Вам также может понравиться
- Vitamins and Minerals: Nutrient (Vitamins) Needed For Key SourcesДокумент4 страницыVitamins and Minerals: Nutrient (Vitamins) Needed For Key SourcesKevin Carl A. CorpuzОценок пока нет
- Muscles of The Upper Limb Made EasyДокумент7 страницMuscles of The Upper Limb Made Easynss92% (26)
- Clinical Anatomy of Upper Limb Joints and MusclesДокумент92 страницыClinical Anatomy of Upper Limb Joints and Musclesgechanatomy100% (1)
- Anatomy and Physiology: Prepared By: Ms. Irish SequihodДокумент30 страницAnatomy and Physiology: Prepared By: Ms. Irish SequihodMarie Fhel G OpenaОценок пока нет
- Anatomy and Physiology No.1Документ38 страницAnatomy and Physiology No.1Ken Marco SalipsipОценок пока нет
- Pagoda - Jeffrey Schecter - Core RulebookДокумент23 страницыPagoda - Jeffrey Schecter - Core Rulebookcaecus7634Оценок пока нет
- Exploratory Latin AnimalsДокумент15 страницExploratory Latin AnimalsKari Kristine Hoskins BarreraОценок пока нет
- Origins, Insertions, and Functions of Human MusclesДокумент5 страницOrigins, Insertions, and Functions of Human MusclesNikhil Narang100% (1)
- 1.introdution To Human Anatomy 1Документ51 страница1.introdution To Human Anatomy 1ruwanganiОценок пока нет
- Back Injuries - Safety MomentДокумент13 страницBack Injuries - Safety MomentAinun Rahmania100% (1)
- Malaysia Asean Science Olympiads: Rules and RegulationsДокумент11 страницMalaysia Asean Science Olympiads: Rules and RegulationsKarren Cacabelos SurОценок пока нет
- Healthy Shoulder Handbook: 100 Exercises for Treating and Preventing Frozen Shoulder, Rotator Cuff and other Common InjuriesОт EverandHealthy Shoulder Handbook: 100 Exercises for Treating and Preventing Frozen Shoulder, Rotator Cuff and other Common InjuriesРейтинг: 2 из 5 звезд2/5 (1)
- Acupuntura - Pulso Tornozelo - InglêsДокумент40 страницAcupuntura - Pulso Tornozelo - InglêsAntonio de AlexandreОценок пока нет
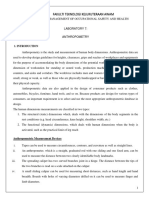
- AnthropometryДокумент4 страницыAnthropometryGeline EsguerraОценок пока нет
- Velopharyngeal DefectsДокумент66 страницVelopharyngeal DefectsVivek ShankarОценок пока нет
- Assessing Childbearing WomenДокумент5 страницAssessing Childbearing WomenJola Ogundiya100% (1)
- Zoology BiomesДокумент11 страницZoology BiomesDennie Zody LoganОценок пока нет
- D 5219 - 99 - RduymtktotkДокумент4 страницыD 5219 - 99 - RduymtktotkMorched TounsiОценок пока нет
- DwarfsДокумент14 страницDwarfslololol69Оценок пока нет
- XBOE4103 - Occupational Ergonomics - Signoff - Soalan AmaliДокумент17 страницXBOE4103 - Occupational Ergonomics - Signoff - Soalan AmalinorfilzahОценок пока нет
- 191 - XBOE4103 - Occupational Ergonomics Lab ManualДокумент16 страниц191 - XBOE4103 - Occupational Ergonomics Lab ManualHuda Hafiz100% (1)
- Lab 7 AnthropometricДокумент6 страницLab 7 Anthropometricadeliene 25Оценок пока нет
- What Is Anthropometry?Документ4 страницыWhat Is Anthropometry?GodisGood AlltheTimeОценок пока нет
- Anthropometry: Assessment and Monitoring of GrowthДокумент10 страницAnthropometry: Assessment and Monitoring of GrowthAbhishek GirdharОценок пока нет
- LAB 03 - AnthropometryДокумент11 страницLAB 03 - AnthropometryMilter GiОценок пока нет
- Ch1 Intro To AnatomyДокумент5 страницCh1 Intro To AnatomyztolmanОценок пока нет
- AnthropometryДокумент13 страницAnthropometryMustofa BahriОценок пока нет
- AnthropometryДокумент17 страницAnthropometrybasmalanasser004Оценок пока нет
- Hong Kong Child Data ErgonomicsДокумент24 страницыHong Kong Child Data Ergonomicshceti3111OMОценок пока нет
- Anatomy Handbook-CodeworksДокумент171 страницаAnatomy Handbook-CodeworksBe GameОценок пока нет
- Anthropometric MeasurementsДокумент11 страницAnthropometric MeasurementsKinjal SharmaОценок пока нет
