Вам также может понравиться
- Jsa - Duck Bank InstallationДокумент10 страницJsa - Duck Bank InstallationAmadeo Sabanal100% (1)
- Aspire Logistics Safetydepartment: Ref. No. AL-SSD-SAF-FRM-02 01 Date 18.07.19 1of6Документ6 страницAspire Logistics Safetydepartment: Ref. No. AL-SSD-SAF-FRM-02 01 Date 18.07.19 1of6Kevin ColmoОценок пока нет
- Jsa - Hot TappingДокумент15 страницJsa - Hot TappingAmadeo Sabanal0% (1)
- RA Existing Asphalt Milling WorksДокумент8 страницRA Existing Asphalt Milling WorksSolimanОценок пока нет
- New Ammend Chemical Register (Draft 2)Документ11 страницNew Ammend Chemical Register (Draft 2)Osh 0717Оценок пока нет
- Full Report Practical 1Документ12 страницFull Report Practical 1Meck LotfiОценок пока нет
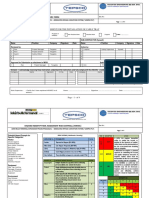
- Biis-Sf-03-Risk Assessment Form-GeneratorДокумент3 страницыBiis-Sf-03-Risk Assessment Form-GeneratorBIIS QAQC Babu SivaОценок пока нет
- RA Bored Cast in Situ PileДокумент38 страницRA Bored Cast in Situ PileAnonymous zsBCtskz100% (1)
- Fire Protection: Effectivity:AllДокумент39 страницFire Protection: Effectivity:All韩建茂Оценок пока нет
- Master - HIRARC Table (Latest)Документ17 страницMaster - HIRARC Table (Latest)Nur Alisha AlishaОценок пока нет
- Hvac WorksДокумент4 страницыHvac WorksSaleem BashaОценок пока нет
- TGPL-AD-HSE01-TEM-HIRA X-Ray 02-1Документ2 страницыTGPL-AD-HSE01-TEM-HIRA X-Ray 02-1Shubham ShuklaОценок пока нет
- Example Industry Hazard Register 2022Документ5 страницExample Industry Hazard Register 2022She-Ra Sha-Ju LaОценок пока нет
- RISKMATRIXДокумент2 страницыRISKMATRIXjohnjovetОценок пока нет
- Risk Management Plan TableДокумент26 страницRisk Management Plan TableJomel medinaОценок пока нет
- RA 023 Risk Assessment - FireДокумент4 страницыRA 023 Risk Assessment - Firethomson100% (4)
- TR - Tax Risk CR-Currency Risk PR - Policy Risk MR - Market Risk IR - Industry Risk RM - Raw Materials Price RiskДокумент2 страницыTR - Tax Risk CR-Currency Risk PR - Policy Risk MR - Market Risk IR - Industry Risk RM - Raw Materials Price Riskneelakanta srikarОценок пока нет
- HSE-F-NEOM-012 - Risk Assessment FormДокумент2 страницыHSE-F-NEOM-012 - Risk Assessment FormAhmed Mohamed100% (1)
- Attachment 1 Risk AssessmentДокумент9 страницAttachment 1 Risk Assessmentjaouad id boubkerОценок пока нет
- RA 021 Risk Assessment - Installation of External Landscape Lighting WorksДокумент13 страницRA 021 Risk Assessment - Installation of External Landscape Lighting Worksthomson50% (2)
- Tdi Hazid TemplateДокумент11 страницTdi Hazid TemplateAnonymous rwojPlYОценок пока нет
- Baseline Risk Assessment1 PDFДокумент25 страницBaseline Risk Assessment1 PDFRico100% (2)
- Chandelier Hoist SystemДокумент10 страницChandelier Hoist SystemNishadh 83Оценок пока нет
- Blank Risk Application MatrixДокумент1 страницаBlank Risk Application MatrixSarfraz EPIC ConsultingОценок пока нет
- Trampoline RMP 2018Документ2 страницыTrampoline RMP 2018api-514548596Оценок пока нет
- 5 Risk Assessment For IRONING 5Документ2 страницы5 Risk Assessment For IRONING 5Anand KumarОценок пока нет
- Risk Management Plan ModelДокумент12 страницRisk Management Plan ModelSamuel DinОценок пока нет
- Ra 02 - Anti-Termite TreatmentДокумент4 страницыRa 02 - Anti-Termite TreatmentHafiz M WaqasОценок пока нет
- Lufkin Risk Assessment 2011 UpdatedДокумент10 страницLufkin Risk Assessment 2011 UpdatedmohammedОценок пока нет
- Risk Assesment Fab - Rev-07Документ71 страницаRisk Assesment Fab - Rev-07Nikhil PuthiryОценок пока нет
- Risk Assessment Road Repair PIC R 7514Документ5 страницRisk Assessment Road Repair PIC R 7514Charles DoriaОценок пока нет
- RA 002forklift OperationsДокумент9 страницRA 002forklift Operationsamrismail2012Оценок пока нет
