Вам также может понравиться
- Pharmacology MCQДокумент1 страницаPharmacology MCQmj CanilangОценок пока нет
- Chapter 46 Chest AssessmentДокумент12 страницChapter 46 Chest Assessmentmj CanilangОценок пока нет
- WHO Core Nurse Educator CompetenciesДокумент1 страницаWHO Core Nurse Educator Competenciesmj CanilangОценок пока нет
- Prelim Exam PharmaДокумент2 страницыPrelim Exam Pharmamj CanilangОценок пока нет
- Wifi HackingДокумент3 страницыWifi Hackingmj CanilangОценок пока нет
- Grading System For NCM 103 - 103A - Funda SL and RDДокумент2 страницыGrading System For NCM 103 - 103A - Funda SL and RDmj CanilangОценок пока нет
- Soliman SchedДокумент1 страницаSoliman Schedmj CanilangОценок пока нет
- PA Lec SchedДокумент5 страницPA Lec Schedmj CanilangОценок пока нет
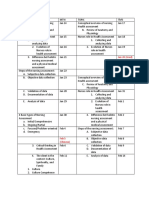
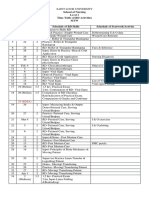
- School of Nursing Level 1 Time Table of RD Activities MTW Day Dates Hrs. Schedule of RD Skills Schedule of Seatwork/ActivityДокумент4 страницыSchool of Nursing Level 1 Time Table of RD Activities MTW Day Dates Hrs. Schedule of RD Skills Schedule of Seatwork/Activitymj CanilangОценок пока нет
- Funda RLE RD Time TableДокумент4 страницыFunda RLE RD Time Tablemj CanilangОценок пока нет
- Teaching Problem Solving in Large Introductory Classes: The View From PhysicsДокумент48 страницTeaching Problem Solving in Large Introductory Classes: The View From PhysicsAlvaro H GalvisОценок пока нет
- Alignment Matrix For PLOs Health AssessmentДокумент4 страницыAlignment Matrix For PLOs Health Assessmentmj CanilangОценок пока нет
- Grading System For NCM 100 - Skills Lectute and RDДокумент2 страницыGrading System For NCM 100 - Skills Lectute and RDmj CanilangОценок пока нет
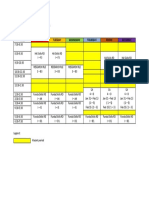
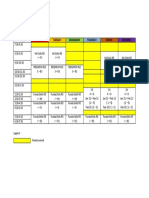
- Time Monday Tuesday Wednesday Thursday Friday SaturdayДокумент1 страницаTime Monday Tuesday Wednesday Thursday Friday Saturdaymj CanilangОценок пока нет
- Grading System For NCM 100 - Skills Lectute and RDДокумент2 страницыGrading System For NCM 100 - Skills Lectute and RDmj CanilangОценок пока нет
- Time Monday Tuesday Wednesday Thursday Friday SaturdayДокумент1 страницаTime Monday Tuesday Wednesday Thursday Friday Saturdaymj CanilangОценок пока нет
- Schedule For Faculty Use - DHДокумент1 страницаSchedule For Faculty Use - DHmj CanilangОценок пока нет
- Wound CareДокумент3 страницыWound Caremj CanilangОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Antepartum HeamorrhageДокумент23 страницыAntepartum HeamorrhageOlumide OlowoseluОценок пока нет
- Xylin Specialist ToothpasteДокумент3 страницыXylin Specialist ToothpasteMarvin AngОценок пока нет
- Urinary IncontinenceДокумент0 страницUrinary Incontinencemango91286Оценок пока нет
- OET Listening Test Question PaperДокумент10 страницOET Listening Test Question PaperkimОценок пока нет
- ProofcorrectionsДокумент10 страницProofcorrectionsRicardo QuintanaОценок пока нет
- Jurnal Obes 1Документ22 страницыJurnal Obes 1mat norОценок пока нет
- Causes of Male InfertilityДокумент31 страницаCauses of Male InfertilityChris Emmanuel NathanОценок пока нет
