of the
cost of FISH probes, the complexity of standardized potential use of these assays, although many of these trials
scoring protocols, and the challenge of integrating are focused on AR splice variants rather than PTEN126–129.
8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
GG1 cancer GG2 cancer GG>2 cancer
No PTEN loss Any PTEN loss No PTEN loss Any PTEN loss No PTEN loss Any PTEN loss
Consider active surveillance Consider definitive treatment
Figure 5 | Proposed management options using clinicopathological variables at biopsy and PTEN status. Patients
with Grade Group (GG) 1 cancer and no loss of phosphatase and tensin homologue (PTEN) on biopsy (byReviews
Nature immunohisto-
| Urology
chemistry (IHC) and/or fluorescence in situ hybridization (FISH)) should be considered for active surveillance. Patients with
GG1 cancer with PTEN loss should be considered for definitive treatment using radiotherapy or prostatectomy. In some
clinical contexts, patients with GG2 cancer with no loss of PTEN could be considered for active surveillance, particularly if
they have low-volume disease and a low percentage of Gleason pattern 4 (indicated by dashed arrow). Patients with GG2
tumours with PTEN loss or tumours greater than GG2 should be considered for definitive treatment in most cases.
One ongoing trial creates a multi-institutional database using everolimus are currently in progress141,142. The
of CTC DNA for chromosomal gains and/or losses and hope is that the results from these trials will be similar
RNA for AR splice variants in patients with mCRPC to the breast cancer BOLERO‑2 trial, in which a com-
before and after treatment with abiraterone, enza bination of hormonal therapy and mTORC1 inhibition
lutamide, or taxane-based chemotherapy, which aims to was quite promising 143. Other trials testing the efficacy
identify markers of therapy-resistance130. of PI3K–AKT–mTOR inhibition with additional agents
in the context of AR axis signalling suppression are
PTEN-targeted therapies in mCRPC currently underway or soon to be reported, including
The potential role of PTEN as a predictive biomarker a phase 1b trial of enzalutamide with the mTOR kinase
in the context of mCRPC is under examination. inhibitor CC‑115 (REF. 144) and a phase 2 study of the
Consistent with mouse models predicting the asso- PI3K–mTOR inhibitor GDC‑0980 with abiraterone145.
ciation of PTEN inactivation with development of One limitation of the aforementioned studies is
CRPC, PTEN loss has been associated with decreased that they have generally been conducted on unselected
response to novel AR‑targeted therapies, including and heterogeneous patient populations, some with and
abiraterone131. However, the most exciting context for some without PTEN loss. This limitation is, in part,
PTEN as a predictive biomarker has been in the setting due to the historical lack of uniformly accepted and
of therapies targeted to PI3K–AKT–mTOR signalling. highly analytically validated assays to measure PTEN
PTEN loss is associated with unimpeded PI3K and loss. Given the relatively high frequency of PTEN loss
downstream signalling, so the initial outlook for the in the CRPC setting, that a therapeutic benefit would
efficacy of PI3K–AKT–mTOR inhibitors in prostate be seen even in unselected patients would seem likely.
cancer was optimistic (FIG. 6). However, despite promis- However, subset analyses stratified by PTEN status
ing performance in preclinical models, the clinical effi- might be required to identify benefit for agents tar-
cacy of these drugs as single agents in CRPC has been geting the PI3K–AKT–mTOR pathway. For example,
uniformly low 132,133. Preclinical models have suggested one trial of a novel ATP-competitive AKT inhibitor
that single-agent therapy with inhibitors targeting the (ipatasertib or GDC‑0068) with abiraterone showed
PI3K–AKT–mTOR pathway activates AR signalling some responses, which occurred much more fre-
via compensatory crosstalk; thus, co‑targeting the AR quently in patients harbouring PTEN loss (identified
and the PI3K pathways might be a more effective thera by IHC)145,146. This promising result suggests that PTEN
peutic approach than using single-agent therapies75,134–136. status, if measured using an analytically validated test,
However, early clinical trial data with PI3K inhibitors could indeed ultimately become a predictive biomarker
and novel androgen-targeted therapies do not look in terms of selection of patients for treatment with
uniformly promising in unselected patients. The trial AKT inhibitors. These data, combined with the ease of
of BKM‑120 — a pan‑PI3K inhibitor — with enzaluta- PTEN status testing by analytically validated IHC or
mide did not show efficacy 137, whereas BEZ235 — a dual FISH, emphasize the need for additional trials selected
PI3K–mTOR inhibitor — in combination with abirater- for tumours with PTEN loss to improve efficacy assess-
one, was poorly tolerated138. Further trials of abirater- ment of combined AR‑targeted and PI3K‑targeted,
one in combination with either BKM‑120 or BEZ235 AKT-targeted, or mTOR-targeted therapies.
are not planned139. One trial of everolimus (RAD001, Another issue with early trials of pan‑PI3K inhibitors
an mTOR inhibitor) and bicalutamide warrants further is that the toxic effects associated with their use are often
investigation, although the treatment-associated toxic limiting. Given that evidence for nonredundant roles of
effects were somewhat limiting 140. Additional trials of PI3K isoforms in different tumour types is increasing,
novel AR‑signalling inhibitors and mTORC1 inhibition isoform-specific inhibitors of PI3K might have a role in
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 9
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
BKM120 GDC-0980 BEZ235 therapies153,154. Finally, emerging evidence suggests that
an alternative variant of PTEN known as PTEN-Long, is
secreted by cells155. The secreted protein can be taken up
IRS-1 PI3K
by other cells, including those that have lost endogenous
PTEN PTEN activity. When mice with xenograft tumours lack-
ing PTEN were treated with PTEN-Long, their tumours
GDC-0068 AKT S473 stayed stable, and some even regressed155. The findings
suggest that, in principle, recombinant secreted PTEN
itself is a novel treatment approach to tumours with
TSC and TSC2 PTEN mutations or deletions156. Ultimately, these stud-
ies emphasize the importance of understanding PTEN
regulatory mechanisms and function for the design of
RHEB novel therapeutic strategies in advanced prostate cancer.
mTOR GBL
Raptor Sin1
mTORC1 PTEN loss and immune microenvironment
mTOR
Rictor GBL Prostate cancer is a slow-growing disease, making it
RAD001 BEZ235
mTORC2 an ideal tumour for immunotherapy. This longer dis-
MLN0128
ease course provides a considerable time period during
S6K1 which novel therapeutics could be applied to trigger an
Figure 6 | Selected drugs in clinical trials targeting the PI3K–AKT pathway that have antitumour immune response157. Emerging data sug-
been used in combination with androgen deprivation therapy. Nature Reviews | Urology
Phosphoinositide gest that, in addition to its established role as a tumour
3‑kinase (PI3K) inhibitors (GDC‑0980, BKM120), combined PI3K–mTOR (mechanistic suppressor, PTEN loss itself is an immunosuppressive
target of rapamycin) inhibitors (BEZ235), mechanistic target of rapamycin complex 1 event 8. Successful immunotherapy in prostate can-
(mTORC1) inhibitors (RAD001), and mTOR kinase inhibitors (CC‑115) have been used in cer will depend on fully understanding the tumour
clinical trials in combination with novel and conventional androgen deprivation microenvironment and the inflammatory mechanisms
therapies. Whereas some trials have been largely negative (BKM‑120)137 or poorly that enable the tumour to evade immune responses, as
tolerated (BEZ235)138, others are promising and suggest that phosphatase and tensin
well as identification of actionable targets to enhance
homologue (PTEN) status is a useful predictive biomarker for response in some contexts
(for example, GDC‑0068 or ipatasertib)146. AKT, RAC-alpha serine/threonine-protein immune attack on tumour cells.