- JSA HEMP Well Services Pg01-05Документ5 страницJSA HEMP Well Services Pg01-05Ashok SureshОценок пока нет
- Agcurate - Satellite Driven Crop Assurance - Pitch Deck 2021DECДокумент10 страницAgcurate - Satellite Driven Crop Assurance - Pitch Deck 2021DECJelly NiОценок пока нет
- Mine Planning - Its Relationship To Risk Management: O.K.H. Steffen SRK ConsultingДокумент17 страницMine Planning - Its Relationship To Risk Management: O.K.H. Steffen SRK ConsultingJhoan ParedesОценок пока нет
- Likelihood Consequence Risk Level Acceptable Level Risk Treatment SДокумент2 страницыLikelihood Consequence Risk Level Acceptable Level Risk Treatment SDianna Grace AlmacinОценок пока нет
- Risk Assessment Format For SampleДокумент3 страницыRisk Assessment Format For SampleSaqib RasoolОценок пока нет
- 4.1.2 Covid-19 Risk AssessmentДокумент41 страница4.1.2 Covid-19 Risk AssessmentaceОценок пока нет
- HARC Driving 2002Документ4 страницыHARC Driving 2002Moustafa AshrafОценок пока нет
- Dekalb Amarillo Dkc32-12ribДокумент4 страницыDekalb Amarillo Dkc32-12ribYubisay RojasОценок пока нет
- RA 024 Risk Assessment - Precast Concrete WorksДокумент14 страницRA 024 Risk Assessment - Precast Concrete Worksthomson78% (9)
- Covid N95 Decon & Reuse: Hydrogen Peroxide Vapor & Hydrogen Peroxide Gas PlasmaДокумент1 страницаCovid N95 Decon & Reuse: Hydrogen Peroxide Vapor & Hydrogen Peroxide Gas PlasmaDeevish N DinakarОценок пока нет
- Jsa For Installation, Testing and Commissioning of Sewer and Strom Water Drainage System at 14 Nos. of Alijarah Warehouse.Документ67 страницJsa For Installation, Testing and Commissioning of Sewer and Strom Water Drainage System at 14 Nos. of Alijarah Warehouse.jafar mohdОценок пока нет
- Activity Title Boiler: 1. Hazard Identification 2. Risk Analysis 3.risk ControlДокумент12 страницActivity Title Boiler: 1. Hazard Identification 2. Risk Analysis 3.risk Controlizzah80% (5)
- RA 020 Risk Assessment - Risk Assessment - Installation of Cables in Ducts & TrenchesДокумент11 страницRA 020 Risk Assessment - Risk Assessment - Installation of Cables in Ducts & Trenchesthomson100% (1)
- Name of Drug and Classification Ass.Документ7 страницName of Drug and Classification Ass.Nathalie kate petallarОценок пока нет
- RA-Chlorination & Disinfectionof Water Supply SystemДокумент11 страницRA-Chlorination & Disinfectionof Water Supply SystemSanto EОценок пока нет
- Risk Asessment For Rawlplug TestingДокумент9 страницRisk Asessment For Rawlplug Testingadeoye AdeyemiОценок пока нет
- Risk Assessment For COVID-19Документ3 страницыRisk Assessment For COVID-19Ali KaziОценок пока нет
- International Patient SafetyДокумент1 страницаInternational Patient SafetyJery JsОценок пока нет
- Managing Major Accident Hazards Through Sce Management ProcessДокумент4 страницыManaging Major Accident Hazards Through Sce Management ProcessLi QiОценок пока нет
- HSE Risk Assessment For Hot Work ActivityДокумент11 страницHSE Risk Assessment For Hot Work ActivityGokul pОценок пока нет
- Tdi Hazid TemplateДокумент11 страницTdi Hazid TemplateAndi Ade Putra SiregarОценок пока нет
- HSE Risk Assessment For Hot Work ActivityДокумент8 страницHSE Risk Assessment For Hot Work ActivityDarseen RОценок пока нет
- Brown Field TNO 0019 RevДокумент2 страницыBrown Field TNO 0019 RevDaniele GouveiaОценок пока нет
- Risk Assesment - Fire HazardДокумент14 страницRisk Assesment - Fire HazardMohammed Amer PashaОценок пока нет
- PB Hva Kebakaran Unit 1Документ8 страницPB Hva Kebakaran Unit 1cindra RamadaniОценок пока нет
- Hirarc Form: Task/Job Description: Method Statement For The Installation of Cable Tray VALIDITY PERIODДокумент4 страницыHirarc Form: Task/Job Description: Method Statement For The Installation of Cable Tray VALIDITY PERIODMohd Faiz MohdОценок пока нет