- Wen Bing2Документ9 страницWen Bing2Jaffer Aftab0% (1)
- Clinical Tips For The Management of Perimenopausal Syndrome by DR - Deepti ChawlaДокумент19 страницClinical Tips For The Management of Perimenopausal Syndrome by DR - Deepti ChawlaHomoeopathic PulseОценок пока нет
- PalatoplastyДокумент5 страницPalatoplastyAngga HermawanОценок пока нет
- Drug Study Name of Drug Classification Adverse Effect Indication Contraindication Nursing ConsiderationДокумент3 страницыDrug Study Name of Drug Classification Adverse Effect Indication Contraindication Nursing ConsiderationCarmie CorpusОценок пока нет
- GONIOSCOPY1Документ74 страницыGONIOSCOPY1partani_anand100% (1)
- Effects of Implementation of Focus-Pdca Model To Decrease Patients' Length of Stay in Emergency DepartmentДокумент5 страницEffects of Implementation of Focus-Pdca Model To Decrease Patients' Length of Stay in Emergency DepartmentMuhammad RamadhanОценок пока нет
- Cross Section Heart - Superior Inferior Vena CavaДокумент2 страницыCross Section Heart - Superior Inferior Vena CavaAlice Del Rosario CabanaОценок пока нет
- Anatomy: Patellar Tendon TearДокумент11 страницAnatomy: Patellar Tendon TearrahadianpambudiОценок пока нет
- DafpusДокумент3 страницыDafpusOtty Mitha OctrizaОценок пока нет
- Child Survival and Safe Motherhood Programme (CSSMP) : 1.CSSM Programme Initiated in The YearДокумент8 страницChild Survival and Safe Motherhood Programme (CSSMP) : 1.CSSM Programme Initiated in The YearJagveer ChauhanОценок пока нет
- Trigonum Colli AnteriusДокумент13 страницTrigonum Colli Anteriusyati rosmiatiОценок пока нет
- Comparison of Intermittent Bolus and Continuous Infusion Techniques For Administration of Atracurium in Renal FailureДокумент5 страницComparison of Intermittent Bolus and Continuous Infusion Techniques For Administration of Atracurium in Renal FailureWantoSKepОценок пока нет
- Full RujiraLeukorrhea, STDS, HIV Infection.02102017 PDFДокумент129 страницFull RujiraLeukorrhea, STDS, HIV Infection.02102017 PDFrujiraОценок пока нет
- Tahbso ArticleДокумент4 страницыTahbso ArticleAlianna Kristine OhОценок пока нет
- 2011 - Policy For Medico Legal Cases (MLC)Документ6 страниц2011 - Policy For Medico Legal Cases (MLC)Shawred Analytics100% (1)
- Five Methods of Breast Volume Measurement: A Comparative Study of Measurements of Specimen Volume in 30 Mastectomy CasesДокумент10 страницFive Methods of Breast Volume Measurement: A Comparative Study of Measurements of Specimen Volume in 30 Mastectomy CasesDIOGENESОценок пока нет
- Perinatal Factor Journal PediatricДокумент8 страницPerinatal Factor Journal PediatricHasya KinasihОценок пока нет
- Vulvar Care e PDFДокумент9 страницVulvar Care e PDFainurrohmaniyahОценок пока нет
- Dr. Hur JunДокумент2 страницыDr. Hur JunMegha GoyalОценок пока нет
- Jurnal Tetes MataДокумент6 страницJurnal Tetes MataSyafiraОценок пока нет
- JGCA JPN Classification 3rd EngДокумент12 страницJGCA JPN Classification 3rd EngLiz PesantesОценок пока нет
- Prepping and Draping The PatientДокумент26 страницPrepping and Draping The Patientjosphinenthenya001Оценок пока нет
- INTRAPARTUMДокумент18 страницINTRAPARTUMMICHELLE FACTOОценок пока нет