kinase; GBL, target of rapamycin complex subunit LST8 (also known as MLST8); The development of chronic prostatic inflammation
IRS1, insulin receptor substrate 1; mTORC2, mechanistic target of rapamycin complex 2; is often accompanied by histological lesions that seem to
PTEN, phosphatase and tensin homologue; Raptor, regulatory-associated protein of be precursors to prostate cancer 158, and histological evi-
mTOR; RHEB, GTP-binding protein RHEB; Rictor, rapamycin-insensitive companion dence shows that prostate tumours are often infiltrated
of mTOR; S6K1, ribosomal protein S6 kinase β-1; Sin1, target of rapamycin complex 2 by immune cells such as CD4+ and CD8+ T cells, natural
subunit MAPKAP1; TSC1, hamartin; TSC2, tuberin. killer (NK) cells, and antigen-presenting cells (dendritic
cells and macrophages)159. The ratios of each subtype are
prostate cancer treatment. PI3Ks consist of a catalytic sub- associated with different prognoses. For example, infil-
unit (p110α, p110β, or p110δ) complexed to a regulatory trating NK cells are associated with good prognosis and
subunit (p85)147. Both the p110α and p110β isoforms are are thought to provide a strong antitumour response160,
ubiquitously expressed; however, in the setting of PTEN whereas CD4+ cells, which are regulatory T cells (Treg
loss, preclinical data suggest that PI3Kα activity is rela- cells), suppress immune responses and are associated
tively suppressed and tumour cells rely more heavily on with a poor prognosis161.
the p110β isoform136. Accordingly, ablation of p110β, but Studies in melanoma, one of the first tumours to
not p110α, was sufficient to impede tumorigenesis in the show a clinical benefit with immunotherapy, have
PTEN-null mouse prostate148. However, even PI3Kβ inhi- shown that PTEN loss correlates with a reduction in
bition activates AR activity in preclinical models136; thus, T cell inflammatory responses and worse outcomes
PI3Kβ‑selective inhibitors combined with AR axis inhibi- with anti‑PD‑1 immunotherapy 162. PTEN has also
tion are currently being tested for their ability to suppress been shown to directly regulate interferon response
the reciprocal feedback activation of both pathways149,150. signalling pathways, and, in studies using oncolytic
Additional novel strategies are being evaluated in viruses, loss of PTEN has a crucial role in mediat-
preclinical studies. One potential therapeutic option ing antiviral innate immunity 7. For example, PTEN-
is combination therapy of PI3K inhibitors with PARP deficient cancer cells have muted type I interferon
inhibitors. PARP is an enzyme that modifies DNA at sin- responses and are more sensitive to viral infections
gle-strand breaks, leading to the recruitment of DNA than cells with intact PTEN7,163. Such alterations to
repair effectors151. Prostate tumour cells deficient in interferon regulation signalling pathways by PTEN
normal DNA repair mechanisms (such as tumours with are likely to have protumorigenic effects in addition
BRCA2 loss) are highly sensitive to PARP inhibition152. to the effects on the innate antiviral immune system.
Furthermore, nuclear PTEN might also have a role in These findings might explain why PTEN-deficient
DNA repair 13,14, raising the question of whether com- tumour cells are more permissive to interferon-
bined PARP and PI3K inhibition might be efficacious. sensitive oncolytic viruses and are an important con-
Preclinical prostate cancer models with combined Pten– sideration for future oncolytic therapy trials targeting
Tp53 loss show some response to these combination PTEN-deficient prostate cancers164.
10 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
The role of PTEN in the tumour immune response is cellular phenotypes, combinations of these phenotypes,
likely to act through activation of the signal transducer and the tumour microenvironment. Further studies are
and activator of transcription (STAT) protein family in needed to exploit PTEN-dependent changes, such as
prostate cancer 165. PTEN dephosphorylates interferon reduced type I interferon response and cytokine signal-
regulatory factor 3 (IRF3) and increases its nuclear ling to the tumour microenvironment and to develop
translocation, leading to increased expression of type I effective immunotherapy in prostate cancer.
interferon response genes7. By contrast, mouse embry-
onic fibroblast cells with Pten knockout have disrupted Conclusions
nuclear import, decreased activity of IRF3, and have Detection of PTEN loss in prostate cancer has tre-
reduced type I IFN response. Downstream targets of mendous potential to enhance our understanding of
IRF3 include IFNα and IFNβ28, both of which activate the biology of the disease and improve patient care.
STAT1 and STAT3 transcription factors. STAT proteins As the most commonly lost tumour suppressor in
are key to both type I and type II interferon responses, primary prostate cancer, PTEN loss is one of few
such as the induction of chemokines that recruit prognostic biomarkers that is reproducibly associ-
immune cells into the tissue microenvironment 166. ated with poor outcomes in patients with the disease.
Understanding the dynamic interaction between Easily and inexpensively measured using analytically
PTEN-deficient tumours and the immune signalling validated assays, PTEN status determination in diag-
that takes place in the tumour microenvironment is nostic biopsies might improve patient selection for AS
important for developing effective immunotherapies. and can identify patients at increased risk of disease
For example, Pten-null mouse models secrete immuno progression who could benefit from intensive defini-
suppressive senescence-associated cytokines into the tive therapies. In advanced metastatic prostate cancer,
tumour microenvironment 167. Interestingly, pharma- PTEN status can be measured in liquid biopsies. At
cological inhibition of the JAK2–STAT3 pathway can this end of the disease spectrum, further refinements
reactivate the senescence-associated cytokine net- in targeting PI3K–AKT–mTOR signalling, most likely
work, leading to an antitumour immune response that in combination with AR signalling, might be effective
enhances sensitivity to chemotherapy 167. These data sug- in subsets of patients with PTEN-deficient tumours.
gest that if the immune surveillance of senescent PTEN- Finally, emerging evidence suggests that PTEN sta-
null tumours is suppressed, specific pharmacological tus influences immune response to tumour progres-
interventions might be able to restore immunogenicity sion and has a role in predicting which patients will
to tumours. respond to promising immunotherapies. Although we
The emerging relationship between PTEN and the are clearly in the early days of molecular classification
immune system is complex and covers both protumori of prostate cancer and its application to clinical care,
genic and antitumorigenic cascades that depend on as a biomarker, PTEN is here to stay.
1. Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, insensitive to PTEN expression. J. Cell Sci. 119, 24. Pesche, S. et al. PTEN/MMAC1/TEP1 involvement in
2017. CA Cancer J. Clin. 67, 7–30 (2017). 5160–5168 (2006). primary prostate cancers. Oncogene 16, 2879–2883
2. Tosoian, J. J. et al. Intermediate and longer-term 13. Shen, W. H. et al. Essential role for nuclear PTEN in (1998).
outcomes from a prospective active-surveillance maintaining chromosomal integrity. Cell 128, 25. Wang, S. I., Parsons, R. & Ittmann, M. Homozygous
program for favorable-risk prostate cancer. J. Clin. 157–170 (2007). deletion of the PTEN tumor suppressor gene in a
Oncol. 33, 3379–3385 (2015). 14. Bassi, C. et al. Nuclear PTEN controls DNA repair and subset of prostate adenocarcinomas. Clin. Cancer Res.
3. Cancer Genome Atlas Research, N. The molecular sensitivity to genotoxic stress. Science 341, 395–399 4, 811–815 (1998).
taxonomy of primary prostate cancer. Cell 163, (2013). 26. Whang, Y. E. et al. Inactivation of the tumor
1011–1025 (2015). 15. Cairns, P. et al. Frequent inactivation of PTEN/MMAC1 suppressor PTEN/MMAC1 in advanced human
4. Taylor, B. S. et al. Integrative genomic profiling of in primary prostate cancer. Cancer Res. 57, prostate cancer through loss of expression. Proc. Natl
human prostate cancer. Cancer Cell 18, 11–22 4997–5000 (1997). Acad. Sci. USA 95, 5246–5250 (1998).
(2010). 16. Steck, P. A. et al. Identification of a candidate tumour 27. Yoshimoto, M. et al. Interphase FISH analysis of PTEN
5. Maehama, T. & Dixon, J. E. The tumor suppressor, suppressor gene, MMAC1, at chromosome 10q23.3 in histologic sections shows genomic deletions in 68%
PTEN/MMAC1, dephosphorylates the lipid second that is mutated in multiple advanced cancers. Nat. of primary prostate cancer and 23% of high-grade
messenger, phosphatidylinositol 3,4,5‑trisphosphate. Genet. 15, 356–362 (1997). prostatic intra-epithelial neoplasias. Cancer Genet.
J. Biol. Chem. 273, 13375–13378 (1998). 17. Suzuki, H. et al. Interfocal heterogeneity of PTEN/ Cytogenet. 169, 128–137 (2006).
