Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Shoji 2019Документ7 страницShoji 2019paulineОценок пока нет
- Strategy For Nasal Reconstruction in Atypical FaciДокумент6 страницStrategy For Nasal Reconstruction in Atypical FacipaulineОценок пока нет
- SBH - Moratorium 2021Документ15 страницSBH - Moratorium 2021paulineОценок пока нет
- Opening & Healing (v2) - 1Документ26 страницOpening & Healing (v2) - 1paulineОценок пока нет
- 2021 Census in Charge-1Документ1 страница2021 Census in Charge-1paulineОценок пока нет
- How To Analyse REITs (Real Estate Investment Trusts)Документ10 страницHow To Analyse REITs (Real Estate Investment Trusts)paulineОценок пока нет
- Identification of Facial Nerve During Parotidectomy: A Combined Anatomical & Surgical StudyДокумент6 страницIdentification of Facial Nerve During Parotidectomy: A Combined Anatomical & Surgical Studyvipul51190Оценок пока нет
- Morning: Agong Decrees Parliament Should Reconvene Before Aug 1Документ25 страницMorning: Agong Decrees Parliament Should Reconvene Before Aug 1paulineОценок пока нет
- Surgical Education: Neck Dissection: Shaheel Chummun, N.R. Mclean, Maniram RagbirДокумент14 страницSurgical Education: Neck Dissection: Shaheel Chummun, N.R. Mclean, Maniram RagbirpaulineОценок пока нет
- Salah Rubayi (Auth.) - Reconstructive Plastic Surgery of Pressure Ulcers-Springer-Verlag Berlin Heidelberg (2015)Документ291 страницаSalah Rubayi (Auth.) - Reconstructive Plastic Surgery of Pressure Ulcers-Springer-Verlag Berlin Heidelberg (2015)paulineОценок пока нет
- Flap Physiology HKCДокумент40 страницFlap Physiology HKCpaulineОценок пока нет
- FLAP ANNA EditedДокумент35 страницFLAP ANNA EditedpaulineОценок пока нет
- Specialty Scissors For Plastic Surgery ProcedureДокумент16 страницSpecialty Scissors For Plastic Surgery ProcedurepaulineОценок пока нет
- Basic Surgical Skills Pauline 1Документ68 страницBasic Surgical Skills Pauline 1paulineОценок пока нет
- DrainsДокумент19 страницDrainspaulineОценок пока нет
- Suture Knots and TechniqueДокумент13 страницSuture Knots and TechniquepaulineОценок пока нет
- Flap Physiology HKCДокумент40 страницFlap Physiology HKCpaulineОценок пока нет
- Diathermy ConceptsДокумент23 страницыDiathermy ConceptsPSNA VIJAYОценок пока нет
- Basic Surgical Skills Pauline 1Документ84 страницыBasic Surgical Skills Pauline 1paulineОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Rapra Review Reports. Polymers in Bulding and Construction (Halliwell S.M., Report 154), 2002 PDFДокумент150 страницRapra Review Reports. Polymers in Bulding and Construction (Halliwell S.M., Report 154), 2002 PDFdusik007100% (1)
- Biofibres and Biocomposites: Maya Jacob John, Sabu ThomasДокумент22 страницыBiofibres and Biocomposites: Maya Jacob John, Sabu Thomaspinkan25Оценок пока нет
- Introduccion Al Polietileno Industrial PDFДокумент29 страницIntroduccion Al Polietileno Industrial PDFFabrizzio Valer89% (9)
- Plasticization Effect of Triacetin On Structure and Properties of Starch Ester FilmДокумент8 страницPlasticization Effect of Triacetin On Structure and Properties of Starch Ester FilmNanik HendrawatiОценок пока нет