- A Human Placenta-Derived Decellularized Connective Tissue Matrix (CTM) Supports Cellular Functions Involved in Wound Healing ProcessesДокумент1 страницаA Human Placenta-Derived Decellularized Connective Tissue Matrix (CTM) Supports Cellular Functions Involved in Wound Healing ProcessesbaoОценок пока нет
- S SmithДокумент1 страницаS SmithbaoОценок пока нет
- Program Guide & Registration: Acfas 2019 Scientific ConferenceДокумент32 страницыProgram Guide & Registration: Acfas 2019 Scientific ConferencebaoОценок пока нет
- A Novel Technique For Repair of An Osteochondral Talar Dome Fracture in A Pediatric Athlete: A Case StudДокумент1 страницаA Novel Technique For Repair of An Osteochondral Talar Dome Fracture in A Pediatric Athlete: A Case StudbaoОценок пока нет
- Beaumont Health Wayne - Foot and Ankle Surgery: Hannah Khlopas DPM PGY 3, Lawrence M. Fallat DPM FACFASДокумент1 страницаBeaumont Health Wayne - Foot and Ankle Surgery: Hannah Khlopas DPM PGY 3, Lawrence M. Fallat DPM FACFASbaoОценок пока нет
- 2016 FINAL Program - 01 - 25 - 16 - Low Res PDFДокумент72 страницы2016 FINAL Program - 01 - 25 - 16 - Low Res PDFbaoОценок пока нет
- Diagnosis and Treatment of Forefoot Disorders. Section 1: Digital DeformitiesДокумент43 страницыDiagnosis and Treatment of Forefoot Disorders. Section 1: Digital DeformitiesbaoОценок пока нет
- Mcglamry: 33 Joint Salvage & Preservation Surgical Techniques For Hallux LimitusДокумент1 страницаMcglamry: 33 Joint Salvage & Preservation Surgical Techniques For Hallux LimitusbaoОценок пока нет
- Foot & Ankle Surg Complications Seminar: ACFAS Tri-State Region PresentsДокумент5 страницFoot & Ankle Surg Complications Seminar: ACFAS Tri-State Region Presentsbao0% (1)
- Mohomad Al-Sawah, Guy Richard Pupp, DPM, FACFAS : DPM Priya Samant, DPM Dustan Mascarenhas, MDДокумент1 страницаMohomad Al-Sawah, Guy Richard Pupp, DPM, FACFAS : DPM Priya Samant, DPM Dustan Mascarenhas, MDbaoОценок пока нет
- DAY Residents: Residency PracticeДокумент5 страницDAY Residents: Residency PracticebaoОценок пока нет
- TH ST ST: You Can Type Out Annotations If More AppropriateДокумент1 страницаTH ST ST: You Can Type Out Annotations If More AppropriatebaoОценок пока нет
- Complications 2016 Seminar: Minimize Your Complications and Maximize Your Patient OutcomesДокумент8 страницComplications 2016 Seminar: Minimize Your Complications and Maximize Your Patient OutcomesbaoОценок пока нет
- Edgardo Rodriguez, DPM Byron Hutchinson, DPM Eric Powell, DPMДокумент1 страницаEdgardo Rodriguez, DPM Byron Hutchinson, DPM Eric Powell, DPMbaoОценок пока нет
- Melody Stouder Class of 2014 TuspmДокумент41 страницаMelody Stouder Class of 2014 TuspmbaoОценок пока нет
- Cotton OsteotomyДокумент16 страницCotton OsteotomybaoОценок пока нет
- FVBДокумент41 страницаFVBbaoОценок пока нет
- The Principles of Intra-Articular Fracture Care: Joseph Schatzker M.D., B.SC., (Med.), F.R.C.S. (C)Документ31 страницаThe Principles of Intra-Articular Fracture Care: Joseph Schatzker M.D., B.SC., (Med.), F.R.C.S. (C)baoОценок пока нет
- 2006 Orthopaedic In-Training Examination: Foot & Ankle QuestionsДокумент34 страницы2006 Orthopaedic In-Training Examination: Foot & Ankle QuestionsbaoОценок пока нет
- Extra ExtraДокумент24 страницыExtra ExtrabaoОценок пока нет
- Distal Femoral Locking Plates For Tibiotalocalcaneal Fusions in The Charcot Ankle: A Retrospective StudyДокумент6 страницDistal Femoral Locking Plates For Tibiotalocalcaneal Fusions in The Charcot Ankle: A Retrospective StudybaoОценок пока нет
- Peter Bellezza DPM, MS Midori Higashi DPM Jeffrey Christensen, DPM, FACFASДокумент1 страницаPeter Bellezza DPM, MS Midori Higashi DPM Jeffrey Christensen, DPM, FACFASbaoОценок пока нет
