Вам также может понравиться
- Heart Failure With Normal Ejection Fraction (HFNEF) : Is It Worth Considering?Документ7 страницHeart Failure With Normal Ejection Fraction (HFNEF) : Is It Worth Considering?bhaskarpurushottamОценок пока нет
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareДокумент10 страницCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareMirachel AugustОценок пока нет
- 403 Full PDFДокумент10 страниц403 Full PDFKuroto YoshikiОценок пока нет
- Dirk L. Brutsaert 2007-1Документ9 страницDirk L. Brutsaert 2007-1CARLOS FRANCISCO MANTILLA MONTALVOОценок пока нет
- Diastolic CHF DiagnosisДокумент3 страницыDiastolic CHF DiagnosissamОценок пока нет
- Diagnosing Heart Failure with Preserved Ejection FractionДокумент8 страницDiagnosing Heart Failure with Preserved Ejection FractionErwin GuerreroОценок пока нет
- Heart Failure With Preserved Ejection Fraction - Concept, Pathophysiology, Diagnosis and Challenges For TreatmentДокумент7 страницHeart Failure With Preserved Ejection Fraction - Concept, Pathophysiology, Diagnosis and Challenges For TreatmentOngky AristianОценок пока нет
- Heart Failure With Preserved Ejection FractionДокумент19 страницHeart Failure With Preserved Ejection Fractioncosmin balanОценок пока нет
- CHFДокумент10 страницCHFPowpOw SangalangОценок пока нет
- Heart Failure Diagnosis and ClassificationДокумент12 страницHeart Failure Diagnosis and ClassificationFreddy PanjaitanОценок пока нет
- Heart Failure With Preserved Ejection Fraction (Hfpef) : A Basic and Clinical PerspectiveДокумент5 страницHeart Failure With Preserved Ejection Fraction (Hfpef) : A Basic and Clinical PerspectiveOngky AristianОценок пока нет
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareДокумент10 страницCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareKevinDilianSugandaОценок пока нет
- 67-Article Text-115-1-10-20171026Документ5 страниц67-Article Text-115-1-10-20171026Maria MiripОценок пока нет
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareДокумент10 страницCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareIntan PurnamasariОценок пока нет
- Brahmbhatt 2018Документ7 страницBrahmbhatt 2018Jr SparkОценок пока нет
- Kjae 70 3Документ10 страницKjae 70 3drsubramanianОценок пока нет
- Ghid Heart FailureДокумент117 страницGhid Heart FailureIlie RoxanaОценок пока нет
- Clinical Epidemiology of Heart Failure ReviewedДокумент11 страницClinical Epidemiology of Heart Failure ReviewedCAMILO ANDRES TOVAR DAZAОценок пока нет
- FCA Hipertensiva Viau2015Документ8 страницFCA Hipertensiva Viau2015gioandregabОценок пока нет
- CME-HFДокумент14 страницCME-HFEffika PutriОценок пока нет
- Journal Reading ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart Failure 2012Документ127 страницJournal Reading ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart Failure 2012Femmy TaniaОценок пока нет
- Penanganan Gagal Jantung Diastolik: Starry H. RampenganДокумент9 страницPenanganan Gagal Jantung Diastolik: Starry H. Rampenganpaul silabanОценок пока нет
- CHF PathДокумент7 страницCHF PathGeraldine Gallaron - CasipongОценок пока нет
- IM - Heart Failure Part 1Документ6 страницIM - Heart Failure Part 1Elisha BernabeОценок пока нет
- Mecanismos Fisiopatológicos de Insuficiencia Cardiaca Con FEVI PreservadaДокумент26 страницMecanismos Fisiopatológicos de Insuficiencia Cardiaca Con FEVI PreservadaJenny de OzОценок пока нет