- PolydimethylsiloxaneMagnesium Oxide Nanosheet Mixed Matrix Membrane For CO2 Separation ApplicationДокумент21 страницаPolydimethylsiloxaneMagnesium Oxide Nanosheet Mixed Matrix Membrane For CO2 Separation ApplicationFikryОценок пока нет
- Drying Behavior of Dense Refractory Castables PartДокумент65 страницDrying Behavior of Dense Refractory Castables PartEbrahim BayoumiОценок пока нет
- International Journal of Adhesion & AdhesivesДокумент6 страницInternational Journal of Adhesion & AdhesivesAshwary Sheel Wali Research Scholar, Dept of Mech Engg., IIT (BHU)Оценок пока нет
- DuPont Teflon AF Processing GuideДокумент2 страницыDuPont Teflon AF Processing GuidewuaiyouОценок пока нет
- Chemistry Unit 1 Practice Exam 3Документ19 страницChemistry Unit 1 Practice Exam 3AlyciaLeeОценок пока нет
- 02 Polymer Modified Asphalt Emulsions Main ReportДокумент170 страниц02 Polymer Modified Asphalt Emulsions Main ReportgiamilliaОценок пока нет
- 152 (Esg)Документ15 страниц152 (Esg)Aditya Prakash Singh100% (1)
- Materials Science and Engineering C: Dan Kai, Sing Shy Liow, Xian Jun LohДокумент12 страницMaterials Science and Engineering C: Dan Kai, Sing Shy Liow, Xian Jun Lohjohn munezОценок пока нет
- O RingsДокумент211 страницO Ringsberylqz100% (2)
- 3.7 Types of Protein Exam QuestionДокумент3 страницы3.7 Types of Protein Exam QuestionjnfjngsdjОценок пока нет
- Mid-2 Objective Engineeringchemistry MaterialДокумент11 страницMid-2 Objective Engineeringchemistry MaterialengineeringchemistryОценок пока нет
- Rabinow 2004 - Nanosuspensions in Drug DeliveryДокумент12 страницRabinow 2004 - Nanosuspensions in Drug DeliveryGaluh PrimadaniОценок пока нет
- Zeng Et Al. - 2022 - Irreversible Synthesis of An Ultrastrong Two-Dimensional Polymeric MaterialДокумент13 страницZeng Et Al. - 2022 - Irreversible Synthesis of An Ultrastrong Two-Dimensional Polymeric MaterialHadi KenarangiОценок пока нет
- Organic Coatings for Corrosion ProtectionДокумент32 страницыOrganic Coatings for Corrosion ProtectionSreekumar RajendrababuОценок пока нет
- Parker ValvesДокумент64 страницыParker ValvesJaime PiedraОценок пока нет
- Review of Encapsulation Methods Suitable For Microbial Biological Control AgentsДокумент10 страницReview of Encapsulation Methods Suitable For Microbial Biological Control AgentsThiago Netto50% (2)
- Concrete Resin PoliesterДокумент22 страницыConcrete Resin Poliestercesar arangoОценок пока нет
- Biopharm Tubing: For Every Part of Your ProcessДокумент24 страницыBiopharm Tubing: For Every Part of Your ProcessFer PabОценок пока нет
- 10 Nylon 11 in Oil Gas1 PDFДокумент36 страниц10 Nylon 11 in Oil Gas1 PDFRamadhaniОценок пока нет
- Litex S 9076Документ1 страницаLitex S 9076New EmailОценок пока нет
- Seminar Final AnandДокумент43 страницыSeminar Final AnandAnand GargОценок пока нет
- Vatan Turkce KatalogДокумент40 страницVatan Turkce KatalogIrsan RajaminОценок пока нет
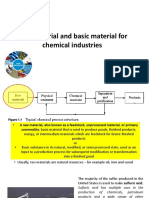
- Raw Material and Basic Material For Chemical IndustriesДокумент20 страницRaw Material and Basic Material For Chemical Industrieslaila nurul qodryОценок пока нет
- 548 5R-94 PDFДокумент26 страниц548 5R-94 PDFJoão Carlos Protz ProtzОценок пока нет
- Googlepreview PDFДокумент244 страницыGooglepreview PDFFREDY CORREAОценок пока нет
- Astm d2022Документ107 страницAstm d2022Anonymous 1ykzuaxWgYОценок пока нет