Академический Документы
Профессиональный Документы
Культура Документы
2015 Adaptações Cardiovasculares Ao Exercício
Загружено:
LeonardoCampanelliАвторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
2015 Adaptações Cardiovasculares Ao Exercício
Загружено:
LeonardoCampanelliАвторское право:
Доступные форматы
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.
75in
Cardiovascular Adaptations to Exercise Training
Ylva Hellsten*1 and Michael Nyberg1
ABSTRACT
Aerobic exercise training leads to cardiovascular changes that markedly increase aerobic power
and lead to improved endurance performance. The functionally most important adaptation is the
improvement in maximal cardiac output which is the result of an enlargement in cardiac dimen-
sion, improved contractility, and an increase in blood volume, allowing for greater filling of the
ventricles and a consequent larger stroke volume. In parallel with the greater maximal cardiac
output, the perfusion capacity of the muscle is increased, permitting for greater oxygen delivery.
To accommodate the higher aerobic demands and perfusion levels, arteries, arterioles, and cap-
illaries adapt in structure and number. The diameters of the larger conduit and resistance arteries
are increased minimizing resistance to flow as the cardiac output is distributed in the body and the
wall thickness of the conduit and resistance arteries is reduced, a factor contributing to increased
arterial compliance. Endurance training may also induce alterations in the vasodilator capacity,
although such adaptations are more pronounced in individuals with reduced vascular function.
The microvascular net increases in size within the muscle allowing for an improved capacity for
oxygen extraction by the muscle through a greater area for diffusion, a shorter diffusion distance,
and a longer mean transit time for the erythrocyte to pass through the smallest blood vessels.
The present article addresses the effect of endurance training on systemic and peripheral cardio-
vascular adaptations with a focus on humans, but also covers animal data. © 2016 American
Physiological Society. Compr Physiol 6:1-32, 2016.
Introduction in the muscle is increased many-fold. Shear stress is sensed by
mechanosensors on the endothelial cells leading to an acute
It has long been known that endurance training leads to adap- increase in vascular conductance but, more importantly, it also
tations in the cardiovascular system (61). Human studies in influences the expression of proteins in the vascular wall of
the 1960s and onward demonstrated that endurance train- significance for vascular function and vascular growth. Both
ing results in increases in cardiac output, increased vascular changes in arterial dimensions, and growth of arterioles and
conductance, a greater perfusion capacity of the muscle, and capillaries are believed to be highly influenced by shear stress.
a greater oxygen extraction, with a consequent increase in The present article discusses evidence for adaptations in
aerobic power (378, 380). At this time, the muscle biopsy the cardiovascular system in response to endurance training
technique was also beginning to be used in humans allow- and takes the reader through adaptations and related mech-
ing for determinations of peripheral adaptations in the trained anisms in cardiac muscle, blood, arterial structure, and the
skeletal muscle and revealing an increased oxidative capacity microvasculature in skeletal muscle but also briefly touches
and increased capillary density in trained muscle (8, 29). In upon adaptations in tissues other than the active muscle. The
the 1980s, Bengt Saltin and colleagues developed the single- review has a focus on humans but also includes data from
leg knee extensor model and used it in combination with animal studies.
the thermodilution technique to assess skeletal muscle blood
flow (7, 9) and provide further evidence for the theory of
a central limitation in oxygen transport capacity (62, 76).
Since this time period and partly with the use of these meth- Central Adaptations to Exercise Training
ods, a large number of studies have addressed the effects of Cardiac adaptations to exercise training
endurance training on adaptations in the cardiovascular sys-
At the onset of exercise, heart rate and stroke volume increase
tem and the underlying mechanisms. Such studies have pro-
so that cardiac output closely matches the metabolic demand
vided insight specifically into the dimensional and functional
of the working skeletal muscles (182, 289). Cardiac output,
improvements in the heart and how vascular function and the
macro and microvascular growth is affected by endurance * Correspondence to yhellsten@nexs.ku.dk
training. In terms of mechanisms, it has clearly been shown 1 Department of Nutrition, Exercise and Sports, University of
that shear stress is a central factor in vascular adaptations Copenhagen, Copenhagen, Denmark
to training. Shear stress, which is the force that the blood Published online, January 2016 (comprehensivephysiology.com)
applies to the endothelial cells as it flows through the blood DOI: 10.1002/cphy.c140080
vessel, is enhanced during endurance training when perfusion Copyright © American Physiological Society.
Volume 6, January 2016 1
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
the product of heart rate (beats min−1 ) and stroke volume characteristics of the LV in trained subjects. Accordingly,
(mL min−1 ), may increase from ∼5 L min−1 at rest to ∼15 increased LV end-diastolic diameter (331, 333, 361), LV wall
L min−1 in young females (449) and ∼20 L min−1 in young thickness (333, 361) and LV mass (333, 338) have consis-
males (288, 378) and up to ∼25 to 30 (449) and ∼35 to 40 L tently been reported in endurance athletes. The most extreme
min−1 (103) in elite female and male athletes, respectively, cavity dimension and/or wall thickness have been reported
during maximal exercise engaging a large muscle mass. This in elite male rowers, cross-country skiers, cyclists and swim-
pronounced effect of exercise training on maximal cardiac mers with large body sizes (331,333,410). The findings on LV
output would be expected to entail a structurally and func- end-diastolic diameter have been confirmed in longitudinal
tionally improved heart in the trained state. This cardiac train- training studies in which rowing for 7 months (453) and pro-
ing adaptation was first described more than 100 years ago fessional cycling for 3 years (2) were associated with increases
by Henschen (179), using only a basic physical examina- in cavity dimension of LV (from 51.5 to 53.3 mm and from
tion with careful percussion to identify enlargement of the 58.3 to 60.3 mm, respectively). Furthermore, one year of
heart due to athletic activity in cross-country skiers. Hen- progressive endurance exercise training performed by previ-
schen concluded that dilatation and hypertrophy of the left ously sedentary male and female subjects lead to increases
and right side of the heart were present in trained individuals in LV mass and LV end-diastolic volume (13). Interestingly,
(179). The use of chest radiography in the 1950s and 1960s the LV responded to the initiation of training (0-6 months,
(350, 367) and development and technological refinement of lower intensity training) with an increase in LV mass without
echocardiography throughout the 1970s and 1980s have pro- a change in LV end-diastolic volume whereas additional three
vided the methodology for a detailed evaluation of training- months of training (high-intensity interval) lead to an increase
induced morphologic and functional changes in the trained in LV end-diastolic volume which restored the baseline mass-
heart. Accordingly, increased end-diastolic dimensions of the to-volume ratio (13).
right (RV) and left ventricle (LV), LV hypertrophy, increased The hemodynamic changes that occur during exercise
LV mass, and increased volume of the left atrium (LA) are constitute the primary stimulus for cardiac remodeling.
now well-established hallmarks of what has been defined as Accordingly, exercise can be separated (although consider-
the athlete’s heart. With regard to the dimensions of the heart, able overlap exists) into two principal forms of physical
it should be noted that body size has a large influence on activity: (i) endurance exercise characterized by sustained
heart size and when comparing absolute dimensions between elevations in cardiac output with reduced peripheral vascular
subjects one should take this variable into account. For this resistance (i.e., long-distance running, cycling, rowing, and
reason, women in general have smaller cardiac dimensions swimming) and (ii) strength training characterized by short
compared to men (332). but intense bouts of increased peripheral vascular resistance
The increase in heart rate is responsible for the major- and only slightly elevated cardiac output (i.e., weightlifting,
ity of cardiac output augmentation during exercise. How- track-and-field throwing events). The notion that these over-
ever, maximal heart rate is relatively unaltered with exer- all differences in cardiac loading with either endurance or
cise training, with some evidence indicating that heart rate strength training lead to different exercise-induced adapta-
may be reduced during maximal exercise with training (463). tions in cardiac structure was first introduced in 1975 (286).