- Heart Failure: Definition, Classification, Epidemiology & PathophysiologyДокумент10 страницHeart Failure: Definition, Classification, Epidemiology & PathophysiologyAlbert ShantoОценок пока нет
- Create PDFДокумент14 страницCreate PDFIkbar FauzanОценок пока нет
- Patofisiologi CHFДокумент7 страницPatofisiologi CHFHafiz Idul FitranulОценок пока нет
- How To Manage Heart Failure New Guidelines 2018Документ3 страницыHow To Manage Heart Failure New Guidelines 2018Dana BursacovschiОценок пока нет
- Heart FailureДокумент70 страницHeart FailureNabin BhusalОценок пока нет
- Right Heart Failure A Narrative Review For Emergency CliniciansДокумент8 страницRight Heart Failure A Narrative Review For Emergency ClinicianssunhaolanОценок пока нет
- Pathophysiology and Management of Heart FailureДокумент21 страницаPathophysiology and Management of Heart FailureRaíla SoaresОценок пока нет
- 1 s2.0 S0735109722056030 MainДокумент15 страниц1 s2.0 S0735109722056030 MainAkhmad HidayatОценок пока нет
- Eisenmenger Syndrome: A Clinical Perspective in A New Therapeutic Era of Pulmonary Arterial HypertensionДокумент8 страницEisenmenger Syndrome: A Clinical Perspective in A New Therapeutic Era of Pulmonary Arterial HypertensionWegrimel AriegaraОценок пока нет
- Etiology: Table 279-1Документ31 страницаEtiology: Table 279-1CatharinaNoviaОценок пока нет
- Falla Cardiaca ReviewДокумент9 страницFalla Cardiaca ReviewYasmin CarhuamacaОценок пока нет
- Heart FailureДокумент8 страницHeart FailureSophia MarieОценок пока нет
- Algorithm For Therapeutic Management of Acute Heart Failure SyndromesДокумент5 страницAlgorithm For Therapeutic Management of Acute Heart Failure SyndromesaegonblackОценок пока нет
- Heart FailureДокумент16 страницHeart FailureAmalia CajesОценок пока нет
- Heart Failure - Clinical Manifestations and Diagnosis in Adults - UpToDateДокумент39 страницHeart Failure - Clinical Manifestations and Diagnosis in Adults - UpToDateArthurОценок пока нет
- Chronic heart failure diagnosis and treatment strategiesДокумент9 страницChronic heart failure diagnosis and treatment strategiesAndi Tiara S. AdamОценок пока нет
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionДокумент15 страницCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoОценок пока нет
- Congestive Heart FailureДокумент13 страницCongestive Heart FailureAgeng BudianantiОценок пока нет
- Clinical Manifestations and Evaluation of The Patient With Suspected Heart Failure PDFДокумент23 страницыClinical Manifestations and Evaluation of The Patient With Suspected Heart Failure PDFcristianamihailaОценок пока нет
- Clinical Assessment in Acute Heart Failure: Review ArticleДокумент17 страницClinical Assessment in Acute Heart Failure: Review ArticleAnonymous NeRC5JYiSОценок пока нет
- 1414 431X BJMBR 53 7 E9646Документ16 страниц1414 431X BJMBR 53 7 E9646leidyalexserraoОценок пока нет
- Heart Failure OlderДокумент18 страницHeart Failure OlderRESIDENTES MEDICINA INTERNAОценок пока нет
- Heart Failure: Clinical Manifestations and Diagnosis in Adults - UpToDateДокумент44 страницыHeart Failure: Clinical Manifestations and Diagnosis in Adults - UpToDateJulia Pelissaro CarboniОценок пока нет
- Mitchell 2005Документ8 страницMitchell 2005DianОценок пока нет
- Hall 2013Документ6 страницHall 2013Julio Orallo MartínezОценок пока нет
- Chronic Heart FailureДокумент11 страницChronic Heart FailurelaydyОценок пока нет
- Heart Failure With Preserved Ejection FractionДокумент7 страницHeart Failure With Preserved Ejection FractionJoko NahamaОценок пока нет
