Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Act G ManualДокумент10 страницAct G ManualMayjie CummosОценок пока нет
- SJT Practice Paper 2 Answers Rationales 26-10-17Документ99 страницSJT Practice Paper 2 Answers Rationales 26-10-17scribdbazo100% (1)
- Tell The World Project WC EditДокумент3 страницыTell The World Project WC Editapi-473913057Оценок пока нет
- Accepted Manuscript: 10.1016/j.bja.2017.10.021Документ73 страницыAccepted Manuscript: 10.1016/j.bja.2017.10.021Ilham EfendiОценок пока нет
- Drug Guideline Title: Sodium Bicarbonate: SummaryДокумент4 страницыDrug Guideline Title: Sodium Bicarbonate: SummaryLoreine Jane ClaritoОценок пока нет
- Clinical Pharmacist in ICUДокумент26 страницClinical Pharmacist in ICUCosmina GeorgianaОценок пока нет
- Hubungan Antara Jarak Waktu Trakeostomi Dengan Mortalitas Pasien Kritis Ter20200505-4830-19g01dw-With-cover-page-V2Документ10 страницHubungan Antara Jarak Waktu Trakeostomi Dengan Mortalitas Pasien Kritis Ter20200505-4830-19g01dw-With-cover-page-V2IswandiОценок пока нет
- Pricing of Hospital ServicesДокумент5 страницPricing of Hospital ServicesSanjay KadamОценок пока нет
- Penatalaksanaan Keperawatan Covid 19 Di Respiratory Ward AustraliaДокумент22 страницыPenatalaksanaan Keperawatan Covid 19 Di Respiratory Ward AustraliaRadenroro Atih Utari RizkyОценок пока нет
- General Principles of Postoperative Intensive Care Unit CareДокумент17 страницGeneral Principles of Postoperative Intensive Care Unit CareSid DhayriОценок пока нет
- Early Mobility and Walking For Patients With Femoral Arterial Catheters in Intensive Care Unit: A Case SeriesДокумент5 страницEarly Mobility and Walking For Patients With Femoral Arterial Catheters in Intensive Care Unit: A Case Seriesapi-240991897Оценок пока нет
- My Philosophy of Professional Nursing PracticeДокумент3 страницыMy Philosophy of Professional Nursing Practiceapi-581399200Оценок пока нет
- Ccu Deparmental Operation PoliciesДокумент7 страницCcu Deparmental Operation PoliciesamalfarhanaОценок пока нет
- Obstetric HDU and ICU: Guidelines ForДокумент52 страницыObstetric HDU and ICU: Guidelines ForsidharthОценок пока нет
- CH 14 Test BankДокумент21 страницаCH 14 Test BankKrestine MolleОценок пока нет
- UntitledДокумент20 страницUntitledpratapekkaОценок пока нет
- Clinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentДокумент18 страницClinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentΜαρία ΧανιωτάκηОценок пока нет
- CritCareNurse 2006 Smith 41 7Документ9 страницCritCareNurse 2006 Smith 41 7ineОценок пока нет
- Course in The WardДокумент5 страницCourse in The WardAngelica Mercado SirotОценок пока нет
- Pt. Thiess PDFДокумент16 страницPt. Thiess PDFLehman ManОценок пока нет
- Brazilya Olumsuz Olay - MakaleДокумент6 страницBrazilya Olumsuz Olay - MakaleHazalОценок пока нет
- Hizon Interview Group 2Документ3 страницыHizon Interview Group 2Dan HizonОценок пока нет
- Hospital PlanningДокумент66 страницHospital PlanningAaquib Mahfuz100% (1)
- Starting Out - New in The ICUДокумент30 страницStarting Out - New in The ICUashdmb217100% (1)
- Use of Essential Oils Following Traumatic Burn Injury A Case StudyДокумент12 страницUse of Essential Oils Following Traumatic Burn Injury A Case StudyShandaPrimaDewiОценок пока нет
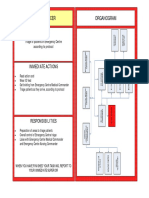
- Triage Officer Organogram: MissionДокумент14 страницTriage Officer Organogram: Missionsnow fazliОценок пока нет
- ICU Procedure HandoutsДокумент26 страницICU Procedure HandoutsDadi Veen100% (2)
- NEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0 PDFДокумент1 страницаNEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0 PDFPrajogo KusumaОценок пока нет
- Missed Opportunities An Observational Study of Vital SignsДокумент6 страницMissed Opportunities An Observational Study of Vital SignsZeera MohamadОценок пока нет
- Worldwide End-Of-Life Practice For Patients in Icus: ReviewДокумент7 страницWorldwide End-Of-Life Practice For Patients in Icus: ReviewANDREA CAROLINA SERNA BELTRANОценок пока нет