Consequently, the large increase in cardiac output associ- In this study (286), athletes exposed to endurance train-
ated with exercise training is the result of a larger stroke ing demonstrated eccentric LV enlargement (increased LV
volume. Stroke volume rises during exercise as a result of end-diastolic volume and mass) whereas athletes exposed
increases in LV end-diastolic volume and, to a lesser extent, to strength training demonstrated concentric LV hypertro-
sympathetically mediated reduction in end-systolic volume. phy, characterized by normal LV end-diastolic volumes, but
LV end-diastolic volume is determined by diastolic filling, increased wall thickness and mass. Recent systematic reviews
which is determined by a complex interplay between heart and meta-analysis suggest that the magnitude of eccentric LV
rate, intrinsic myocardial relaxation, ventricular compliance, hypertrophy that results from endurance exercise training is
ventricular filling pressures, atrial contraction and pericardial typically more pronounced than the concentric hypertrophy
and pulmonary constraints (18). An increase in stroke volume that accompanies strength training (18, 443).
with exercise training could, therefore, potentially be a result Changes in LV function have been extensively evaluated
of changes in one or more of these variables. in trained individuals. Endurance training leads to enhanced
early diastolic LV filling (19,307,337) and a more rapid filling
of the heart during high-intensity exercise (109). This rapid
The left ventricle
filling is the result of mechanical restorative forces due to
The majority of data characterizing left ventricular structure the remodeling of the heart, which markedly augment the
and function in trained individuals comes from cross-sectional transmittal intraventricular pressure gradient whereby blood
studies. Although this approach does not allow for definite is rapidly sucked from the LA into the apex of LV (462).
conclusions regarding the temporal nature and dose-response This diastolic suction and hence rapid filling of LV is likely to
relationship between exercise and cardiac remodeling, find- explain the observation that there is a continuous rise in stroke
ings from these studies have provided valuable insight on volume in highly trained endurance individuals (132, 467) as
2 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
opposed to less active and sedentary subjects who display a (A) 200
plateau around 40% to 50% of VO2max (15,132). In addition to
diastolic suction, cardiac chamber compliance has also been
shown to be enhanced in athletes, resulting in a large end-
diastolic LV volume and a greater use of the Frank-Starling
Heart rate (bpm)
mechanism (257). Notably, one year of progressive exercise 150
training was only associated with a modest increase in LV
distensibility and compliance and these posttraining values
were substantially below that observed in elite athletes (13). In
contrast to diastolic function, systolic function as assessed by Elite
100 Trained
LV ejection fraction, is generally normal among athletes (18) Untrained
and the rate of ventricular emptying plays only a modest role
in the augmentation of stroke volume during exercise (132). 0
Collectively, the adaptations in LV diastolic function are the (B) 0 2 4 6 8
225
primary mechanisms underlying the larger LV end-diastolic
volume and hence larger stroke volume in trained subjects.
200
Myocardial blood flow per gram of tissue is lower in
Stroke volume (mL)
highly trained endurance athletes both at rest (171, 172) and
during exercise performed at the same absolute workload 175
(171,239) and athletes have higher myocardial oxygen extrac-
tion facilitated by longer blood mean transit time (171). Evi- 150
dence from animal studies suggests that a larger capillary sur-
face area and a more efficient blood flow distribution through 125
the myocardium contribute to the increased oxygen extrac-
tion in the trained heart (245). Moreover, myocardial O2 per 100
gram of tissue at rest and during exercise at the same abso- 0
lute workload is lower in athletes (171). Collectively, these 0 2 4 6 8
(C) 40
findings suggest that the improved cardiac pump function with
training is related to a larger circulatory and metabolic reserve.
Cardiac output (L min–1)
30
The right ventricle
Endurance exercise of moderate to high intensity requires 20
that both the LV and RV receive and eject large quantities
of blood and without any significant shunting both cham-
bers will inevitably have to enhance structure and function 10
to a somewhat similar extent. In accordance with this con-
cept of balanced, biventricular enlargement, RV enlargement
has been shown to parallel LV enlargement (387, 388). The 0
impact of strength training on the RV remains uncertain due 0 2 4 6 8
to inconsistent and limited data (18). Systemic VO2 (L min–1)
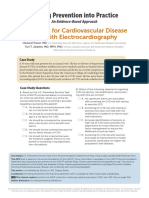
Figure 1 Heart rate (A), stroke volume (B), and cardiac output (C)
The left atrium in relation to systemic V̇ O2 in untrained and trained subjects and elite
athletes.
Several small cohort studies were the first to report LA
enlargement in trained athletes (167, 189). This structural
adaptation is in line with later observations (81, 195) and at rest is largely unaffected by exercise training (26,415), and
cumulative lifetime exercise training hours have been shown the bradycardia is, therefore, likely secondary to the training-
to be an important determinant of LA size (454). induced increase in stroke volume. The autonomic mecha-
nisms underlying the decrease in heart rate at rest is a result
of an increase in vagal tone and a decline in the intrinsic heart
Cardiac output: From rest to maximal exercise
rate, while a reduction in sympathetic activity has minimal
One of the hallmarks of cardiovascular training is a lower- impact (366, 405).
ing of heart rate at rest (sinus bradycardia) and during exer- The increase in heart rate following exercise onset is medi-
cise at any absolute level of submaximal oxygen uptake (35) ated by a combination of vagal withdrawal and β-adrenergic
(Fig. 1). Systemic oxygen demand and hence cardiac output stimulation (123, 359) and an essentially linear relationship
Volume 6, January 2016 3
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
35 3.0 for preservation of a large end-diastolic volume and stroke
MSNA
Venous norepinephrine volume (103, 132), of which the latter may exceed that of
Venous norepinephrine (ng mL–1)
30 2.5 sedentary subjects by ∼60% to 70% during maximal exercise
(54, 103, 467). Such an advantageous functional consequence
MSNA (burst min–1)
25
2.0
of an increased filling time is in line with that restrictions in
20
filling time appear to compromise ventricular filling, stroke
1.5
15 volume, and cardiac output during maximal exercise in trained
1.0 individuals (303).
10 The capacity to produce a very high power output for
5 0.5 a prolonged period of time is essential for endurance per-
formance. To support the very high rates of oxygen uptake
0 0.0 required, the heart must generate a high cardiac output that
Untrained Trained
is achieved by a large stroke volume. This training-induced
Figure 2 Skeletal muscle sympathetic nervous activity (MSNA) during increase in stroke volume is in turn mediated predominantly
knee-extensor exercise and venous norepinephrine concentrations dur- by a large LV end-diastolic volume.
ing cycling exercise in the untrained and trained state. MSNA was mea-
sured by microneurography in the resting leg. Adapted from (346) and
(457) with permission of the American Physiological Society. MSNA =
Muscle sympathetic nerve activity.