- Atrial FibrillationДокумент20 страницAtrial Fibrillationsabadboy 01Оценок пока нет
- Atrial Fibrillation and Heart Failure - Cause or Effect?Документ8 страницAtrial Fibrillation and Heart Failure - Cause or Effect?Cosmin GabrielОценок пока нет
- Causes of Heart FailureДокумент4 страницыCauses of Heart Failurejana7-7Оценок пока нет
- Ventriculo Derecho IIДокумент15 страницVentriculo Derecho IIElizabeth Yaya InfanteОценок пока нет
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtОт EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtРейтинг: 5 из 5 звезд5/5 (1)
- Down Syndrome and Incidental Pediatric Basal Ganglia Calcifications at AutopsyДокумент3 страницыDown Syndrome and Incidental Pediatric Basal Ganglia Calcifications at AutopsyPaul HartingОценок пока нет
- Structural and Functional Brain Differences in Key Opinion Journal LeadersДокумент4 страницыStructural and Functional Brain Differences in Key Opinion Journal LeadersPaul HartingОценок пока нет
- Indications and Clinical Outcomes of High Tibial Osteotomy A Literature ReviewДокумент8 страницIndications and Clinical Outcomes of High Tibial Osteotomy A Literature ReviewPaul HartingОценок пока нет
- Changes in The Structure of Synovial Fluids Between Healthy Joints and in OsteoarthritisДокумент3 страницыChanges in The Structure of Synovial Fluids Between Healthy Joints and in OsteoarthritisPaul HartingОценок пока нет
- Generation and Characterization of A Monoclonal Antibody Against Pseudorabies Virus Glycoprotein CДокумент5 страницGeneration and Characterization of A Monoclonal Antibody Against Pseudorabies Virus Glycoprotein CPaul HartingОценок пока нет
- Molecular Analysis For Genetic Diversity and Population Structure of Ethiopian Faba Bean (Vicia Faba L) AccessionsДокумент10 страницMolecular Analysis For Genetic Diversity and Population Structure of Ethiopian Faba Bean (Vicia Faba L) AccessionsPaul HartingОценок пока нет
- CAR-T Cell Immunotherapy and Nanotechnology: An Integrated Approach For Cancer CareДокумент2 страницыCAR-T Cell Immunotherapy and Nanotechnology: An Integrated Approach For Cancer CarePaul HartingОценок пока нет
- Multifocal Tuberculosis in Southern Tunisia What Is Specific With ?Документ4 страницыMultifocal Tuberculosis in Southern Tunisia What Is Specific With ?Paul HartingОценок пока нет
- Aneurysmal Bone Cyst of The Fibular Malleolus Report of An Additional Case at Rare SiteДокумент4 страницыAneurysmal Bone Cyst of The Fibular Malleolus Report of An Additional Case at Rare SitePaul HartingОценок пока нет
- Repulsive Lubrication On Hydrophilic SurfacesДокумент4 страницыRepulsive Lubrication On Hydrophilic SurfacesPaul HartingОценок пока нет
- Two Stage Treatment of Concomitant Complicated Right Amyand's Hernia and Incarcerated Left Inguinal Hernia Case Report and Review of The LiteratureДокумент3 страницыTwo Stage Treatment of Concomitant Complicated Right Amyand's Hernia and Incarcerated Left Inguinal Hernia Case Report and Review of The LiteraturePaul HartingОценок пока нет
- Pigmented Bowen Disease On Sclerosus and Atrophicus LichenДокумент3 страницыPigmented Bowen Disease On Sclerosus and Atrophicus LichenPaul HartingОценок пока нет
- Crop Tolerance Against Salt StressДокумент2 страницыCrop Tolerance Against Salt StressPaul HartingОценок пока нет