6. Song, M. S., Salmena, L. & Pandolfi, P. P. The MMAC1 gene alterations in multiple metastatic prostate 28. Verhagen, P. C. et al. The PTEN gene in locally
functions and regulation of the PTEN tumour cancer tissues. Cancer Res. 58, 204–209 (1998). progressive prostate cancer is preferentially
suppressor. Nat. Rev. Mol. Cell Biol. 13, 283–296 18. Berger, M. F. et al. The genomic complexity of primary inactivated by bi‑allelic gene deletion. J. Pathol. 208,
(2012). human prostate cancer. Nature 470, 214–220 699–707 (2006).
7. Li, S. et al. The tumor suppressor PTEN has a critical (2011). 29. McCall, P., Witton, C. J., Grimsley, S., Nielsen, K. V. &
role in antiviral innate immunity. Nat. Immunol. 17, 19. Barbieri, C. E. et al. Exome sequencing identifies Edwards, J. Is PTEN loss associated with clinical
241–249 (2016). recurrent SPOP, FOXA1 and MED12 mutations in outcome measures in human prostate cancer? Br.
8. Chen, L. & Guo, D. The functions of tumor suppressor prostate cancer. Nat. Genet. 44, 685–689 (2012). J. Cancer 99, 1296–1301 (2008).
PTEN in innate and adaptive immunity. Cell. Mol. 20. Yoshimoto, M. et al. FISH analysis of 107 prostate 30. Yoshimoto, M. et al. Absence of TMPRSS2:ERG
Immunol. 14, 581–589 (2017). cancers shows that PTEN genomic deletion is fusions and PTEN losses in prostate cancer is
9. Tamura, M. et al. Inhibition of cell migration, associated with poor clinical outcome. Br. J. Cancer associated with a favorable outcome. Mod. Pathol. 21,
spreading, and focal adhesions by tumor suppressor 97, 678–685 (2007). 1451–1460 (2008).
PTEN. Science 280, 1614–1617 (1998). 21. Krohn, A. et al. Genomic deletion of PTEN is 31. Attard, G. et al. Characterization of ERG, AR and
10. Zhang, S. et al. Combating trastuzumab resistance by associated with tumor progression and early PSA PTEN gene status in circulating tumor cells from
targeting SRC, a common node downstream of recurrence in ERG fusion-positive and fusion-negative patients with castration-resistant prostate cancer.
multiple resistance pathways. Nat. Med. 17, prostate cancer. Am. J. Pathol. 181, 401–412 (2012). Cancer Res. 69, 2912–2918 (2009).
461–469 (2011). 22. Troyer, D. A. et al. A multicenter study shows PTEN 32. Sircar, K. et al. PTEN genomic deletion is associated
11. Weng, L. P., Brown, J. L. & Eng, C. PTEN coordinates deletion is strongly associated with seminal vesicle with p‑Akt and AR signalling in poorer outcome,
G(1) arrest by down-regulating cyclin D1 via its protein involvement and extracapsular extension in localized hormone refractory prostate cancer. J. Pathol. 218,
phosphatase activity and up‑regulating p27 via its prostate cancer. Prostate 75, 1206–1215 (2015). 505–513 (2009).
lipid phosphatase activity in a breast cancer model. 23. Feilotter, H. E., Nagai, M. A., Boag, A. H., Eng, C. & 33. Han, B. et al. Fluorescence in situ hybridization study
Hum. Mol. Genet. 10, 599–604 (2001). Mulligan, L. M. Analysis of PTEN and the 10q23 shows association of PTEN deletion with ERG
12. Lindsay, Y. et al. Localization of agonist-sensitive region in primary prostate carcinomas. Oncogene 16, rearrangement during prostate cancer progression.
PtdIns(3,4,5)P3 reveals a nuclear pool that is 1743–1748 (1998). Mod. Pathol. 22, 1083–1093 (2009).
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 11
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
34. Krohn, A. et al. Heterogeneity and chronology of 61. Gumuskaya, B. et al. Assessing the order of critical variant prostate cancers. Clin. Cancer Res. 22,
PTEN deletion and ERG fusion in prostate cancer. alterations in prostate cancer development and 1520–1530 (2016).
Mod. Pathol. 27, 1612–1620 (2014). progression by IHC: further evidence that PTEN loss 87. Hubbard, G. K. et al. Combined MYC activation and
35. Steurer, S. et al. TMPRSS2‑ERG fusions are strongly occurs subsequent to ERG gene fusion. Prostate Pten loss are sufficient to create genomic instability
linked to young patient age in low-grade prostate Cancer Prostat. Dis. 16, 209–215 (2013). and lethal metastatic prostate cancer. Cancer Res. 76,
cancer. Eur. Urol. 66, 978–981 (2014). 62. Lotan, T. L. et al. PTEN loss as determined by clinical- 283–292 (2016).
36. Lotan, T. L. et al. Analytic validation of a clinical-grade grade immunohistochemistry assay is associated with 88. Blattner, M. et al. SPOP mutation drives prostate
PTEN immunohistochemistry assay in prostate cancer worse recurrence-free survival in prostate cancer. Eur. tumorigenesis in vivo through coordinate regulation of
by comparison with PTEN FISH. Mod. Pathol. 29, Urol. Focus 2, 180–188 (2016). PI3K/mTOR and AR signaling. Cancer Cell 31,
904–914 (2016). 63. Lotan, T. L. et al. Cytoplasmic PTEN protein loss 436–451 (2017).
37. Ahearn, T. U. et al. A prospective investigation of distinguishes intraductal carcinoma of the prostate 89. Zhao, D. et al. Synthetic essentiality of chromatin
PTEN loss and ERG expression in lethal prostate from high-grade prostatic intraepithelial neoplasia. remodelling factor CHD1 in PTEN-deficient cancer.
cancer. J. Natl Cancer Inst. 108, djv34 (2016). Mod. Pathol. 26, 587–603 (2013). Nature 542, 484–488 (2017).
38. Liu, W. et al. Copy number analysis indicates 64. Morais, C. L. et al. Utility of PTEN and ERG 90. Moschini, M. et al. Low-risk prostate cancer:
monoclonal origin of lethal metastatic prostate cancer. immunostaining for distinguishing high-grade PIN identification, management, and outcomes. Eur. Urol.
Nat. Med. 15, 559–565 (2009). from intraductal carcinoma of the prostate on needle 72, 238–249 (2017).
39. Grasso, C. S. et al. The mutational landscape of lethal biopsy. Am. J. Surg. Pathol. 39, 169–178 (2015). 91. Bruinsma, S. M. et al. Active surveillance for prostate
castration-resistant prostate cancer. Nature 487, 65. Morais, C. L. et al. ERG and PTEN status of isolated cancer: a narrative review of clinical guidelines. Nat.
239–243 (2012). high-grade PIN occurring in cystoprostatectomy Rev. Urol. 13, 151–167 (2016).
40. Robinson, D. et al. Integrative clinical genomics of specimens without invasive prostatic adenocarcinoma. 92. Barrett, T. & Haider, M. A. The emerging role of MRI
advanced prostate cancer. Cell 161, 1215–1228 Hum. Pathol. 55, 117–125 (2016). in prostate cancer active surveillance and ongoing
(2015). 66. Trotman, L. C. et al. Pten dose dictates cancer challenges. AJR Am. J. Roentgenol. 208, 131–139
41. Khani, F. et al. Evidence for molecular differences in progression in the prostate. PLOS Biol. 1, E59 (2003). (2017).
prostate cancer between African American and 67. Di Cristofano, A., Pesce, B., Cordon-Cardo, C. & 93. Ma, T. M. et al. The role of multiparametric magnetic
Caucasian men. Clin. Cancer Res. 20, 4925–4934 Pandolfi, P. P. Pten is essential for embryonic resonance imaging/ultrasound fusion biopsy in active
(2014). development and tumour suppression. Nat. Genet. surveillance. Eur. Urol. 71, 174–180 (2017).