Blood Volume Response to
Exercise Training
exists between relative workload and heart rate during exer-
cise that is independent of training status (35, 122). Simi- During exercise, plasma volume is acutely reduced in propor-
lar to resting conditions, cardiac output at a given absolute tion to metabolic and/or thermal demands and the resulting
submaximal workload is not significantly different follow- loss in plasma volume is accompanied by increased electrolyte
ing exercise training as oxygen demand is also unaltered concentrations and osmolality that leads to activation of the
(26, 415). The unchanged cardiac output is the result of a renin-angiotensin-aldosterone cascade and ultimately renal
larger stroke volume and lower heart rate (132, 415). The water retention (71). Exercise training leads to an expansion
mechanisms underlying the lower heart rate during submax- of blood volume (hypervolemia) via an aldosterone-sodium
imal exercise are still unclear but are likely to be related to retention mechanism along with increases in plasma albumin
both autonomic and nonautonomic factors. Exercise training content (70). Cross-sectional data have shown that exercise
results in diminished sympathetic drive for a given level of training is associated with a 20% to 25% larger blood vol-
exercise (75, 346, 405, 457) (Fig. 2) whereas training does not ume in trained individuals and ∼50% larger blood volume
appear to induce a decrease in vagal tone during exercise. In in elite athletes compared to untrained individuals (69, 170)
addition, some evidence has been provided for that increases (Fig. 3). The fast rate at which exercise-induced hypervolemia
in heart volume lowers intrinsic heart rate (224, 258). The occurs is demonstrated by the fact that one single exercise
increase in stroke volume during exercise at a given abso- bout can increase blood volume by 10% to 12% within 24
lute workload in the trained state is a result of an increase h (130, 341). The hypervolemia appears to reach a plateau
in blood volume, an augmented left ventricular end-diastolic at around 10 to 14 days of training and virtually all of this
volume, and cardiac preload (198,236) as well as a lower car- increase in blood volume is due to increased plasma vol-
diac afterload (arterial pressure) (132,296). Notably, evidence ume as erythrocyte mass does not change significantly within
suggests that cardiac output during exercise is regulated by this timeframe (69). As training continues, erythrocyte vol-
peripheral oxygen demand (16, 156) and that this regulation ume expansion is observed and increases (with most of the
is independent of training status (296). effect observed within 30 days) until plasma and erythrocyte
To what extent heart rate during maximal exercise is volume is 8% to 10% above the pretraining level (69). The
altered with exercise training remains a topic of debate. Never- result is a hematocrit that returns to an only slighter lower
theless, maximal heart rate has been reported to be decreased level than before training initiation (385). A modestly lower
by 3% to 7% with training in a large number of studies (463). hematocrit with training is in congruence with cross-sectional
At least some of the mechanisms underlying a decrease in data demonstrating that athletes have ∼1% lower hematocrit
maximal heart rate are likely to be similar to those underlying than sedentary controls (170). Whereas the control of erythro-
resting and submaximal bradycardia. One such mechanism poiesis in hypoxia and anemic hypoxia is well understood, the
could be a receptor downregulation as β-adrenergic blockade signals stimulating erythropoiesis upon training in normoxia
has been shown to abolish the difference in maximal heart are unclear, but may involve an exercise-induced increase in
rate between sedentary and trained subjects due to a less sig- androgens that stimulate erythropoietin (EPO) release and
nificant reduction in heart rate in the trained subjects (215). an increase in catecholamines and cortisol that stimulate the
From a functional perspective, a lower maximal heart rate will release of reticulocytes (immature erythrocytes) from bone
allow for increased filling time, which is likely to be important marrow and possibly EPO release (271).
4 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
(A) 10 and stroke volume. Reestablishing blood volume to a level
similar to that observed before a 6-week training interven-
tion by phlebotomy, abolished the training-induced change in
8
maximal cardiac output, suggesting that the training-induced
Blood volume (L)
change in maximal cardiac output following a short period of
6 exercise training is a consequence of an increase in blood vol-
ume (39). Furthermore, a large part of the difference in stroke
4 volume between trained and untrained has also been sug-
gested to be related to differences in blood volume (198,236).
2 Exercise training also activates de novo protein synthesis and
leads to a more dilute sweat. These adaptations will help to
0
compartmentalize fluid within the vascular space which will
(B) 5 5 help to keep blood volume normal via fluid shifts during peri-
ods of sweat loss, due to elevations in oncotic pressure and
Erythrocyte volume
Plasma volume
intravascular electrolyte levels (69).
4 4
Hemoglobin is an excellent buffer, and an increase in
Erythrocyte volume (L)
Plasma volume (L)
hemoglobin mass enhances the buffering capacity of the
3 3 blood (58). The training-induced increase in hemoglobin mass
could, therefore, potentially facilitate a higher lactate and pro-
2 2 ton release from active skeletal muscle due to a higher diffu-
sion gradient from the interstitium to the blood and improve
1 1 the capacity to produce energy via anaerobic pathways. How-
ever, experimental data for such an effect is lacking.
0 0
Indications of the performance enhancing effects of the
training-induced increase in erythrocyte mass, plasma and
(C) 50
blood volume can be seen from studies where blood has
been drawn and then reinfused after several weeks to increase
these variables (also known as blood doping). Accordingly, an
improvement in VO ̇ 2max and endurance performance (longer
Hematocrit (%)
45 exercise time at a given workload, greater mean power output
or speed during a time trial) with this intervention has been a
general finding (47,102,439,455). Notably, blood doping also
increases hematocrit and hence the oxygen carrying capacity
of the blood, which is in contrast to the normal physiolog-
40 ical training response where hematocrit is slightly lowered
(170), and care should, therefore, be taken when extrapo-
0
Untrained Trained Elite lating findings from these studies. Nevertheless, data from
trained endurance athletes suggests that the increase in ery-
Figure 3 Blood volume (A), erythrocyte and plasma volume (B), and throcyte mass (208, 385) and plasma and blood volume (266)
hematocrit (C) in untrained and trained subjects and elite athletes.
are important training adaptations for endurance exercise
performance.
The hypervolemia associated with exercise training
reflects a larger total body water volume (68) which increases
interstitial fluid available to the sweat glands and allows for a
greater plasma volume to perfuse skin to enhance conductive Effect of Exercise Training on
heat exchange. Accordingly, hypervolemia following exercise Blood Pressure at Rest and
training is related to increased sweat rate and evaporative cool- During Acute Exercise
ing during exercise (68, 70). In addition to thermoregulatory
advantages, hypervolemia and the associated lower hema- The long-term control of blood pressure has been recognized
tocrit and blood viscosity have been proposed to decrease as a complex mixture of neural, hormonal and intrinsic fac-
the workload of the heart (104) due to a greater filling of tors involving the brain, heart, vasculature, and especially the
the heart and lower peripheral resistance. Studies employing kidneys due to its control of fluid balance. In a mathemati-
acute expansion of blood volume by intravenous infusion of cal model composed of hundreds of equations, Guyton and
dextran (198, 236) or albumin (115) have demonstrated that co-workers proposed that a volume increase in the vascular
increased blood volume significantly influences cardiac per- system would lead to an increase in blood pressure (157).
formance by increasing cardiac preload, ventricular filling Nevertheless, despite the effects of training on blood volume
Volume 6, January 2016 5
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
it is well established that endurance training reduces blood reduced arterial wall thickness and an increased lumen diam-
pressure at rest in both normotensive and hypertensive sub- eter (147, 302).
jects, with a more pronounced effect in hypertensive sub- The function of conduit and resistance arteries is to allow
jects (73). The mechanisms underlying this effect of exercise for transport of blood from the heart to the different organs
training remain undisclosed, but are likely to be multifacto- and the diameter and elastic properties of these arteries should
rial and include vascular remodeling (169) and/or changes optimally be adequate so as not to limit the blood flowing from
in peripheral vascular function (419), sympathetic nervous the heart. In general, although the diameter of larger resis-
activity (73, 244, 300), function of the nitric oxide (NO) and tance arteries may contribute to overall vascular resistance,
prostanoid system (315), and the renin-angiotensin system the greatest resistance is located further down in the smaller
(73). With regard to the sympathetic nervous system, the role arterioles within organs, thus structural changes at this level
of skeletal muscle sympathetic nervous activity (MSNA) for may be more important.
the training-induced reduction in blood pressure is likely to be In comparing muscle blood flow during intense exercise
limited as training does not reduce MSNA at rest (393). Inter- with a smaller versus larger muscle mass, it is clear that per-
estingly, in healthy older humans exercise training has even fusion of muscle during whole body exercise is limited by the
been shown to be associated with elevated basal MSNA (310). magnitude of the cardiac output (52,377,395,446). Therefore,
Exercise training leads to a reduction in blood pressure as cardiac output is increased with endurance training, the per-
and sympathetic drive during acute submaximal exercise per- fusion capacity of the muscle increases during intense exercise
formed at the same absolute intensity when muscles of the with larger muscle groups (377), but maximal perfusion dur-
lower limb are recruited (75,110,296,346,457) (Fig. 2). Con- ing one-leg exercise, for which there is no central limitation,
versely, exercise training does not appear to affect the MSNA is also increased (353). To accommodate the higher perfu-
response when forearm exercise is performed (393), suggest- sion rates, the arteries undergo structural adaptations leading
ing that the effects of exercise training on MSNA during to an increased diameter and reduced wall thickness and the
exercise may be related to the limb and/or the size of muscle volume of the arteriolar net is increased.