- Craniometry: Craniometry Is A Technique Used To Measure Skull and Determine Human NatureДокумент7 страницCraniometry: Craniometry Is A Technique Used To Measure Skull and Determine Human NatureZirgi RanaОценок пока нет
- Es411 Week 5Документ25 страницEs411 Week 5sezerkumtashОценок пока нет
- ThesisДокумент11 страницThesisShruti ChaudharyОценок пока нет
- 14.ergonomic Workstation Design For Science Laboratory (Norhafizah Rosman) PP 93-102Документ10 страниц14.ergonomic Workstation Design For Science Laboratory (Norhafizah Rosman) PP 93-102upenapahangОценок пока нет
- ISAK Antrophometric CourseДокумент5 страницISAK Antrophometric Coursekabut81Оценок пока нет
- CHAPTER THREE - MethodДокумент5 страницCHAPTER THREE - MethodAhmed ElabdlyОценок пока нет
- NutriДокумент6 страницNutri002Оценок пока нет
- Peerj 04 2397Документ18 страницPeerj 04 2397Wannapa TarananimitОценок пока нет
- BME411 - Physiological Fluid MechanicsДокумент93 страницыBME411 - Physiological Fluid Mechanicsjoyonize08Оценок пока нет
- Anthropocentric TechniqueДокумент16 страницAnthropocentric TechniqueNeelam SiddiquiОценок пока нет
- Introduction To Anatomy by WubshetДокумент55 страницIntroduction To Anatomy by WubshetTofik MohammedОценок пока нет
- Chapter 1Документ12 страницChapter 1Ajay Pal NattОценок пока нет
- Frozen ShoulderДокумент33 страницыFrozen ShoulderPrashant YadavОценок пока нет
- Introduction To Anatomy: BY Ap Dr. Khin Thant Zin 2017Документ42 страницыIntroduction To Anatomy: BY Ap Dr. Khin Thant Zin 2017emyОценок пока нет
- 028 With Cover Page v2Документ9 страниц028 With Cover Page v2Carunia MuliaОценок пока нет
- 1 Antropometri CSДокумент17 страниц1 Antropometri CSTop Eleven2Оценок пока нет
- Engineering Anthropometry: AbstractДокумент4 страницыEngineering Anthropometry: Abstractlakku12Оценок пока нет
- D 5219 - 99 RduymtktukveДокумент10 страницD 5219 - 99 RduymtktukveJuan GutierrezОценок пока нет
- Musculoskeletal SystemДокумент160 страницMusculoskeletal SystemAirene Aquino BusaniaОценок пока нет
- Basic Anatomical TerminologyДокумент11 страницBasic Anatomical TerminologyJayrelle D. SafranОценок пока нет
- Perancangan Meja Dapur Ergonomis Pada Masyarakat Desa: Suryani, Basuki Arianto Dan Wt. BhirawaДокумент13 страницPerancangan Meja Dapur Ergonomis Pada Masyarakat Desa: Suryani, Basuki Arianto Dan Wt. BhirawaKii IkiiОценок пока нет
- The Human Organism: ThehumanorganismДокумент9 страницThe Human Organism: ThehumanorganismElaine MaghanoyОценок пока нет
- The Human Body: Cartoneros, Jane Marie S. Morillo Eriz Shane B. Peren, Aira M. Razon Judylyn B. Bsed Math 1101Документ29 страницThe Human Body: Cartoneros, Jane Marie S. Morillo Eriz Shane B. Peren, Aira M. Razon Judylyn B. Bsed Math 1101Aira PerenОценок пока нет
- Basic Human Anatomy AND Physiology: Emmanuel Z. Pagala M.DДокумент136 страницBasic Human Anatomy AND Physiology: Emmanuel Z. Pagala M.DDARLENE SUETOSОценок пока нет
- Cun MeasurementsДокумент3 страницыCun MeasurementsAliki MaraveliaОценок пока нет
- AnthropДокумент51 страницаAnthropRori de los ReyesОценок пока нет
- Anthropometry: by G Hema MaliniДокумент52 страницыAnthropometry: by G Hema MaliniHema MaliniОценок пока нет
- Shoulder AnatomyДокумент8 страницShoulder AnatomyPraneeth KumarОценок пока нет
- The Comparison and Evaluation of Carrying Angle of Elbow With Anthropometric Measurements in Both SexesДокумент5 страницThe Comparison and Evaluation of Carrying Angle of Elbow With Anthropometric Measurements in Both SexesChetanya aggarwalОценок пока нет
- AnthroДокумент30 страницAnthroJuli DeviaОценок пока нет
- اطراف كاملة كورس 2Документ42 страницыاطراف كاملة كورس 2قاسم محمدОценок пока нет
- PhysioLab Module2Документ13 страницPhysioLab Module2Lizadette Balanci LazoОценок пока нет