42. Tosoian, J. J. et al. Prevalence and prognostic 19, 348–355 (1998). 94. Epstein, J. I. et al. The 2014 International Society of
significance of PTEN loss in African-American and 68. Stambolic, V. et al. High incidence of breast and Urological Pathology (ISUP) Consensus Conference on
European-American men undergoing radical endometrial neoplasia resembling human Cowden Gleason Grading of Prostatic Carcinoma: definition of
prostatectomy. Eur. Urol. 71, 697–700 (2017). syndrome in pten+/− mice. Cancer Res. 60, grading patterns and proposal for a new grading
43. Lindquist, K. J. et al. Mutational landscape of 3605–3611 (2000). system. Am. J. Surg. Pathol. 40, 244–252 (2016).
aggressive prostate tumors in African American men. 69. Podsypanina, K. et al. Mutation of Pten/Mmac1 in 95. Epstein, J. I. et al. A contemporary prostate cancer
Cancer Res. 76, 1860–1868 (2016). mice causes neoplasia in multiple organ systems. Proc. grading system: a validated alternative to the Gleason
44. Huang, F. W. et al. Exome sequencing of African- Natl Acad. Sci. USA 96, 1563–1568 (1999). score. Eur. Urol. 69, 428–435 (2016).
American prostate cancer reveals loss‑of‑function ERF 70. Wang, S. et al. Prostate-specific deletion of the murine 96. Ross, A. E., D’Amico, A. V. & Freedland, S. J. Which,
mutations. Cancer Discov. 7, 973–983 (2017). Pten tumor suppressor gene leads to metastatic when and why? Rational use of tissue-based molecular
45. Reid, A. H. et al. Novel, gross chromosomal prostate cancer. Cancer Cell 4, 209–221 (2003). testing in localized prostate cancer. Prostate Cancer
alterations involving PTEN cooperate with allelic loss 71. Chen, Z. et al. Crucial role of p53‑dependent cellular Prostat. Dis. 19, 1–6 (2016).
in prostate cancer. Mod. Pathol. 25, 902–910 (2012). senescence in suppression of Pten-deficient 97. Lotan, T. L. et al. PTEN protein loss by immunostaining:
46. Murphy, S. J. et al. Integrated analysis of the genomic tumorigenesis. Nature 436, 725–730 (2005). analytic validation and prognostic indicator for a high
instability of PTEN in clinically insignificant and 72. Shen, M. M. & Abate-Shen, C. Pten inactivation and risk surgical cohort of prostate cancer patients. Clin.
significant prostate cancer. Mod. Pathol. 29, the emergence of androgen-independent prostate Cancer Res. 17, 6563–6573 (2011).
143–156 (2016). cancer. Cancer Res. 67, 6535–6538 (2007). 98. Wang, Y. & Dai, B. PTEN genomic deletion defines
47. Ibeawuchi, C. et al. Exploring prostate cancer genome 73. Jiao, J. et al. Murine cell lines derived from Pten null favorable prognostic biomarkers in localized prostate
reveals simultaneous losses of PTEN, FAS and PAPSS2 prostate cancer show the critical role of PTEN in cancer: a systematic review and meta-analysis. Int.
in patients with PSA recurrence after radical hormone refractory prostate cancer development. J. Clin. Exp. Med. 8, 5430–5437 (2015).
prostatectomy. Int. J. Mol. Sci. 16, 3856–3869 Cancer Res. 67, 6083–6091 (2007). 99. Reid, A. H. et al. Molecular characterisation of ERG,
(2015). 74. Mulholland, D. J. et al. Cell autonomous role of PTEN ETV1 and PTEN gene loci identifies patients at low
48. Whang, Y. E., Wu, X. Y. & Sawyers, C. L. Identification in regulating castration-resistant prostate cancer and high risk of death from prostate cancer. Br.
of a pseudogene that can masquerade as a mutant growth. Cancer Cell 19, 792–804 (2011). J. Cancer 102, 678–684 (2010).
allele of the PTEN/MMAC1 tumor suppressor gene. 75. Carver, B. S. et al. Reciprocal feedback regulation of 100. Trock, B. J. et al. PTEN loss and chromosome 8
J. Natl Cancer Inst. 90, 859–861 (1998). PI3K and androgen receptor signaling in PTEN- alterations in Gleason grade 3 prostate cancer cores
49. Zysman, M. A., Chapman, W. B. & Bapat, B. deficient prostate cancer. Cancer Cell 19, 575–586 predicts the presence of un‑sampled grade 4 tumor:
Considerations when analyzing the methylation status (2011). implications for active surveillance. Mod. Pathol. 29,
of PTEN tumor suppressor gene. Am. J. Pathol. 160, 76. Choucair, K. et al. PTEN genomic deletion predicts 764–771 (2016).
795–800 (2002). prostate cancer recurrence and is associated with low 101. Lotan, T. L. et al. PTEN loss is associated with
50. Beltran, H. et al. Targeted next-generation sequencing AR expression and transcriptional activity. BMC upgrading of prostate cancer from biopsy to radical
of advanced prostate cancer identifies potential Cancer 12, 543 (2012). prostatectomy. Mod. Pathol. 28, 128–137 (2015).
therapeutic targets and disease heterogeneity. Eur. 77. Bismar, T. A. et al. Interactions and relationships of 102. Picanco-Albuquerque, C. G. et al. In prostate cancer
Urol. 63, 920–926 (2013). PTEN, ERG, SPINK1 and AR in castration-resistant needle biopsies, detections of PTEN loss by
51. Bermudez Brito, M., Goulielmaki, E. & prostate cancer. Histopathology 60, 645–652 fluorescence in situ hybridization (FISH) and by
Papakonstanti, E. A. Focus on PTEN Regulation. Front. (2012). immunohistochemistry (IHC) are concordant and show
Oncol. 5, 166 (2015). 78. Grabowska, M. M. et al. Mouse models of prostate consistent association with upgrading. Virchows Arch.
52. Garcia, J. M. et al. Promoter methylation of the PTEN cancer: picking the best model for the question. 468, 607–617 (2016).
gene is a common molecular change in breast cancer. Cancer Metastasis Rev. 33, 377–397 (2014). 103. Guedes, L. B., Tosoian, J. J., Hicks, J., Ross, A. E. &
Genes Chromosomes Cancer 41, 117–124 (2004). 79. Carver, B. S. et al. Aberrant ERG expression Lotan, T. L. PTEN loss in Gleason score 3 + 4 = 7
53. Konishi, N. et al. Heterogeneous methylation and cooperates with loss of PTEN to promote cancer prostate biopsies is associated with nonorgan confined
deletion patterns of the INK4a/ARF locus within progression in the prostate. Nat. Genet. 41, 619–624 disease at radical prostatectomy. J. Urol. 197,
prostate carcinomas. Am. J. Pathol. 160, 1207–1214 (2009). 1054–1059 (2017).
(2002). 80. King, J. C. et al. Cooperativity of TMPRSS2‑ERG with 104. Lokman, U., Erickson, A. M., Vasarainen, H.,
54. Tay, Y. et al. Coding-independent regulation of the PI3‑kinase pathway activation in prostate oncogenesis. Rannikko, A. S. & Mirtti, T. PTEN loss but not ERG
tumor suppressor PTEN by competing endogenous Nat. Genet. 41, 524–526 (2009). expression in diagnostic biopsies is associated with
mRNAs. Cell 147, 344–357 (2011). 81. Chen, Y. et al. ETS factors reprogram the androgen increased risk of progression and adverse surgical
55. Poliseno, L. et al. Identification of the miR‑106b~25 receptor cistrome and prime prostate tumorigenesis in findings in men with prostate cancer on active
microRNA cluster as a proto-oncogenic PTEN- response to PTEN loss. Nat. Med. 19, 1023–1029 surveillance. Eur. Urol. Focus https://doi.
targeting intron that cooperates with its host gene (2013). org/10.1016/j.euf.2017.03.004 (2017).
MCM7 in transformation. Sci. Signal. 3, ra29 (2010). 82. Kim, J. et al. A mouse model of heterogeneous, 105. Mithal, P. et al. PTEN loss in biopsy tissue predicts
56. Leslie, N. R. & Foti, M. Non-genomic loss of PTEN c‑MYC-initiated prostate cancer with loss of Pten and poor clinical outcomes in prostate cancer. Int. J. Urol.
function in cancer: not in my genes. Trends Pharmacol. p53. Oncogene 31, 322–332 (2012). 21, 1209–1214 (2014).