mass engaged in exercise. The effect of training on MSNA
could be related to alterations in both central command and
Effects of training on arterial diameter
the pressor response originating from the contracting skeletal
muscle as both influence sympathetic nervous activity (282). Conduit arteries Conduit artery dimensions can be
The pressor response is thought to be the result of affer- assessed by ultrasound Doppler technique with good accuracy
ent input coming from group III and IV fibers that respond in humans (426). Cross-sectional studies comparing differ-
to mechanical distortion and changes in the chemical envi- ent groups of athletes including tennis players, road cyclists,
ronment, respectively (225). A lower skeletal muscle lactate runners, and wheel-chair athletes with sedentary individu-
production associated with exercise training could be one als, have demonstrated that the diameter of muscular conduit
important chemical influence as in animal models, blockade arteries is larger in trained than untrained muscle (90,200,372,
of acid sensitive ion channels has been shown to attenuate 389). This observation also holds true for intraindividual com-
the pressor response (168) and a relationship between pH parisons of the dominant and nondominant arm of tennis play-
and sympathetic nervous activity has been reported (445). ers (200), for the preferred arm of squash players (371) and
Furthermore, training also reduces central command output for trained below knee one-leg amputees (200). In accordance
as evidenced by attenuation of the blood pressure and heart with the findings from cross-sectional studies, longitudinal
rate response to acute exercise in the contralateral untrained studies provide evidence for that a period of aerobic training
limb (110). As previously described, heart rate is lower during of 6 to 12 weeks is sufficient to increase the diameter of the
exercise engaging a trained muscle group. Despite this effect femoral artery (90, 283). In further support of a relationship
on heart rate, stroke volume still remains higher in the trained between training and conduit artery dimensions is the obser-
state which primarily is the result of the lower arterial blood vation that femoral arterial diameter and maximal oxygen
pressure and hence cardiac afterload (296). uptake correlate well (r = 0.91) in young healthy men (345).
Some studies on human coronary arteries (183, 234) have
shown that the resting diameter of endurance trained individu-
Arterial Remodeling in Response to als is similar to that of sedentary individuals. However, Pelic-
Exercise Training cia and co-workers reported a relationship between coronary
artery diameter and cardiac dimension in top-level athletes,
It is well established that changes in hemodynamic forces, indicating a training-induced enlargement of coronary arter-
including shear stress and transmural pressure, can lead to ies, although it should be kept in mind that a genetic contribu-
remodeling arteries and arterioles (1,45,268,302). In humans, tion cannot be excluded in such measurements (334). More-
some of the clearest evidence for remodeling is observed in, on over, at a functional level, the increase in coronary diameter
one hand, individuals with hypertension who have increased with either the NO donor nitroglycerin (166), adenosine infu-
arterial wall thickness and reduced lumen diameter and, on sion (183), or dipyridamole, an inhibitor of adenosine uptake
the other hand, endurance trained individuals who display a (234), has been found to be greater in endurance athletes than
6 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
in sedentary subjects, indicating a greater flow reserve. In lon- increased after a 12-week period of endurance training (44)
gitudinal studies, a period of endurance training has accord- and, in rats, a higher cast weight of coronary arterioles was
ingly been shown to increase coronary flow reserve in healthy observed after a period of endurance training (186).
individuals (456) and patients with coronary disease (158).
Effects of training on arterial wall thickness
Resistance arteries
Most studies on the effect of endurance training on wall thick-
In contrast to conduit arteries, resistance artery dimensions ness suggests that wall thickness is reduced with training both
cannot be directly measured but have instead been estimated in the forearm and leg (90,372,373,427) although an increased
from measurements of maximal flow changes in response to a arterial wall thickness in parallel with an increase in arterial
period of ischemia (112, 404, 421). The method estimates the diameter has been reported (389).
dimensions of the whole resistance vasculature and assumes Exercise training that induces large increases in blood
that absolutely maximal flow capacity is achieved after the pressure such as heavy load resistance training, is likely to
ischemic period and that there therefore is no functional limi- have an impact on the arterial wall thickness similar to that
tation to the measurements. This assumption could leave some observed with hypertension (302). Data on the effect of resis-
uncertainty as to whether maximal flows actually have been tance training on arterial dimensions is sparse (34) but it has
achieved in all studies. However, evidence has been provided been shown that resistance training increases wall thickness
for that the training-induced increase in maximal response without an equivalent effect on diameter leading to a higher
with this method is not necessarily paralleled by an increased wall thickness to diameter ratio (389).
capacity of vasodilator systems (140, 145) and the response A functional consequence of a change in wall thick-
does not appear to be affected by sympathetic drive (421). ness is a change in compliance. Several studies have
Endurance training has been observed to increase the max- shown that endurance training increases arterial compliance
imal vasodilator capacity, as assessed by ischemia with or (53, 229, 284) whereas strength training can reduce arterial
without added exercise. Sinoway and coworkers reported a compliance (31). However, alterations in arterial compliance
greater peak vasodilator response in the dominant arm of with training may also be related to changes in the wall com-
tennis players (402) and a maximal vasodilator response has position (214, 274). Functionally, an improved compliance in
been described after a period of forearm training in previously the large elastic arteries dampens the pulse pressure and is
untrained individuals (140, 143, 403). In the leg vasculature, important for maintaining flow high in the diastolic phase
a higher maximal flow capacity was observed in endurance also at high stroke volumes (the windkessel effect) (119).
trained than in sedentary individuals (407).
In laboratory animals, not only the dimension but also the
Hemodynamic signals affecting arterial remodeling
number of arteries and arterioles can be directly assessed by
methods including vascular casting and immunohistochemi- An important hemodynamic variable for the increase in lumi-
cal differentiation of blood vessels. By use of vascular casting, nal diameter of arteries is shear stress (240, 335, 440). Shear
Laughlin and co-workers compared the effect of endurance stress is the frictional force on the endothelium applied by the
training and interval sprint training on the number of arterioles blood as it flows through the vessel. Shear stress is elevated
in skeletal muscle groups of different fiber types in rats (246). when blood flow increases without a compensating change in
Their data showed that not only both endurance and sprint vessel diameter. In particular in smaller resistance vessels an
training-induced growth of smaller arterioles but also that increase in shear stress will induce formation of vasodilators
growth differed depending on fiber type. Based on their find- leading to increased arteriolar diameter that neutralizes the
ings, the authors concluded that arteriolar growth occurred in shear stress. However, despite this dilatory effect, shear stress
the muscles mainly used during the training, that is, endurance is a central signal for vascular remodeling at all levels of the
training primarily leads to arteriolarization in oxidative and arteriolar tree. The clearest evidence for shear stress being an
fast oxidative glycolytic fibers (246). The authors also specu- important factor in expansion of the luminal diameter stems
lated that the increased arteriolarization after endurance train- from animal studies showing that interventions such as arterial
ing (246) could be a contributing factor for their previously ligation with arteriovenous shunting, leading to increased flow
observed 50% increase in flow capacity as assessed by differ- through the collateral arteries, results in a profound increase
ent levels of perfusion pressure (248). It may be mentioned in arterial diameter of these arteries (101, 386).
that fiber-type specific adaptations in the microvasculature in The shear stress induced enlargement of arteries is likely
rats are not so easily translated into humans as much of human to, at least in part, be mediated by NO. Shear stress leads
locomotor muscle, including the most commonly examined to both an acute increase in NO formation (374) and an
vastus lateralis muscle, has a less uniform distribution of fiber upregulation of endothelial nitric oxide synthase (eNOS)
types (259). (24, 440, 458). Inhibition of NO has been reported to abolish
Coronary arteriolar dimensions have also been shown to both shear stress induced increase in carotid artery diameter
be increased with endurance training. In a study on pigs, the (435) and the exercise training-induced increase in collateral
numerical and length densities of coronary arterioles were flow in skeletal muscle (265). NO in turn interacts closely with
Volume 6, January 2016 7
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
vascular endothelial growth factor (VEGF) which is known to compounds that directly reduce the effect of the sympathetic
be important in arteriogenesis (263). The interaction between activity. The below sections discuss how training may alter
NO and VEGF is bidirectional; NO promotes VEGF expres- exercise hyperemia and the mechanisms underlying vasodi-
sion (82,128,216) but VEGF can also promote NO formation latation in skeletal muscle.