- Simultaneous Determination of The Ratio of Live, Dead and Adherent Bacteria in The Presence of Various Single-Walled Carbon NanotubesДокумент5 страницSimultaneous Determination of The Ratio of Live, Dead and Adherent Bacteria in The Presence of Various Single-Walled Carbon NanotubesPaul HartingОценок пока нет
- Effect of Size On Gold Nanoparticles in Radiation Therapy Uptake and Survival EffectsДокумент8 страницEffect of Size On Gold Nanoparticles in Radiation Therapy Uptake and Survival EffectsPaul HartingОценок пока нет
- Seborrheic Keratosis of The Breast Mimicking MelanomaДокумент3 страницыSeborrheic Keratosis of The Breast Mimicking MelanomaPaul HartingОценок пока нет
- Maternal and Fetal Effects of Cardiac Illness During Pregnancy in Beni Suef LocalitiesEgypt A Multi Centric Cross Sectional StudyДокумент7 страницMaternal and Fetal Effects of Cardiac Illness During Pregnancy in Beni Suef LocalitiesEgypt A Multi Centric Cross Sectional StudyPaul HartingОценок пока нет
- Difference Between Being in Favor of Permitting Abortion After Rape and Willingness To Provide Such Services According To Physician's CharacteristicsДокумент4 страницыDifference Between Being in Favor of Permitting Abortion After Rape and Willingness To Provide Such Services According To Physician's CharacteristicsPaul HartingОценок пока нет
- Extra Genital Lichen Sclero AtrophicДокумент2 страницыExtra Genital Lichen Sclero AtrophicPaul HartingОценок пока нет
- Recombinant Human Bone Morphogenetic Protein 2 For Correction of Unilateral Cleft Lip and Palatal Case ReportДокумент4 страницыRecombinant Human Bone Morphogenetic Protein 2 For Correction of Unilateral Cleft Lip and Palatal Case ReportPaul HartingОценок пока нет
- Neuromyelitis Optica Spectrum Disorder With Spinal Involvement Including Conus Medullaris Lesions With Anti-Aquaporin-4 Antibody: A Pediatric Case and Literature ReviewДокумент3 страницыNeuromyelitis Optica Spectrum Disorder With Spinal Involvement Including Conus Medullaris Lesions With Anti-Aquaporin-4 Antibody: A Pediatric Case and Literature ReviewPaul HartingОценок пока нет
- Examining The Association of Right Ventricular Dysfunction With Moderate To Severe Bronchopulmonary Dysplasia in Preterm InfantsДокумент7 страницExamining The Association of Right Ventricular Dysfunction With Moderate To Severe Bronchopulmonary Dysplasia in Preterm InfantsPaul HartingОценок пока нет
- Oral Apthous Ulcer Healing StepsДокумент2 страницыOral Apthous Ulcer Healing StepsPaul HartingОценок пока нет
- Prevalence of Anti Cyclic Citrullinated Peptide Antibodies in Juvenile Idiopathic Arthritis in BeninДокумент4 страницыPrevalence of Anti Cyclic Citrullinated Peptide Antibodies in Juvenile Idiopathic Arthritis in BeninPaul HartingОценок пока нет
- A Novel Use of Extracorporeal Membrane Oxygenation in The Management of Prosthetic Valve Thrombosis During PregnancyДокумент4 страницыA Novel Use of Extracorporeal Membrane Oxygenation in The Management of Prosthetic Valve Thrombosis During PregnancyPaul HartingОценок пока нет
- Use of Short Term Orthodontics by The Specialist OrthodontistДокумент5 страницUse of Short Term Orthodontics by The Specialist OrthodontistPaul HartingОценок пока нет
- Who Was HakimДокумент2 страницыWho Was HakimPaul HartingОценок пока нет
- Factors Associated With Self Rated Oral Health in Adolescents in São Luís Maranhão Brazil 2014Документ8 страницFactors Associated With Self Rated Oral Health in Adolescents in São Luís Maranhão Brazil 2014Paul HartingОценок пока нет