Sci. 32, 131–140 (2011). 83. Couto, S. S. et al. Simultaneous haploinsufficiency of 106. Shah, R. B., Bentley, J., Jeffery, Z. & DeMarzo, A. M.
57. Salmena, L., Carracedo, A. & Pandolfi, P. P. Tenets of Pten and Trp53 tumor suppressor genes accelerates Heterogeneity of PTEN and ERG expression in
PTEN tumor suppression. Cell 133, 403–414 (2008). tumorigenesis in a mouse model of prostate cancer. prostate cancer on core needle biopsies: implications
58. Gundem, G. et al. The evolutionary history of lethal Differentiation 77, 103–111 (2009). for cancer risk stratification and biomarker sampling.
metastatic prostate cancer. Nature 520, 353–357 84. Ku, S. Y. et al. Rb1 and Trp53 cooperate to suppress Hum. Pathol. 46, 698–706 (2015).
(2015). prostate cancer lineage plasticity, metastasis, and 107. Wobker, S. E. & Epstein, J. I. Differential diagnosis of
59. Haffner, M. C. et al. Tracking the clonal origin of lethal antiandrogen resistance. Science 355, 78–83 (2017). intraductal lesions of the prostate. Am. J. Surg. Pathol.
prostate cancer. J. Clin. Invest. 123, 4918–4922 85. Tan, H. L. et al. Rb loss is characteristic of prostatic 40, e67–e82 (2016).
(2013). small cell neuroendocrine carcinoma. Clin. Cancer Res. 108. Epstein, J. I. & Herawi, M. Prostate needle biopsies
60. Bismar, T. A. et al. PTEN genomic deletion is an early 20, 890–903 (2014). containing prostatic intraepithelial neoplasia or
event associated with ERG gene rearrangements in 86. Aparicio, A. M. et al. Combined tumor suppressor atypical foci suspicious for carcinoma: implications for
prostate cancer. BJU Int. 107, 477–485 (2011). defects characterize clinically defined aggressive patient care. J. Urol. 175, 820–834 (2006).
12 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
109. Tosoian, J. J., Alam, R., Ball, M. W., Carter, H. B. & 130. US National Library of Medicine. ClinicalTrials.gov 154. van de Ven, A. L. et al. Nanoformulation of olaparib
Epstein, J. I. Managing high-grade prostatic https://clinicaltrials.gov/ct2/show/NCT02269982 amplifies PARP inhibition and sensitizes PTEN/
intraepithelial neoplasia (HGPIN) and atypical glands (2018). TP53‑deficient prostate cancer to radiation. Mol.
on prostate biopsy. Nat. Rev. Urol. 15, 55–66 131. Ferraldeschi, R. et al. PTEN protein loss and clinical Cancer Ther. 16, 1279–1289 (2017).
(2018). outcome from castration-resistant prostate cancer 155. Hopkins, B. D. et al. A secreted PTEN phosphatase
110. Guo, C. C. & Epstein, J. I. Intraductal carcinoma of the treated with abiraterone acetate. Eur. Urol. 67, that enters cells to alter signaling and survival. Science
prostate on needle biopsy: histologic features and 795–802 (2015). 341, 399–402 (2013).
clinical significance. Mod. Pathol. 19, 1528–1535 132. Edlind, M. P. & Hsieh, A. C. PI3K‑AKT-mTOR signaling 156. Wang, H. et al. Relevance and therapeutic possibility
(2006). in prostate cancer progression and androgen of PTEN-long in renal cell carcinoma. PLOS One 10,
111. Robinson, B. D. & Epstein, J. I. Intraductal carcinoma deprivation therapy resistance. Asian J. Androl. 16, e114250 (2015).
of the prostate without invasive carcinoma on needle 378–386 (2014). 157. Drake, C. G. Immunotherapy for prostate cancer: an
biopsy: emphasis on radical prostatectomy findings. 133. Dillon, L. M. & Miller, T. W. Therapeutic targeting of emerging treatment modality. Urol. Clin. North Am.
J. Urol. 184, 1328–1333 (2010). cancers with loss of PTEN function. Curr. Drug Targets 37, 121–129 (2010).
112. Hickman, R. A. et al. Atypical intraductal cribriform 15, 65–79 (2014). 158. De Marzo, A. M. et al. Inflammation in prostate
proliferations of the prostate exhibit similar molecular 134. Thomas, C. et al. Synergistic targeting of PI3K/AKT carcinogenesis. Nat. Rev. Cancer 7, 256–269 (2007).
and clinicopathologic characteristics as intraductal pathway and androgen receptor axis significantly 159. Strasner, A. & Karin, M. Immune infiltration and
carcinoma of the prostate. Am. J. Surg. Pathol. 41, delays castration-resistant prostate cancer prostate cancer. Front. Oncol. 5, 128 (2015).
550–556 (2017). progression in vivo. Mol. Cancer Ther. 12, 160. Gannon, P. O. et al. Characterization of the intra-
113. De Marzo, A. M., Haffner, M. C., Lotan, T. L., 2342–2355 (2013). prostatic immune cell infiltration in androgen-deprived
Yegnasubramanian, S. & Nelson, W. G. Premalignancy 135. Marques, R. B. et al. High efficacy of combination prostate cancer patients. J. Immunol. Methods 348,
in prostate cancer: rethinking what we know. Cancer therapy using PI3K/AKT inhibitors with androgen 9–17 (2009).
Prev. Res. 9, 648–656 (2016). deprivation in prostate cancer preclinical models. Eur. 161. Si, T. G., Wang, J. P. & Guo, Z. Analysis of circulating
114. Pettersson, A. et al. The TMPRSS2:ERG Urol. 67, 1177–1185 (2015). regulatory T cells (CD4+CD25+CD127-) after
rearrangement, ERG expression, and prostate cancer 136. Schwartz, S. et al. Feedback suppression of PI3Kalpha cryosurgery in prostate cancer. Asian J. Androl. 15,
outcomes: a cohort study and meta-analysis. Cancer signaling in PTEN-mutated tumors is relieved by 461–465 (2013).
Epidemiol. Biomarkers Prev. 21, 1497–1509 selective inhibition of PI3Kbeta. Cancer Cell 27, 162. Peng, W. et al. Loss of PTEN promotes resistance to T
EPI‑12‑0042 (2012). 109–122 (2015). cell-mediated immunotherapy. Cancer Discov. 6,
115. Leinonen, K. A. et al. Loss of PTEN is associated with 137. Armstrong, A. J. et al. Phase II trial of the PI3 kinase 202–216 (2016).
aggressive behavior in ERG-positive prostate cancer. inhibitor buparlisib (BKM‑120) with or without 163. Moussavi, M. et al. Oncolysis of prostate cancers
Cancer Epidemiol. Biomarkers Prev. 22, 2333–2344 enzalutamide in men with metastatic castration induced by vesicular stomatitis virus in PTEN knockout
(2013). resistant prostate cancer. Eur. J. Cancer 81, 228–236 mice. Cancer Res. 70, 1367–1376 (2010).
116. Fontugne, J. et al. Recurrent prostate cancer genomic (2017). 164. Champion, B. R., Fisher, K. & Seymour, L. A. PTENtial
alterations predict response to brachytherapy 138. Wei, X. X. et al. A phase I study of abiraterone acetate cause for the selectivity of oncolytic viruses? Nat.
treatment. Cancer Epidemiol. Biomarkers Prev. 23, combined with BEZ235, a dual PI3K/mTOR inhibitor, Immunol. 17, 225–226 (2016).
594–600 (2014). in metastatic castration resistant prostate cancer. 165. Pencik, J. et al. STAT3 regulated ARF expression
117. Lahdensuo, K. et al. Loss of PTEN expression in ERG- Oncol. 22, e503–e543 (2017). suppresses prostate cancer metastasis. Nat. Commun.
negative prostate cancer predicts secondary therapies 139. Massard, C. et al. Phase Ib dose-finding study of 6, 7736 (2015).
and leads to shorter disease-specific survival time abiraterone acetate plus buparlisib (BKM120) or 166. Yu, H., Pardoll, D. & Jove, R. STATs in cancer
after radical prostatectomy. Mod. Pathol. 29, dactolisib (BEZ235) in patients with castration-resistant inflammation and immunity: a leading role for STAT3.