(304,328). It should, however, be emphasized that, in addition
to VEGF and NO, a vast number of compounds are affected
Blood flow at submaximal workloads
by shear stress and several of these may influence arterial
growth (96, 459). Blood flow to the muscle during submaximal exercise has
Arterial wall thickness, has been reported to be dependent been shown to be either unaffected (26, 315), reduced
on vasoconstriction (21, 94), increased sympathetic influence (228, 315, 339), or even increased with exercise training
(89), and changes in transmural pressure (112, 422). Trans- (28, 237). The discrepancy between findings is not clear but
mural pressure, which is the difference between the pressure may partly reflect the use of different subject groups. In the
inside and outside of the vessel, is elevated with increased study by Nyberg et al. (315) it was found that blood flow
blood pressure. Although systolic arterial blood pressure is during submaximal exercise performed at the same abso-
increased during endurance exercise, the increase is limited lute workload was reduced in normotensive subjects whereas
and the effect on diastolic and mean arterial blood pressure is it was unaltered in hypertensive subjects after 8 weeks of
small (62). In contrast, high load resistance exercise leads to endurance training. Similarly, the study by Beere and co-
pronounced blood pressure changes, in particular resistance workers reported unaltered submaximal blood flows after
exercise with large muscle groups during which systolic blood training in young but higher submaximal flows after train-
pressure can exceed 300 mmHg. Severe resistance training ing in aged (26). It appears plausible that subjects that have
may also lead to permanent elevations in resting blood pres- impaired submaximal blood flows at the onset of training may
sure (389) which could contribute to increased vascular wall experience improvements in vasodilator capacity that cancel
thickness. It has been proposed that a more chronic increase out the peripheral adaptations leading to reduced submaximal
in blood pressure may have a greater impact on arterial wall blood flows.
thickness compared to the transient increases that occur dur- One frequently observed outcome of endurance training,
ing exercise (147). that likely affects the magnitude of blood flow to the muscle
To conclude, existing studies clearly show that exercise during submaximal exercise, is an increased a-v O2 extrac-
training can modify the structure of larger arteries with the tion, which in part occurs as a result of an increased cap-
most noticeable change being an increased luminal diameter illarization and thereby improved oxygen diffusion capacity
and a reduced wall thickness in response to endurance (220, 233, 380) (Fig. 4). Another training-induced adaptation
training. An additional adaptation is an increase in the size that may influence the level of blood flow to the active muscle
of the arteriolar tree. The stimulus for an increased vascular is an improved distribution of flow within the active limb.
diameter and arteriolar growth is thought to be primarily an Improved flow distribution may result from a more optimal
increase in shear stress. The functional consequence of an vascular architecture or a more precise neural control of blood
increase in arterial diameter is reduced resistance during high flow, with a consequent smaller portion of the blood being
levels of perfusion, whereas changes in wall thickness and distributed to nonactive muscle (380, 381). An improved dis-
wall composition have implications for vascular compliance. tribution of flow is not easily determined but studies using
positron emission tomography indicate that endurance trained
individuals have less inhomogeneous blood flow distribution
during exercise (219, 220). Very low femoral venous oxygen
Peripheral Adaptations to levels during maximal exercise have been observed in aged
Exercise Training life-long endurance trained individuals (Mortensen and Saltin,
unpublished observation) and although there may be several
The effect of training on blood flow responses to explanations for this observation, the possibility of an opti-
submaximal and maximal exercise mized microvascular architecture combined with improved
During exercise, blood flow to skeletal muscle can increase flow distribution is intriguing.
up to almost 100-fold from rest to accommodate the increased
demand for oxygen by the contracting muscle. This elevation
Maximal blood flow
in blood flow is achieved by an increased cardiac output in
combination with an enhancement in vascular conductance in It has long been known that endurance training leads to an
the active muscle. The increase in cardiac output upon initia- increase in exercise-induced maximal perfusion of skeletal
tion of exercise is mainly driven by an increase in sympathetic muscle (35, 255, 378). The earlier determinations were con-
activity, which also induces an increase in vasoconstrictor ducted with xenon clearance methods during cycling exer-
tone in most organs. In the active muscle, the increased sym- cise and although they revealed a higher level of maximal
pathetic vasoconstriction is overcome by local formation of blood flow in trained compared to untrained individuals the
a number of different vasodilators but also by sympatholytic overall blood flow levels were unrealistically low (62, 255).
8 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
(A) 3.0 160
Submaximal intensity
a-vO2 difference (ml L–1)
140
Blood flow (L min–1)
2.5
120
2.0 100
0.0 0
(B)
10 180
Maximal intensity
Blood flow
a-vO2 difference 160
a-vO2 difference (ml L–1)
8
Blood flow (L min–1)
140
6
120
4 100
0 0
Immobilized Untrained Trained
Figure 4 Femoral arterial blood flow and arterio-venous O2 difference during submaximal (A)
and maximal (B) single leg knee-extensor exercise with a previously immobilzed leg, untrained
and trained leg. Immobilization lasted for 2 weeks and was achieved by casting. Blood flow was
determined by ultrasound Doppler methodology, arterio-venous oxygen extraction was obtained
by measurements of oxygen content in blood drawn simultaneously from the femoral artery and
femoral vein. Adapted from (292) and (298) with permission of the American Physiological Society.
In the 1980s, Saltin and Andersen developed the one leg knee have shown a higher maximal perfusion capacity in well
extensor model that allowed for the determination of blood trained than in untrained individuals (36, 353). One of the
flow to a limited muscle mass (7). A particularly useful aspect limitations in comparing skeletal muscle blood flow during
of this model was that the active muscle mass could be defined maximal exercise in untrained versus trained individuals is
and that exercise with such a relatively small muscle mass that the work capacity and the maximal limb oxygen uptake
imposed no limit on the central capacity of healthy individ- of the trained individuals commonly is greater than that of the
uals, thus the true maximal perfusion capacity of the muscle untrained individuals (9, 233). As blood supply to the muscle
could be more correctly determined. Use of this model, com- during maximal one-leg exercise is unlikely to be limiting
bined with the thermodilution method for the determination (9, 370), the higher blood flow in the trained would be a con-
of blood flow (9), revealed maximal blood flow levels of 250 sequence of the greater work output rather than a reflection
to 300 mL 100 g min−1 (9, 217, 354) which were evidently of maximal perfusion capacity.
greater than those previously reported for skeletal muscle Nevertheless, a greater perfusion capacity in trained mus-
in humans (35, 255). Measurements of maximal perfusion cle is a likely outcome of aerobic training as evidenced by
capacity in trained individuals with use of the one leg model greater maximal blood flows in endurance trained animals
Volume 6, January 2016 9
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
(247-249,397). The advantage in animal models compared to flow is regulated is not complete. A number of mecha-
the human model is that flow capacity can be assessed more nisms and compounds have been identified and proposed
directly, by determination of maximal perfusion achieved to play a role but exactly how the systems are integrated
through increases in perfusion pressure, thus without influ- and their relative importance and roles remain somewhat
ence of a change in performance. On the other hand, the lim- unclear. Out of the mechanisms and compounds identified,
itation with this method is that it primarily determines struc- several induce their effect via sensors or receptors located on
tural adaptations and not adaptations in vasodilator capacity. the endothelium, resulting in the formation of vasodilators.
As described in more detail below, similar kinds of mea- Such endothelial-dependent mechanisms include flow (shear
surements have been performed in humans by use of brief stress)-induced vasodilatation and vasodilatation induced by
periods of ischemia alone or ischemia combined with exer- chemicals such as ATP and adenosine. Apart from endothe-
cise to reach maximal perfusion capacity (329,402,421). Data lial cells, cellular sources of vasodilator compounds dur-
from such interventions in humans (143,402,407) confirm the ing exercise include erythrocytes and skeletal muscle cells.
direct measurements in animals of greater maximal perfusion Skeletal muscle cells produce vasodilators such as NO, ATP,
in trained muscle. and adenosine (176, 177) whereas erythrocytes have been
shown to release the vasodilators ATP (105) and NO (401) in
response to oxygen desaturation of the hemoglobin molecule.