- Potassium Channels in Breast CancerДокумент6 страницPotassium Channels in Breast CancerPaul HartingОценок пока нет
- Benign Stromal Tumor Breast ImagesДокумент2 страницыBenign Stromal Tumor Breast ImagesPaul HartingОценок пока нет
- Acute Kidney Injury: Gezahegn D. (Pediatrian)Документ46 страницAcute Kidney Injury: Gezahegn D. (Pediatrian)Abu HajerahОценок пока нет
- PG BOTANY Plant Physiology Question Bank CompleteДокумент10 страницPG BOTANY Plant Physiology Question Bank CompleteAbid ShowketОценок пока нет
- CH 10 Test BankДокумент25 страницCH 10 Test BankBiano, Fortune JayneОценок пока нет
- Chapter 16 Anatomy of The HeartДокумент5 страницChapter 16 Anatomy of The Heartphotojockey18Оценок пока нет
- Antiporda Pcoglec-Hw1midtermsДокумент5 страницAntiporda Pcoglec-Hw1midtermsSean Antiporda100% (1)
- Acute Renal FailureДокумент4 страницыAcute Renal FailureKim GarciaОценок пока нет
- Eddy Wirawan, SPJP - Fiha: Rsud. Ulin BanjarmasinДокумент49 страницEddy Wirawan, SPJP - Fiha: Rsud. Ulin Banjarmasineka febriantyОценок пока нет
- Cardiorespiratory Arrest (FS)Документ88 страницCardiorespiratory Arrest (FS)haerul ikhsanОценок пока нет
- Peripheral Vascular DiseaseДокумент17 страницPeripheral Vascular DiseaseJee Ho SohnОценок пока нет
- EMD Guidecards PDFДокумент49 страницEMD Guidecards PDFЛизатро1980 ЛизаОценок пока нет
- Haad AnswersДокумент106 страницHaad AnswersMohammadKhanОценок пока нет
- 10 Palpasi Abdomen Dan Bagian Tubuh LainnyaДокумент26 страниц10 Palpasi Abdomen Dan Bagian Tubuh LainnyaSANGGA BUWANAОценок пока нет
- Patient 1 Drug StudyДокумент2 страницыPatient 1 Drug StudyCharlyn JenselОценок пока нет
- Introduction to Cells and Signaling in the Nervous SystemДокумент23 страницыIntroduction to Cells and Signaling in the Nervous SystemadfhОценок пока нет
- 09-10 ABSITE Review Session1Документ72 страницы09-10 ABSITE Review Session1Katerina Ts100% (4)
- SEMINARДокумент31 страницаSEMINARDeveshОценок пока нет
- Anatomy of The HeartДокумент42 страницыAnatomy of The HeartMae Rose Charlene MendozaОценок пока нет
- Unlock-Forensik Etik Medikolegal - PESERTAДокумент156 страницUnlock-Forensik Etik Medikolegal - PESERTAAde fathОценок пока нет
- Muscle Tissue and Physiology of Muscle ContractionДокумент16 страницMuscle Tissue and Physiology of Muscle ContractionPRIYADARSHINIОценок пока нет
- Final TCS ModuleДокумент24 страницыFinal TCS Modulemae cudalОценок пока нет
- SpermatogenesisДокумент2 страницыSpermatogenesisKRISTOFER BALAISОценок пока нет
- Concept Map 1Документ3 страницыConcept Map 1Rubie Ann TillorОценок пока нет
- PNF Respiration PDFДокумент7 страницPNF Respiration PDFBlake d souzaОценок пока нет
- SOMBILLO Scenario 1 ANGINAДокумент2 страницыSOMBILLO Scenario 1 ANGINAKarla SombilloОценок пока нет
- Atorvastatin Nursing ConsiderationsДокумент11 страницAtorvastatin Nursing ConsiderationsClaire M. AuditorОценок пока нет
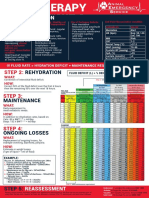
- FLUIDTHERAPY STEP 1: PERFUSIONДокумент1 страницаFLUIDTHERAPY STEP 1: PERFUSIONChristian De Leon100% (1)
- Nerve Cell PPT 1Документ16 страницNerve Cell PPT 1Zhen ObelidorОценок пока нет
- 100 Item Exam On Fundamentals of NursingДокумент19 страниц100 Item Exam On Fundamentals of NursingFilipino Nurses Central100% (1)
- PATHOLOGY MCQsДокумент16 страницPATHOLOGY MCQstaliassalimОценок пока нет
- Musculoskeletal SystemДокумент92 страницыMusculoskeletal SystemBrenda LynОценок пока нет