1565–1574 (2016). prostate cancer. Eur. J. Cancer 76, 36–44 (2017). Nat. Rev. Cancer 9, 798–809 (2009).
118. Yoshimoto, M. et al. PTEN genomic deletions that 140. Chow, H. et al. A phase 2 clinical trial of everolimus 167. Toso, A. et al. Enhancing chemotherapy efficacy in
characterize aggressive prostate cancer originate close plus bicalutamide for castration-resistant prostate Pten-deficient prostate tumors by activating the
to segmental duplications. Genes Chromosomes cancer. Cancer 122, 1897–1904 (2016). senescence-associated antitumor immunity. Cell Rep.
Cancer 51, 149–160 (2012). 141. US National Library of Medicine. ClinicalTrials.gov 9, 75–89 (2014).
119. Yoshimoto, M. et al. Incorporation of flanking probes https://clinicaltrials.gov/ct2/show/NCT02106507 168. Cuzick, J. et al. Prognostic value of PTEN loss in men
reduces truncation losses for fluorescence in situ (2017). with conservatively managed localised prostate
hybridization analysis of recurrent genomic deletions 142. US National Library of Medicine. ClinicalTrials.gov cancer. Br. J. Cancer 108, 2582–2589 (2013).
in tumor sections [abstract]. Cancer Res. 73, 63 https://clinicaltrials.gov/ct2/show/NCT02125084 169. Lotan, T. L. et al. PTEN loss detection in prostate
(2014). (2017). cancer: comparison of PTEN immunohistochemistry
120. Sangale, Z. et al. A robust immunohistochemical assay 143. Baselga, J. et al. Everolimus in postmenopausal and PTEN FISH in a large retrospective prostatectomy
for detecting PTEN expression in human tumors. Appl. hormone-receptor-positive advanced breast cancer. cohort. Oncotarget 8, 65566–65576 (2017).
Immunohistochem. Mol. Morphol. 19, 173–183 N. Engl. J. Med. 366, 520–529 (2012).
(2011). 144. US National Library of Medicine. ClinicalTrials.gov Acknowledgements
121. Chaux, A. et al. Loss of PTEN expression is associated https://clinicaltrials.gov/ct2/show/NCT02833883 Funding for this research was provided in part by a
with increased risk of recurrence after prostatectomy (2017). Transformative Impact Award from the Congressionally
for clinically localized prostate cancer. Mod. Pathol. 145. US National Library of Medicine. ClinicalTrials.gov Directed Medical Research Program–Prostate Cancer
25, 1543–1549 (2012). https://clinicaltrials.gov/ct2/show/NCT01485861 Research Program (CDMRP-PCRP) (W81XWH‑13‑2‑0070,
122. Punnoose, E. A. et al. PTEN loss in circulating tumour (2018). H.I.S. and T.L.L.). T.L.L. was additionally supported by the NIH
cells correlates with PTEN loss in fresh tumour tissue 146. de Bono, J. S. et al. PTEN loss as a predictive and National Cancer Institute (NCI) P30 Cancer Center
from castration-resistant prostate cancer patients. Br. biomarker for the Akt inhibitor ipatasertib combined Support Grant CA006973 and the Patrick Walsh Prostate
J. Cancer 113, 1225–1233 (2015). with abiraterone acetate in patients with metastatic Cancer Research Fund. H.I.S. was additionally supported by
123. Wyatt, A. W. et al. Genomic alterations in cell-free castration-resistant prostate cancer (mCRPC). Ann. NIH and NCI Prostate SPORE Grant P50‑CA92629, NIH and
DNA and enzalutamide resistance in castration- Oncol. 27, 718O (2016). NCI P30 Cancer Center Support Grant CA008748, and the
resistant prostate cancer. JAMA Oncol. 2, 147. Fruman, D. A. et al. The PI3K pathway in human Prostate Cancer Foundation. T.J. and D.M.B. were funded by
1598–1606 (2016). disease. Cell 170, 605–635 (2017). Prostate Cancer Canada and the Movember Foundation
124. Xia, Y. et al. Copy number variations in urine cell free 148. Jia, S. et al. Essential roles of PI(3)K-p110beta in cell (Grant #T2014‑01‑PRONTO). T.J. was supported by a
DNA as biomarkers in advanced prostate cancer. growth, metabolism and tumorigenesis. Nature 454, Transformative Pathology Fellowship funded by the Ontario
Oncotarget 7, 35818–35831 (2016). 776–779 (2008). Institute for Cancer Research through funding provided by
125. Wyatt, A. W. et al. Concordance of circulating tumor 149. US National Library of Medicine. ClinicalTrials.gov the Government of Ontario.
DNA and matched metastatic tissue biopsy in https://clinicaltrials.gov/ct2/show/NCT01884285
prostate cancer. J. Natl Cancer Inst. 110, 78–86 (2018). Author contributions
(2017). 150. US National Library of Medicine. ClinicalTrials.gov All authors researched data for the article, took part in dis-
126. US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/NCT02215096 cussions of the content, and wrote the manuscript. T.J.,
https://clinicaltrials.gov/ct2/show/NCT03236688 (2018). D.M.B., H.I.S., A.M.D.M., J.A.S., and T.L.L. reviewed and
(2017). 151. Mateo, J. et al. DNA repair in prostate cancer: biology edited the manuscript before submission.
127. US National Library of Medicine. ClinicalTrials.gov and clinical implications. Eur. Urol. 71, 417–425
https://clinicaltrials.gov/ct2/show/NCT02438007 (2017). Competing interests
(2017). 152. Mateo, J. et al. DNA-repair defects and olaparib in T.L.L. has received research support from Ventana Medical
128. US National Library of Medicine. ClinicalTrials.gov metastatic prostate cancer. N. Engl. J. Med. 373, Systems. D.M.B. has received financial support from Myriad
https://clinicaltrials.gov/ct2/show/NCT03050866 1697–1708 (2015). Genetics and Metamark Genetics.
(2017). 153. Gonzalez-Billalabeitia, E. et al. Vulnerabilities of
129. US National Library of Medicine. ClinicalTrials.gov PTEN‑TP53‑deficient prostate cancers to compound Publisher’s note
https://clinicaltrials.gov/ct2/show/NCT02853097 PARP‑PI3K inhibition. Cancer Discov. 4, 896–904 Springer Nature remains neutral with regard to jurisdictional
(2017). (2014). claims in published maps and institutional affiliations.
NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 13
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
Вам также может понравиться
- Oligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Документ11 страницOligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Orlando SotoОценок пока нет
- Reviews: Marked For Death: Targeting Epigenetic Changes in CancerДокумент23 страницыReviews: Marked For Death: Targeting Epigenetic Changes in CancerLorena RamosОценок пока нет
- Feinberg AP Et Al. 2016 Epigenetic Modulators, Modifiers and Mediators in Cancer Aetiology and ProgressionДокумент16 страницFeinberg AP Et Al. 2016 Epigenetic Modulators, Modifiers and Mediators in Cancer Aetiology and ProgressionJasmyn KimОценок пока нет
- MacrophagesДокумент18 страницMacrophagesSaif WahidОценок пока нет
- Reviews: Computational Genomics Tools For Dissecting Tumour-Immune Cell InteractionsДокумент18 страницReviews: Computational Genomics Tools For Dissecting Tumour-Immune Cell Interactionsdata lmleОценок пока нет
- Loss-Of-Function Genetic Tools For Animal Models - Cross-Species and Cross-Platform DifferencesДокумент17 страницLoss-Of-Function Genetic Tools For Animal Models - Cross-Species and Cross-Platform DifferencesLeon PalomeraОценок пока нет
- Renal CellДокумент10 страницRenal CellEss liОценок пока нет
- Nrclinonc 2017 95Документ13 страницNrclinonc 2017 95김현수Оценок пока нет
- Cancers Prostate ScreeningДокумент12 страницCancers Prostate ScreeningMed. TrackОценок пока нет
- Primer. Vejiga. 2017Документ19 страницPrimer. Vejiga. 2017Isabel Gago CastilloОценок пока нет
- Targeting Neoantigens To Augment Antitumour ImmunityДокумент14 страницTargeting Neoantigens To Augment Antitumour Immunitylaura isabellaОценок пока нет
- Engineering and Physical Sciences in Oncology - Challenges and OpportunitiesДокумент17 страницEngineering and Physical Sciences in Oncology - Challenges and OpportunitiesAlessandroОценок пока нет
- Paper TranscripcionДокумент13 страницPaper TranscripcionKarime MontenegroОценок пока нет
- Genetic-Guidedrisk Assessmentand Managementofthyroidcancer: Mingzhao XingДокумент16 страницGenetic-Guidedrisk Assessmentand Managementofthyroidcancer: Mingzhao XingPedro Gómez RОценок пока нет
- Kellum 2018Документ14 страницKellum 2018hemer hadyn calderon alvitesОценок пока нет
- Inequality in MedicineДокумент2 страницыInequality in MedicineSezen DemirhanОценок пока нет
- 10 1038@nrneph 2017 85 PDFДокумент13 страниц10 1038@nrneph 2017 85 PDFSirGonzОценок пока нет
- DownloadДокумент12 страницDownloadhasan nazzalОценок пока нет
- NeuroblastomaДокумент21 страницаNeuroblastomaRichard DjigoОценок пока нет
- Tumor Immune Microenvironment in Cancer Progression and Cancer TherapyОт EverandTumor Immune Microenvironment in Cancer Progression and Cancer TherapyPawel KalinskiОценок пока нет
- MMP in MetastasisДокумент7 страницMMP in Metastasistasnishapeer15Оценок пока нет
- Membranosa 2Документ17 страницMembranosa 2Carolina CastroОценок пока нет
- NRD 2016 211Документ14 страницNRD 2016 211김승훈(이과대학 화학)Оценок пока нет
- d41586 017 07689 5 PDFДокумент2 страницыd41586 017 07689 5 PDFTI MkОценок пока нет
- Primer: HypoparathyroidismДокумент20 страницPrimer: HypoparathyroidismKarenОценок пока нет
- Hepatocarcinoma 2Документ23 страницыHepatocarcinoma 2NaraMayhumiDeBelenMerinoOrtizОценок пока нет
- Metaplasia. Nature ReviewsДокумент11 страницMetaplasia. Nature ReviewsCamila RodríguezОценок пока нет
- Integration Site Selection by Retroviruses and Transposable Elements in EukaryotesДокумент17 страницIntegration Site Selection by Retroviruses and Transposable Elements in EukaryotesLuis ZabalaОценок пока нет
- Hormona Tiroidea y Sistema Cardiovascular - Nature 2017Документ17 страницHormona Tiroidea y Sistema Cardiovascular - Nature 2017Cristian MuñozОценок пока нет
- A Triumvirate Correlating Thyroid Cytopathology Mole 2023 Surgical PatholДокумент14 страницA Triumvirate Correlating Thyroid Cytopathology Mole 2023 Surgical PatholrubenmacaОценок пока нет
- Ijo 40 6 1889 PDFДокумент11 страницIjo 40 6 1889 PDFshovonОценок пока нет
- Otto 2017Документ23 страницыOtto 2017yankusumaОценок пока нет
- NRDP 201755Документ21 страницаNRDP 201755Hussein El-SanabaryОценок пока нет
- Hormonas Tiroideas y Enfermedades Cardiovasculares Nature, 2016Документ17 страницHormonas Tiroideas y Enfermedades Cardiovasculares Nature, 2016Ruber Ballesteros LoraОценок пока нет
- Epigenetic Modulations and Lineage Plasticity in Advanced Prostate CancerДокумент10 страницEpigenetic Modulations and Lineage Plasticity in Advanced Prostate CancerGabriel ŞarguОценок пока нет
- Articulo ElegioДокумент12 страницArticulo ElegioAna LarrabeitiОценок пока нет
- Ya EstasДокумент19 страницYa EstasMedranoReyesLuisinОценок пока нет
- A Network-Biology Perspective of MicroRNA Function and Dysfunction in CancerДокумент14 страницA Network-Biology Perspective of MicroRNA Function and Dysfunction in CancerRicardo GoreОценок пока нет
- Blood Based Biomarkers For MelanomaДокумент2 страницыBlood Based Biomarkers For MelanomaMichael MooreОценок пока нет
- Modelling Diabetic Nephropathy in MiceДокумент9 страницModelling Diabetic Nephropathy in MiceKarina ThiemeОценок пока нет
- Dermal Transmission Examination Associated With Paclitaxel Within an Ex Girlfriend or Boyfriend Vivo Porcine Headsets Model Making Use of Epifluorescence Microscopy as Well as Digital Graphic DigestingqolvvДокумент2 страницыDermal Transmission Examination Associated With Paclitaxel Within an Ex Girlfriend or Boyfriend Vivo Porcine Headsets Model Making Use of Epifluorescence Microscopy as Well as Digital Graphic Digestingqolvvjoinfile8Оценок пока нет
- J Jbior 2017 10 010 PDFДокумент20 страницJ Jbior 2017 10 010 PDF肖茹雪Оценок пока нет
- PTEN Loss in Gleason Grade 7 Prostate Tumors Exhibits Intratumoral Heterogeneity and Is Associated With Unfavorable Pathological FeaturesДокумент6 страницPTEN Loss in Gleason Grade 7 Prostate Tumors Exhibits Intratumoral Heterogeneity and Is Associated With Unfavorable Pathological FeaturesAnnaoОценок пока нет
- Nature - Antithrombotic Therapy For PatientsДокумент19 страницNature - Antithrombotic Therapy For PatientsMatheus Augusto Salerno Miguel e SousaОценок пока нет
- Unexplored Therapeutic Opportunities in The Human GenomeДокумент16 страницUnexplored Therapeutic Opportunities in The Human GenomeTony ChengОценок пока нет
- CCDT Cancer ProteomicsДокумент37 страницCCDT Cancer ProteomicsRakesh InnovationsAnd SolutionsInstituteОценок пока нет
- Smolen2018 PDFДокумент23 страницыSmolen2018 PDFJose Correa100% (1)
- Orton 1996Документ1 страницаOrton 1996Felipe Carvajal VillarroelОценок пока нет
- Molecular Mechanism of Triple Negative Breast Cancer Associated BRCA1 and The Identification of Signaling PathwaysДокумент10 страницMolecular Mechanism of Triple Negative Breast Cancer Associated BRCA1 and The Identification of Signaling PathwaysnagarajharishОценок пока нет
- Unraveling the Complexities of Metastasis: Transition from a Segmented View to a Conceptual ContinuumОт EverandUnraveling the Complexities of Metastasis: Transition from a Segmented View to a Conceptual ContinuumAmmad Ahmad FarooqiОценок пока нет
- @@@tumor MarkersДокумент6 страниц@@@tumor Markers918832Оценок пока нет
- Symmetric Dimethylarginine Concentrations Inside Puppies With Thyroid Problems Pre and Post Treatement Together With Levothyroxineqlpvr PDFДокумент1 страницаSymmetric Dimethylarginine Concentrations Inside Puppies With Thyroid Problems Pre and Post Treatement Together With Levothyroxineqlpvr PDFcolorhot0Оценок пока нет
