Вам также может понравиться
- Strategies Epmm CommentДокумент42 страницыStrategies Epmm CommentReyhan IsmОценок пока нет
- (Asian Biomedicine) The Emergence of Lincosamide and Macrolide Resistance in Streptococcus Pyogenes From PakistanДокумент4 страницы(Asian Biomedicine) The Emergence of Lincosamide and Macrolide Resistance in Streptococcus Pyogenes From PakistanReyhan IsmОценок пока нет
- Critical Care Burn Lecture Butler 11-14-06 CondДокумент58 страницCritical Care Burn Lecture Butler 11-14-06 CondReyhan IsmОценок пока нет
- Clinical Practice Guideline: Bell's PalsyДокумент27 страницClinical Practice Guideline: Bell's PalsyReyhan IsmОценок пока нет
- 3020 FullДокумент17 страниц3020 FullReyhan IsmОценок пока нет
- Comparison of Neutrophil CD64 Expression, Manual Myeloid Immaturity Counts, and Automated Hematology Analyzer Fla...Документ12 страницComparison of Neutrophil CD64 Expression, Manual Myeloid Immaturity Counts, and Automated Hematology Analyzer Fla...Reyhan IsmОценок пока нет
- Growth Children With Thalassaemia: Effect of Different Transfusion RegimensДокумент4 страницыGrowth Children With Thalassaemia: Effect of Different Transfusion RegimensReyhan IsmОценок пока нет
- Z Score Boys PDFДокумент15 страницZ Score Boys PDFMuhammad Aldiansyah Januario0% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Extraction of Mangiferin From Mangifera Indica L. LeavesДокумент7 страницExtraction of Mangiferin From Mangifera Indica L. LeavesDaniel BartoloОценок пока нет
- PM 50 Service ManualДокумент60 страницPM 50 Service ManualLeoni AnjosОценок пока нет
- Worked Solution Paper5 A LevelДокумент8 страницWorked Solution Paper5 A LevelBhoosan AncharazОценок пока нет
- 15 Miscellaneous Bacteria PDFДокумент2 страницы15 Miscellaneous Bacteria PDFAnne MorenoОценок пока нет
- Glossary of Blasting TermsДокумент13 страницGlossary of Blasting TermsNitesh JainОценок пока нет
- Leather PuppetryДокумент8 страницLeather PuppetryAnushree BhattacharyaОценок пока нет
- The Anti-PaladinДокумент9 страницThe Anti-PaladinBobbyОценок пока нет
- Philippine Education Deteriorating - EditedДокумент3 страницыPhilippine Education Deteriorating - EditedRukimi Yamato100% (1)
- Thermal Physics Lecture 1Документ53 страницыThermal Physics Lecture 1Swee Boon OngОценок пока нет
- Standard BMW PDFДокумент19 страницStandard BMW PDFIna IoanaОценок пока нет
- Ferobide Applications Brochure English v1 22Документ8 страницFerobide Applications Brochure English v1 22Thiago FurtadoОценок пока нет
- Partnership Digest Obillos Vs CIRДокумент2 страницыPartnership Digest Obillos Vs CIRJeff Cadiogan Obar100% (9)
- HangersSupportsReferenceDataGuide PDFДокумент57 страницHangersSupportsReferenceDataGuide PDFIndra RosadiОценок пока нет
- Quotation - 1Документ4 страницыQuotation - 1haszirul ameerОценок пока нет
- Previews 1633186 PreДокумент11 страницPreviews 1633186 PreDavid MorenoОценок пока нет
- BSRM Ultima BrochureДокумент2 страницыBSRM Ultima BrochuresaifuzzamanОценок пока нет
- An Enhanced Radio Network Planning Methodology For GSM-R CommunicationsДокумент4 страницыAn Enhanced Radio Network Planning Methodology For GSM-R CommunicationsNuno CotaОценок пока нет
- Index: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsДокумент5 страницIndex: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsZidi BoyОценок пока нет
- Punches and Kicks Are Tools To Kill The Ego.Документ1 страницаPunches and Kicks Are Tools To Kill The Ego.arunpandey1686Оценок пока нет
- Pogon Lifta MRL PDFДокумент128 страницPogon Lifta MRL PDFMašinsko ProjektovanjeОценок пока нет
- Clinical Skills TrainingДокумент12 страницClinical Skills TrainingSri Wahyuni SahirОценок пока нет
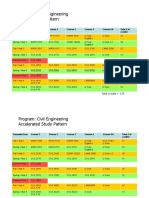
- HKUST 4Y Curriculum Diagram CIVLДокумент4 страницыHKUST 4Y Curriculum Diagram CIVLfrevОценок пока нет
- Fin Accounting IFRS 2e Ch13Документ62 страницыFin Accounting IFRS 2e Ch13Nguyễn Vinh QuangОценок пока нет
- Vendor Registration FormДокумент4 страницыVendor Registration FormhiringОценок пока нет
- 2.ed - Eng6 - q1 - Mod3 - Make Connections Between Information Viewed and Personal ExpiriencesДокумент32 страницы2.ed - Eng6 - q1 - Mod3 - Make Connections Between Information Viewed and Personal ExpiriencesToni Marie Atienza Besa100% (3)
- 6int 2008 Dec AДокумент6 страниц6int 2008 Dec ACharles_Leong_3417Оценок пока нет
- Method Statement FINALДокумент61 страницаMethod Statement FINALshareyhou67% (3)
- Initial Police Report: Calamba City Police Station Brgy Real, Calamba City, Laguna E-Mail: 545-1694/545-6789 Loc 8071Документ1 страницаInitial Police Report: Calamba City Police Station Brgy Real, Calamba City, Laguna E-Mail: 545-1694/545-6789 Loc 8071Jurish BunggoОценок пока нет
- CHN Nutri LabДокумент4 страницыCHN Nutri LabMushy_ayaОценок пока нет
- You Can't Blame A FireДокумент8 страницYou Can't Blame A FireMontana QuarterlyОценок пока нет