- Sup-ER Orthosis: An Innovative Treatment For Infants With Birth Related Brachial Plexus InjuryДокумент6 страницSup-ER Orthosis: An Innovative Treatment For Infants With Birth Related Brachial Plexus InjuryJuli DeviaОценок пока нет
- Upper Extremity Pain - Jack L RookДокумент60 страницUpper Extremity Pain - Jack L RookShauki AliОценок пока нет
- Classification & Characteristics of Human S Classification & Characteristics of Human SДокумент37 страницClassification & Characteristics of Human S Classification & Characteristics of Human SShafaqat Ghani Shafaqat GhaniОценок пока нет
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointОт EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointОценок пока нет
- Invitation Layout: Irene D. Cabunyag Ms. Abigail VitoДокумент2 страницыInvitation Layout: Irene D. Cabunyag Ms. Abigail VitoWarren De Lumen CabunyagОценок пока нет
- Online Monitoring of Sow Breeding in Lucban Quezon Using Information SystemДокумент1 страницаOnline Monitoring of Sow Breeding in Lucban Quezon Using Information SystemWarren De Lumen CabunyagОценок пока нет
- Oversize Materials Existence of Foreign Objects: Unclean Machine Not Properly HammeredДокумент1 страницаOversize Materials Existence of Foreign Objects: Unclean Machine Not Properly HammeredWarren De Lumen CabunyagОценок пока нет
- Appendix B. Reliability and Mean Time To Repair (MTTR) ComputationДокумент2 страницыAppendix B. Reliability and Mean Time To Repair (MTTR) ComputationWarren De Lumen CabunyagОценок пока нет
- Usability in Context: Improving Quality of Use: Miles MacleodДокумент7 страницUsability in Context: Improving Quality of Use: Miles MacleodWarren De Lumen CabunyagОценок пока нет
- INCAN AND AZTECS MAJESTIES CULTURESessayДокумент5 страницINCAN AND AZTECS MAJESTIES CULTURESessayMary Isabel DCОценок пока нет
- SANGGUNIANДокумент3 страницыSANGGUNIANirby AcabadoОценок пока нет
- Report Text About PandaДокумент2 страницыReport Text About PandaYOHANES NONOОценок пока нет
- Euthanasia: Methods of Euthanasia Case Study - Euthanasia ReferencesДокумент11 страницEuthanasia: Methods of Euthanasia Case Study - Euthanasia ReferencesManoj KarkiОценок пока нет
- Selat BaliДокумент3 страницыSelat BaliyensiОценок пока нет
- Handouts Fable-1Документ5 страницHandouts Fable-1Joezel Vince EfondoОценок пока нет
- ĐỀ ĐỀ XUẤT ANH 10 -CBNДокумент12 страницĐỀ ĐỀ XUẤT ANH 10 -CBNNgan LeОценок пока нет
- Nurse EnglishДокумент7 страницNurse EnglishBudhi Priyanto DitaraОценок пока нет
- Symbiosis PresentationДокумент7 страницSymbiosis Presentationmisterbrowner@yahoo.com100% (1)
- Globalization in FisheriesДокумент7 страницGlobalization in Fisheriesnylra MОценок пока нет
- Pass Al UrusДокумент4 страницыPass Al UrusMirjana Karanovic-SamardzijaОценок пока нет
- Anatomical Planes: MD Valeria de La Peña GutierrezДокумент36 страницAnatomical Planes: MD Valeria de La Peña GutierrezValeria De la peñaОценок пока нет
- Presentation 1Документ52 страницыPresentation 1Capili AppleОценок пока нет
- Soal UN BIG 2017 BДокумент11 страницSoal UN BIG 2017 BasmaОценок пока нет
- Breathing Ny Hidetaka NishiyamaДокумент3 страницыBreathing Ny Hidetaka NishiyamaJohnОценок пока нет
- Aipg 09 MDSДокумент7 страницAipg 09 MDSDENTALORG.COM100% (2)
- Normal Menstrual Cycle The ProcessДокумент6 страницNormal Menstrual Cycle The ProcessBrett StevensonОценок пока нет
- AQA-synoptic Essay Marking GuidelinesДокумент13 страницAQA-synoptic Essay Marking GuidelinesSarah HarleyОценок пока нет
- Anatomy of Organum GustatoriumДокумент11 страницAnatomy of Organum GustatoriumthesaanandaОценок пока нет
- Nama Binatang A - ZДокумент24 страницыNama Binatang A - ZNur H. TauchidОценок пока нет
- Tensile Strength of FibersДокумент26 страницTensile Strength of FibersSandip Bakshi50% (2)
- Agriculture Question Paper GR.5Документ6 страницAgriculture Question Paper GR.5vemuna katjiuanjoОценок пока нет