- My: Devans0123: Daniel - Evans@rosalindfranklin - EduДокумент209 страницMy: Devans0123: Daniel - Evans@rosalindfranklin - EdubaoОценок пока нет
- Primary Subtalar Joint Arthrodesis in The Treatment of Calcaneal FracturesДокумент27 страницPrimary Subtalar Joint Arthrodesis in The Treatment of Calcaneal FracturesbaoОценок пока нет
- Failed Tarsal Tunnel ReleaseДокумент27 страницFailed Tarsal Tunnel ReleasebaoОценок пока нет
- Mini Clinical Examination (Mini-CEX)Документ21 страницаMini Clinical Examination (Mini-CEX)Jeffrey Dyer100% (1)
- Launching The Century of PatientsДокумент26 страницLaunching The Century of PatientsshaniaggrandОценок пока нет
- Introduction To Clinical Pharmacology 9th Edition Visovsky Test BankДокумент7 страницIntroduction To Clinical Pharmacology 9th Edition Visovsky Test BankJeremyBellotdfx100% (18)
- Pneumonia Case StudyДокумент12 страницPneumonia Case StudyCharisse Joy Cudal100% (7)
- CopdДокумент23 страницыCopdCt Miza100% (2)
- Brain Development of Children From 0 To 6 Years How The Brain LearnsДокумент1 страницаBrain Development of Children From 0 To 6 Years How The Brain Learnssyarifah wardah el hilwaОценок пока нет
- Primary Health Care Presentation - Dr. Rasha SalamaДокумент40 страницPrimary Health Care Presentation - Dr. Rasha SalamaSpislgal PhilipОценок пока нет
- ResumedieteticinternshipДокумент1 страницаResumedieteticinternshipapi-208833628Оценок пока нет
- MedDRA N SOPДокумент32 страницыMedDRA N SOPsuri33350% (2)
- PacemakerДокумент63 страницыPacemakerMonish RautОценок пока нет
- John O. Agwunobi MD Mba MPHДокумент1 страницаJohn O. Agwunobi MD Mba MPHStalyn DíazОценок пока нет
- Cardiac Enzyme StudiesДокумент4 страницыCardiac Enzyme StudiesDara VinsonОценок пока нет
- Chapter 4Документ4 страницыChapter 4Niño Dwayne TuboОценок пока нет
- 2009 Final Program PAAO PapersДокумент16 страниц2009 Final Program PAAO PapersMonica MendozaОценок пока нет
- MCQsДокумент95 страницMCQsMarcus GrisomОценок пока нет
- Geuder Instruments Main CatalogueДокумент312 страницGeuder Instruments Main Catalogueophtho india incОценок пока нет
- Agitation and Delirium at The End of Life: "We Couldn't Manage Him"Документ15 страницAgitation and Delirium at The End of Life: "We Couldn't Manage Him"Ivonne Soledad Che PiñeiroОценок пока нет
- Medical CannabisДокумент6 страницMedical CannabisJuvy Balono KansiОценок пока нет
- Pediatric OphthalmologyДокумент12 страницPediatric Ophthalmologyapi-3743483Оценок пока нет
- Corneal Collagen Cross-Linking: A ReviewДокумент12 страницCorneal Collagen Cross-Linking: A ReviewHimawan WidyatmikoОценок пока нет
- Verbal (Non Verbal) Therapeutic Communication Technique Used Rationale and Feelings of Nurse EvaluationДокумент13 страницVerbal (Non Verbal) Therapeutic Communication Technique Used Rationale and Feelings of Nurse EvaluationLei Ortega80% (10)
- YeДокумент39 страницYeRhea RaveloОценок пока нет
- CV Fitri DiktiДокумент12 страницCV Fitri DiktiMilatul AfifahОценок пока нет
- Fulltext PDFДокумент6 страницFulltext PDFMelinda CuraОценок пока нет
- Filamentary KeratitisДокумент3 страницыFilamentary KeratitisRiski SudaenyОценок пока нет
- MCQ1Документ11 страницMCQ1Yuda Lutfiadi100% (1)
- Lesson Plan Personality DisorderДокумент7 страницLesson Plan Personality DisorderRaj MeghwalОценок пока нет
- Test Bank Abnormal Psychology 1st Edition Butcher PDFДокумент60 страницTest Bank Abnormal Psychology 1st Edition Butcher PDFRaiza BettinaОценок пока нет
- Non-Bone Graft Associated Regenerative Periodontal TherapyДокумент80 страницNon-Bone Graft Associated Regenerative Periodontal TherapyGorremuchu Srinivas0% (1)