The effect of training on flow-mediated
This latter mechanism is highly attractive as it provides
vasodilatation a direct link between oxygen and vasodilatation; however,
The response in blood flow during exercise can be considered the physiological importance of this mechanism in humans
the most functionally relevant test of vascular function, as it remains unclear.
examines the combined effect of a large number of regulatory An important mechanical signal in the cardiovascular sys-
systems in an integrated response. Nevertheless, other vascu- tem is shear stress. As should be evident from other sections
lar function tests, such as reactive hyperemia, flow-mediated in this review, shear stress has a range of acute and long
dilatation (FMD) and infusion of vasodilators are useful in that term effects on the vasculature and changes in shear stress
they test mainly one vasodilating mechanism and the effect levels due to inactivity or activity markedly alters the phe-
or role of only one or a few vasodilator compounds. Such notype of endothelial cells and affects vascular function and
tests therefore allow for more specific insight into vasoregu- vascular growth, (96, 433, 459). The acute effect of increased
latory mechanisms than exercise and particularly FMD has shear stress is an increase in the formation of vasodilators
been proven useful as predictor of cardiovascular disease including NO, prostacyclin, and endothelial-derived hyper-
(142). FMD is commonly measured in the brachial artery polarizing factors (EDHF) (50), but NO may be the most
and assessed as the change in vessel diameter that occurs important component (141). The role of shear stress for exer-
after a period of forearm occlusion induced by use of a cuff cise hyperemia is unclear but it is more likely that shear stress
(57). A large number of studies have been conducted in which has a role in fine tuning rather than in regulation of the overall
the effect of training on FMD has been evaluated in different magnitude of blood flow.
populations with an emphasis not only on individuals at risk Another mechanism in the control of blood flow to the
for cardiovascular disease (142), but also in healthy young working muscle is conducted vasodilation. Conducted vasodi-
individuals (309, 409). Cardiovascular risk groups generally lation is a process in which the signal for vasodilatation trav-
experience marked improvements in FMD with exercise train- els up- and downstream, along the vascular wall, either in the
ing (426) whereas the effects are less clear in young healthy endothelium or the smooth muscle cells, via gap junctions
controls (146). As with other cardiovascular adaptations, an (20, 396). This mechanism is important for coordination of
important mechanism underlying an improved FMD response flow as it allows vasodilatation to occur in the larger upstream
with training is the exercise-induced shear stress signaling vessels that do not necessarily experience the chemical or
(433) which is a stimulator of improved endothelial function mechanical stimuli that are present in proximity of the work-
through an upregulation of vasodilators including NO (50). ing muscle fibers. It has been clearly demonstrated that con-
traction of muscle fibers induces conducted vasodilation in
animal models, supporting a functional role of this mecha-
Control of exercise hyperemia
nism in the exercising skeletal muscle (67, 305).
Exercise hyperemia is a highly complex and well regulated An additional vasodilator mechanism is the myogenic
process that involves sympathetic vasoconstriction, an inte- response, which is the response of smooth muscle cells to
gration of a large number of vasodilator systems as well changes in transmural pressure that occur with a change in
as several modes of activation of these systems (Fig. 5). blood pressure. The myogenic response is known to exist
During exercise the increased sympathetic activity causes in skeletal muscle arterioles, especially in smaller arterioles
arteriolar constriction and in the active muscle effective (85), and it has been shown that vasodilatation induced by
amounts of vasodilators have to be formed to overcome and mechanical compression, as would take place during con-
exceed this constriction to enable sufficient oxygen delivery. traction, occurs in part through a myogenic response (64).
Our understanding of precisely how skeletal muscle blood However, as such, the myogenic response may not be of great
10 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
Muscle
Conducted contraction/
vasodilation metabolism
Endothelial Functional
mediated dilation sympatholysis
Mechanically Chemically Cellular
induced induced sources
Endothelial cell Skeletal muscle cell Red blood cell
Adenosine Adenosine ATP
ATP ATP NO
NO NO
Prostanoids ROS
EDHF
Endothelin-1
ROS
Smooth muscle cell
Figure 5 Regulation of skeletal muscle blood flow during exercise. Several vasoactive mechanisms are involved
in the regulation of skeletal muscle blood flow during exercise and together these mechanisms secure a highly
precise oxygen delivery for the energy production required for the contractile work of the muscle. The vasodilator
mechanisms include endothelial dependent vasodilatation which can be induced both by mechanical influence,
primarily via shear stress, but also chemically via compounds such as ATP and adenosine. In response to the
contractile work, skeletal muscle cells can produce and release vasodilator compounds including nitric oxide
(NO) and ATP. NO and ATP can also be produced by red blood cells in response to off-loading of oxygen
from the hemoglobin molecule which occurs in the arterioles and capillaries. Coordination of blood flow in the
microvascular system is facilitated by retrograde conducted vasodilation. In conducted vasodilation an electrical
signal and a calcium wave travel in retrograde direction leading to vasodilatation in upstream arterioles. Finally,
specific compounds such as ATP may reduce the efficacy of sympathetic activity in the skeletal muscle arterioles,
thereby reducing the constrictive effect. ATP: Adenosine 5′ triphosphate, NO: nitric oxide; ROS: reactive oxygen
species; EDHF: endothelial-derived hyperpolarizing factor.
importance for control of skeletal muscle blood flow during on P2Y receptors on the endothelial cells (48). Animal experi-
exercise. ments have suggested that the vasodilatory effect of interstitial
It should be mentioned that, although most vasodilator ATP is stronger than its constrictive effect (93, 313).
mechanisms can be activated from the luminal side of the In summary, skeletal muscle blood flow during exercise
blood vessels, compounds on the interstitial side, such as is regulated by a balance between, on one hand, primarily
those formed by the skeletal muscle, are also likely to be sympathetic vasoconstriction and, on the other hand, sev-
important in blood flow control. Vasodilators present in the eral vasodilating mechanisms leading to the formation of
muscle interstitium may induce their effect by direct action endothelial-dependent and endothelial-independent vasodila-
on the smooth muscle cells or via endothelial cells, either tors. In addition, as further described below, metabolic
at the capillary level inducing conducted vasodilation, or at modulation of the effect of the sympathetic nervous activity,
the arteriolar level through endothelial cell protrusions (384). so-called functional sympatholysis, is likely to be a central
Several vasoactive compounds have been shown to increase regulatory mechanism in exercise hyperemia.
in the interstitium with exercise including adenosine, ATP,
prostacyclin, and NO (116, 176). Out of these compounds
Effect of endurance training on vasodilator
adenosine, prostacyclin, and NO can induce vasodilatation
capacity and vasoconstrictors
by direct action on the smooth muscle cells. Interstitial ATP
can induce vasoconstriction via P2X receptors on the smooth One of the most well studied vasodilator systems in skeletal
muscle cells or, alternatively, induce vasodilatation by acting muscle tissue is NO (Fig. 6). The functional role of NO for
Volume 6, January 2016 11
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
A training-induced enhancement in NO availability could
potentially be brought on by several mechanisms including
increased eNOS protein, increased eNOS activity by changes
in phosphorylation status, reduced eNOS uncoupling and
reduced removal of NO by reactive oxygen species (114).
These mechanisms are described below.
eNOS expression
A large number of human (66,117,161) and animal (251,277)
studies have shown a higher level of eNOS protein in skele-
tal muscle tissue and blood vessels after a period of exercise
training. Through detailed studies on eNOS expression in
the arteriolar bed of trained rats, McAllister and co-workers
(276) demonstrated that training-induced alterations in eNOS
differed according to fiber type and also concluded that the
Figure 6 The effect of endurance training on vasodilators and vaso- upregulation of eNOS occurred primarily in muscles in which
constrictors involved in the regulation of skeletal muscle blood flow. training had induced a flow response. This proposition fits well
Skeletal muscle blood flow regulation is brought about by a balance
between on one hand sympathetic vasoconstriction and other vaso- with the documented importance of shear stress in upregula-
constrictors such as endothelin 1 (ET-1) and thromboxane (TXA2 ) and tion of eNOS (136, 352). It should be noted that exercise
on the other hand vasodilators formed in the active muscle, of which training also has been shown to increase levels of neuronal
nitric oxide (NO) and prostacyclin (PGI2 ) appear to be central. Another
important aspect in skeletal muscle blood flow regulation is the sub- NOS (nNOS) (135, 314, 315, 408). nNOS, which is located
stantial interaction between vasodilator systems and compounds. For in large amounts within the skeletal muscle fibers, may con-
example, ATP and adenosine can mediate vasodilatation via activation tribute to vascular control, in part through its role in functional
of receptors on the endothelial cells resulting in the formation of NO and
PGI2 . NO and PGI2 in turn interact in a redundant manner so that when sympatholysis in rodents (430).