- Reviews: Proton-Pump Inhibitors: Understanding The Complications and RisksДокумент14 страницReviews: Proton-Pump Inhibitors: Understanding The Complications and RisksRONALD. D VIERA .MОценок пока нет
- A Systematic Review and Meta Analysis 1625134013Документ13 страницA Systematic Review and Meta Analysis 1625134013bannour_Оценок пока нет
- tmp2977 TMPДокумент7 страницtmp2977 TMPFrontiersОценок пока нет
- A New Emerging Picoscale BiotechnologyДокумент194 страницыA New Emerging Picoscale BiotechnologyRakesh SharmaОценок пока нет
- Molecular Pathogenesis and Mechanisms of Thyroid Cancer: Mingzhao XingДокумент16 страницMolecular Pathogenesis and Mechanisms of Thyroid Cancer: Mingzhao XingTaeyomiОценок пока нет
- Para This Fibromin That The Role of CDC73 in Parathyr 2023 Surgical PatholДокумент9 страницPara This Fibromin That The Role of CDC73 in Parathyr 2023 Surgical PatholrubenmacaОценок пока нет
- The Oncologist 2010 Melck 1285 93Документ11 страницThe Oncologist 2010 Melck 1285 93Enda RafiqohОценок пока нет
- Tumor Heterogeneity and Therapy Resistance - Implications For Future Treatments of Prostate CancerДокумент13 страницTumor Heterogeneity and Therapy Resistance - Implications For Future Treatments of Prostate Cancermedp7060Оценок пока нет
- Tumour Heterogeneity and Resistance To Cancer TherapiesДокумент14 страницTumour Heterogeneity and Resistance To Cancer Therapiesmedp7060Оценок пока нет
- Regulatory T Cells - A Potential Target in Cancer ImmunotherapyДокумент12 страницRegulatory T Cells - A Potential Target in Cancer Immunotherapymedp7060Оценок пока нет
- Targeting MYC in Multiple MyelomaДокумент12 страницTargeting MYC in Multiple Myelomamedp7060Оценок пока нет
- ANOVA - Analysis of Variance (Slides)Документ41 страницаANOVA - Analysis of Variance (Slides)medp7060Оценок пока нет
- Evidence Based Oncology Aug EBO 2017Документ44 страницыEvidence Based Oncology Aug EBO 2017medp7060Оценок пока нет
- Cancer Biomarkers and Targeted TherapiesДокумент2 страницыCancer Biomarkers and Targeted Therapiesmedp7060Оценок пока нет
- Antibody Therapy Against Cancer MM PDFДокумент10 страницAntibody Therapy Against Cancer MM PDFpaОценок пока нет
- Bi123 - The Biology of CancerДокумент5 страницBi123 - The Biology of Cancermedp7060Оценок пока нет
- Course Syllabus For "BIO404: Cancer Biology"Документ5 страницCourse Syllabus For "BIO404: Cancer Biology"medp7060Оценок пока нет
- Nir 3876Документ1 страницаNir 3876Sarita RawatОценок пока нет
- Department of Cancer BiologyДокумент2 страницыDepartment of Cancer Biologymedp7060Оценок пока нет
- The Human Caspase-2 Gene Alternative Promoters, Pre-mRNA Splicing and AUG Usage Direct Isoform-Specific ExpressionДокумент12 страницThe Human Caspase-2 Gene Alternative Promoters, Pre-mRNA Splicing and AUG Usage Direct Isoform-Specific Expressionmedp7060Оценок пока нет
- Epidermal Growth Factors and CancerДокумент2 страницыEpidermal Growth Factors and Cancermedp7060Оценок пока нет
- Trastuzumab Cardiotoxicity in Early-Stage Breast CancerДокумент1 страницаTrastuzumab Cardiotoxicity in Early-Stage Breast Cancermedp7060Оценок пока нет
- Identification of Human Gene Core Promoters in SilicoДокумент9 страницIdentification of Human Gene Core Promoters in Silicomedp7060Оценок пока нет
- Targeting HER2 For The Treatment of Breast CancerДокумент21 страницаTargeting HER2 For The Treatment of Breast Cancermedp7060Оценок пока нет
- Better Together Targeted Combination Therapies in Breast CancerДокумент9 страницBetter Together Targeted Combination Therapies in Breast Cancermedp7060Оценок пока нет
- NatureДокумент3 страницыNatureSharad ShresthaОценок пока нет
- Breast Cancer and Environment - Breast Cancer ActionДокумент5 страницBreast Cancer and Environment - Breast Cancer Actionmedp7060Оценок пока нет
- Wind Windy Weather - ExersicesДокумент1 страницаWind Windy Weather - Exersicesmedp7060Оценок пока нет
- Wind Types of Wind Storm WindsДокумент1 страницаWind Types of Wind Storm Windsmedp7060Оценок пока нет
- Classroom AbusesДокумент6 страницClassroom AbusesJulius de la CruzОценок пока нет
- Nestle Assignement 1Документ10 страницNestle Assignement 1Saqib HanifОценок пока нет
- Format Data Kpps CilelesДокумент181 страницаFormat Data Kpps CilelesRizky OktaviaОценок пока нет
- Abnormal Psychology TestДокумент19 страницAbnormal Psychology TestJona MaeОценок пока нет
- West Philippine SeaДокумент4 страницыWest Philippine SeaFrancheskalane ValenciaОценок пока нет
- Ges New Jhs Syllabus Career Technology CCP Curriculum For b7 b10 Draft ZeroДокумент367 страницGes New Jhs Syllabus Career Technology CCP Curriculum For b7 b10 Draft ZeroElvis Adjei Yamoah100% (1)
- 1849055947Документ194 страницы1849055947Andrej Hodonj100% (1)
- Week 3 Assignment: Lab: Due Sunday by 11:59pmДокумент7 страницWeek 3 Assignment: Lab: Due Sunday by 11:59pmEssay NationОценок пока нет
- CH 4&5 QuestionsДокумент4 страницыCH 4&5 QuestionsRajender KittuОценок пока нет
- Title First - Name Last - Name Date - of - Birth Gender Mobile - Number EmailДокумент26 страницTitle First - Name Last - Name Date - of - Birth Gender Mobile - Number EmailUndergraduate LibraryОценок пока нет
- Ardyss Product CatalogДокумент32 страницыArdyss Product CatalogrolandakjonesОценок пока нет
- What Does TOTAPS Stand For? Touch, ObserveДокумент4 страницыWhat Does TOTAPS Stand For? Touch, ObserveMohd Shafuan33% (3)
- Orthodontics & Dentofacial Orthopaedics: Page 1 of 24Документ24 страницыOrthodontics & Dentofacial Orthopaedics: Page 1 of 24Abdul MohaiminОценок пока нет
- LR SDL - 21. Allen2017Документ6 страницLR SDL - 21. Allen2017Anggita Nandya ArdiatiОценок пока нет
- Entry 3 Reading Sample Paper 1 CA v3 Dec17Документ10 страницEntry 3 Reading Sample Paper 1 CA v3 Dec17lilalilak0% (1)
- Phys113 Notes 9Документ4 страницыPhys113 Notes 9Manuel DiazОценок пока нет
- Final Graduation ListДокумент108 страницFinal Graduation ListJonn MashОценок пока нет
- The Social-Emotional Functioning of YoungДокумент13 страницThe Social-Emotional Functioning of YoungKELLY LIEW VUN NIE STUDENTОценок пока нет
- Stok 16 Juni 2023Документ62 страницыStok 16 Juni 2023Icha FransiscaОценок пока нет
- Master Youtube: WorkbookДокумент64 страницыMaster Youtube: WorkbookLucian TrandafirОценок пока нет
- Assessment Task 3 Collaborative Alliances Plan TemplateДокумент2 страницыAssessment Task 3 Collaborative Alliances Plan TemplateAhmer100% (1)
- Adaptation of Smartphone Addiction ScaleДокумент20 страницAdaptation of Smartphone Addiction Scalechelito93Оценок пока нет
- Fundamentals Mt1 Nov 2023Документ16 страницFundamentals Mt1 Nov 2023Rika MaeОценок пока нет
- 1.8 Annex 4 - BOPIS DCF FORM 2-DДокумент2 страницы1.8 Annex 4 - BOPIS DCF FORM 2-DAida TagaroОценок пока нет
- ResearchДокумент14 страницResearchShannel SanzОценок пока нет
- Practical Guideline in Office Hysteroscopy SEGiДокумент95 страницPractical Guideline in Office Hysteroscopy SEGiMarcus MenezesОценок пока нет
- CrossCulture TaskPerformanceДокумент3 страницыCrossCulture TaskPerformanceMarianne DimsОценок пока нет
- Review On Contact Tracing With Machine LearningДокумент4 страницыReview On Contact Tracing With Machine LearningInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Adult Health Nursing II Laboratory Course Syllabus 2020-2021Документ52 страницыAdult Health Nursing II Laboratory Course Syllabus 2020-2021Hajer Alowaisi100% (1)
- Chapter 25Документ27 страницChapter 25Kriana RosalesОценок пока нет