one is inhibited the other system can compensate. The effect of train-
ing on the formation of vasodilators and constrictors (marked by blue
arrows) has not been fully clarified and the attempt to illustrate changes eNOS activation
in this figure is tentative. Studies show that the concentrations of NO and
prostacyclin in plasma and the muscle interstitium are either enhanced Findings on the effect of training on the basal state of acti-
or remain unaltered at rest and during exercise. Adenosine and ATP vation of eNOS, as assessed by changes in eNOS phospho-
levels in the muscle interstitium may increase with training, however, in
parallel, the vascular sensitivity to nucleotides is reduced. On the con- rylation status or direct measurements of activity in skeletal
strictor side, ET-1 and TXA2 have been shown to be reduced in plasma muscle, have not been consistent. Some studies in humans
at rest whereas plasma noradrenaline is reduced during exercise indi- (59, 135, 315) and rodents (278, 436) have shown no effect
cating an attenuated sympathetic drive. ATP = Adenosine 5’triphos-
phate, ADO = adenosine; PGI2 = prostacyclin; NO = nitric oxide; NE of exercise training either on basal vascular eNOS phos-
= Noradrenaline, ET-1 = endothelin-1, TXA2 = thromboxane A2 . p and phorylation or activity. However, an increased eNOS activity
i in figure beside blue arrows specify that changes were observed in after training has been reported in skeletal muscle of young
plasma and muscle interstitium, respectively.
(165) and aged (408) rodents. Moreover, immunohistochem-
ical analysis of eNOS phosphorylation has shown a reduction
exercise hyperemia has been determined by use of NO block- in the basal and exercise-induced eNOS ser1177 phosphoryla-
ade during exercise. Such studies have shown that removal tion after training (66). The reason for these discrepancies in
of NO production by infusion of an NOS inhibitor does findings is not clear.
not alter leg blood flow (118, 344), whereas in the forearm,
NOS inhibition has none or a modest effect on steady-state
eNOS uncoupling
exercise hyperemia (131, 390, 398) but a more pronounced
effect on the rapid rise in blood flow at onset of exercise eNOS is a homodimeric enzyme which can be uncoupled to
(55, 56). Several studies have, moreover, found a lowering monomers due to factors such as increased oxidative stress and
of blood flow with combined inhibition of NOS with either reduced availability of the cofactor tetrahydrobiopterin (BH4)
inhibition of cyclooxygenase (41, 173, 291) or inhibition of (114). Instead of forming NO, the eNOS monomer produces
cytochrome P450 2C9, an enzyme producing the endothe- the reactive oxygen species, superoxide, thereby resulting in
lial derived hyperpolarizing factor 11, 12, eicosatrienoic acid not only a reduced formation of NO but also an increased for-
(184). Based on existing data, it has been theorized that NO is mation of superoxide anions that can react with and remove
important for exercise hyperemia, but not obligatory as other NO (113). A direct assessment of eNOS uncoupling by West-
systems may compensate for NO when the formation of NO ern blot analysis in humans before and after a training period
is impaired. For a more complete description of the interac- has been conducted in skeletal muscle samples of normoten-
tion and redundancy of vasodilators, the reader is referred to sive and hypertensive individuals (315). The study showed
reviews specifically addressing this topic (177). that the content of eNOS monomers to total eNOS in skeletal
12 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
muscle tissue was lower after training in both groups of sub- been shown to be more markedly improved in exercise trained
jects, reflecting a reduced degree of uncoupling. In addition, than in sedentary muscle (125,181,301). Nyberg et al. showed
indirect evidence for eNOS uncoupling has been reported in that combined NOS and COX inhibition reduced exercise
rodents (399). The authors demonstrated that the availability hyperemia more after 8 weeks of spinning training in nor-
of BH4 was restored in aged rodents with exercise training motensive individuals suggesting that the role of NO and
concomitant with an improved flow stimulated NO availabil- prostanoids was lower after training (315). Accordingly, the
ity in soleus arterioles (399). Functionally, eNOS uncoupling hyperemic response to passive movement of the lower leg,
could have a relatively large impact on NO availability and which is induced by shear stress and almost fully NO depen-
further studies on the effect of training on eNOS uncoupling dent (287), appears to be lower in young trained compared
are clearly warranted. to untrained individuals (Nyberg, Bangsbo, Hellsten, unpub-
lished observation) whereas in aged training was shown not
to alter the magnitude of hyperemia during passive move-
Removal of NO by ROS
ment (135).
Exercise training may enhance NO bioavailability by reduc- Based on existing data on the effect of training on eNOS
ing the presence of ROS and thus lowering scavenging of and NO availability and function, it may be concluded that
NO by ROS, at least in the elderly. In elderly individuals, endurance training can lead to an improvement in the avail-
the bioavailability of NO is seemingly lower than in young, ability of NO in skeletal muscle, in part by increased forma-
an effect that, at least in part, may be related to an increased tion of NO and in part by reduced removal of NO via ROS.
presence of ROS (79, 121, 231, 417). Comparisons between Evidence point at that increased formation of NO may be the
physically active and sedentary aged and young have shown result of increased eNOS expression and increased eNOS acti-
that NO availability, as assessed by an improved response to a vation via shear stress or chemical (e.g., ATP or adenosine)
vasodilator stimulus after infusion of the antioxidant ascorbic influence. The functional consequence of improved NO avail-
acid, was improved in sedentary aged individuals with little ability may be more evident in the forearm than the leg vas-
effect seen in young and trained elderly (121, 417). In a study culature but also most prominent in individuals with impaired
determining NO metabolites in plasma and muscle intersti- vascular function.
tial fluid in sedentary and lifelong trained aged individuals,
infusion of the antioxidant n-acetylcysteine (NAC) revealed
a greater elevation in NO metabolite concentrations in the
Prostaglandins
untrained than in the trained individuals (314). These find-
ings suggest that exercise training reduces the removal of NO Vasoactive prostaglandins include the vasodilators prostacy-
by ROS, potentially by improving the endogenous antioxidant clin and prostaglandin E2 and the vasoconstrictor thrombox-
defense (336). Interestingly, in contrast to the findings in the ane A2. There has been much less focus in the literature on
forearm (79, 231, 417), the improved NO availability in the the role of prostaglandins than on NO for control of exer-
aged sedentary group with NAC infusion was not paralleled cise hyperemia, however, prostacyclin is a mediator of both
by improved exercise hyperemia in the leg, suggesting that mechanical and chemical signals in the vasculature including
the increased presence of NO had little functional influence shear stress (199) and ATP and adenosine induced vasodi-
(314). In the discussion on the removal of NO by ROS it latation in the leg (290, 294) with a limited effect evident
should, nevertheless, be emphasized that an appropriate bal- in the forearm (78, 362). As described above, prostacyclin
ance between NO and ROS appears essential for adaptation has been proposed to interact closely with NO in a manner
to training and function in the vascular system as evidenced where prostacyclin can compensate for a lack of NO and vice
by training-induced enhancements in NADPH oxidase (135) versa (40, 291). Studies have shown that a period of exer-
and evidence for the importance of ROS in vascular function cise training increases the protein concentration of prostacy-
(135, 399, 400). clin synthase and COX-1 in skeletal muscle tissue (135, 175)
Overall, evidence suggests that endurance training can although this has not been observed in all studies (161). In
improve NO availability by reducing NO removal by ROS, animal studies, training-induced improvements in endothelial
presumably via improved antioxidant defense or reduced ROS dependent vasodilatation via bradykinine and acetylcholine
formation, although this may primarily be evident in aged are partly dependent on prostaglandins (86, 87). Moreover,
individuals or individuals with compromised vascular func- in individuals with essential hypertension, training enhances
tion (121, 316). the increase in muscle interstitial prostacyclin in response to
adenosine infusion (175) and improves the balance between
basal prostacyclin and thromboxane levels in the muscle inter-
Functional role of NO in trained versus stitium (161). Therefore, although relatively limited data is
untrained individuals
available on the effect of training on the prostaglandin system,
A few studies have assessed the functional role of NO in evidence point in the direction of that this system contributes
trained versus untrained subjects through studies of NO block- importantly to the training-induced improvement in vascular
ade. The vasodilator response to ACh and bradykinine has adaptations.
Volume 6, January 2016 13
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
Nucleotides vasodilators, most likely via purinergic receptors on the
ATP endothelium (313). Somewhat unexpectedly, endurance train-
ing leads to a reduced sensitivity to arterially infused ATP
ATP has been proposed to hold several roles in muscle blood (293), whereas immobilization of the leg leads to an increased
flow regulation. ATP in plasma binds to P2Y purinergic recep- sensitivity to infused ATP (292). This may seem counterintu-
tors on the endothelium (74), most likely P2Y2 receptors, itive; however, it may suggest that the relative importance of
leading to formation of NO, prostaglandins, and possibly the different vasoactive compounds can change with training
other unidentified vasodilators (330). ATP can also induce status.
a propagated response, initiated from the smallest microves-
sels and capillaries, leading to upstream vasodilatation (105).
In addition, ATP has a sympatholytic effect (365) and may
Adenosine
induce vasodilatation through hyperpolarization of the vascu- Adenosine is a degradation product of ATP that binds to
lar cells (77). The functional role of ATP has been proposed to P1 purinergic receptors whereby NO and prostaglandins are
be related to distribution of microcirculatory flow more than formed (348,406). In humans, the concentration of adenosine
to the magnitude of flow to the muscle (412). in plasma does not increase during exercise, which probably
ATP increases both in plasma and in the muscle intersti- is related to a very brief half-life of this purine. In the muscle
tial fluid during acute exercise (176, 297). In the circulation, interstitium, the adenosine concentration does increase with
ATP may originate from erythrocytes, endothelial cells or exercise, to some extent in relation to exercise intensity (176).
platelets, although erythrocytes appear to be a primary source Nonspecific inhibition of adenosine receptors lowers blood
(412). It has been well documented that erythrocytes release flow to exercising muscle by about 15% to 20% (294,343) pro-
ATP in response to a reduction in oxygen saturation of the viding evidence for a functional role of adenosine in exercise
hemoglobin molecule, a mechanism that occurs primarily in hyperemia, although there are individual differences as evi-
the smallest arterioles and the capillaries (411). There is also denced by a negligible effect of adenosine receptor blockade
evidence for that compression of erythrocytes causes release on exercise hyperemia in a fraction of the population (272).
of ATP (105). It should be noted that in patients with cys- Limited data exist on training and the adenosine sys-
tic fibrosis, erythrocytes lack the capacity to release ATP, yet tem. In hypertensive individuals, training has been shown
exercise hyperemia is similar in magnitude to that of controls to result in an increased exercise-induced muscle intersti-
(391). This observation would suggest that ATP originating tial adenosine concentration whereas no effect was observed
from erythrocytes is not obligatory for bulk flow to the muscle; in a matched group of normotensive individuals (175). The
however, it does not exclude a role in flow distribution. vasodilator response to adenosine after a period of training
In the muscle interstitium, ATP is thought to originate has been reported to be lowered in the human leg (175) and
primarily from the contracting skeletal muscle although the either unaffected (241) or enhanced (87) in animals. Further
underlying mechanism is not completely clarified. In vitro studies are needed to clarify these divergent findings.
studies have provided evidence for that ATP may be released An overall conclusion from existing data is that training
from skeletal muscle cells via pannexin-1 hemi channels (51) can increase the exercise induced ATP and adenosine forma-
and the cystic fibrosis transmembrane conductance regula- tion and reduce the sensitivity to ATP and adenosine. It is
tor (438). Measurements of ATP in the muscle interstitium clear that nucleotides are important for the control of skeletal
have revealed inconsistent findings. In aged men, ATP levels muscle blood flow, however, the effect of exercise training on
have been reported to be higher in life-long trained compared the functional role of ATP and adenosine remains uncertain.
to sedentary men (295) whereas in hypertensive individuals
reduced interstitial ATP levels were observed after training
EDHF
(161). Moreover, in young healthy men, a period of immo-
bilization by casting of one leg was shown to reduce the The concept of EDHF was originally derived from the finding
exercise-induced increase in inerstitial ATP levels (292). So that a fraction of the vasodilatory response to a vasodilator
far, no studies have addressed the effect of exercise training such as ACh, is still present when NO and prostaglandin for-
on the specific mechanisms of ATP release from erythrocytes mation is blocked (49). The remaining vasodilatation related
in vitro. to hyperpolarization is defined as EDHF (49, 111). EDHF
In the muscle interstitium, ATP may actually induce vaso- has been identified as multiple compounds, where the iden-
constriction by direct action on purinergic P2X1 receptors tity differs between tissues and vessel size. In skeletal mus-
located on the smooth muscle cells (48). It has, however, cle, hydrogen peroxide and eicosatrienoic acids (38,108,256)
been shown in laboratory animals that superfusion of skele- have been identified as EDHFs. No human studies have doc-
tal muscle with ATP, which would correspond to increased umented an effect of endurance training on the role of EDHF
ATP in the interstitium, induces vasodilatation (93,313). Inhi- for vascular function, however, in rodents, EDHF has been
bition of NO and prostaglandin formation abolishes ATP- implicated in training-induced improvements in endothelial-
induced vasodilatation in this model suggesting that the effect dependent dilation in cardiac (148, 285) and skeletal muscle
of interstitial ATP is mediated by the formation of these (149).
14 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
Endothelin-1, thromboxane, and angiotensin II the effect of training on vascular function in humans and
laboratory animals have reported a lack of effect on smooth
Endothelin-1 is a circulating vasconstrictor thought to be of muscle cell sensitivity to NO (88, 120, 436) although excep-
importance in particular in pulmonary hypertension, kidney, tions exist (242). It is nevertheless unlikely that improved NO
and metabolic syndrome (383). Individuals with metabolic sensitivity is a primary mechanism behind training-induced
syndrome commonly have elevated levels of endothelin and improvements in vascular function. Other compounds such
there are also indications that endothelin bears a relation- as adenosine and prostacyclin can also induce vasodilatation
ship to age (317). In healthy young and old individuals, through direct action on the smooth muscle cells, however, as
endothelin receptor A/B blockade or specific receptor A adenosine also acts via endothelial cells (318) and prostacy-
blockade has been shown to increase exercise hyperemia clin shows a strong interaction with NO (311) the interpreta-
with a greater effect observed in aged (23, 428). Moreover, in tion of their direct effect on smooth muscle is difficult.
spontaneously hypertensive rats, treatment with a blocker of In animal models, exercise training has also been shown to
endothelin receptor A has been shown to increase flow depen- affect aspects such as calcium control (442) and the expression
dent dilatation (203). Endurance training has a pronounced and activity of potassium channels in vascular smooth muscle
effect on levels of endothelin-1 in plasma and endurance cells (261, 464), but to date little evidence exists in humans.
training has been found to reduce endothelin-1 levels by up
to 30% (25, 270, 317, 319). Maeda and collaborators (269)
found that endothelin A and B receptor inhibition improved
carotid artery compliance in sedentary middle-aged and older Effect of Exercise Training on
subjects and that this effect was abolished after regular physi-
cal activity in parallel with a lowering of plasma endothelin-1 Functional Sympatholysis
levels. In animal studies, the effect of training on the func- During exercise, sympathetic nervous activity increases
tional role of endothelin-1 is less consistent (91, 250). It is (5, 394) in both resting and contracting skeletal muscle
not known whether the improved vascular function com- (163, 347, 414). In inactive tissues, the increase in sympa-
monly observed with training is related to the reduction in thetic drive causes vasoconstriction (32, 368). However, in
plasma endohelin-1 levels; however, it is likely a contributing young healthy individuals the vasoconstrictor effect of an
factor (428). increase in sympathetic nervous activity, induced by lower
Thromboxane A2 is a vasoconstrictor formed in the body negative pressure (162, 447), or by an increase in nore-
arachidonic acid pathway, a pathway that also produces pinephrine release from sympathetic nervous endings induced
other prostanoids including the vasodilator prostacyclin. An by tyramine infusion (292, 295, 314, 364, 437), can be attenu-
impaired balance between vasodilating and vasoconstricting ated or even abolished in skeletal muscle during contraction.
prostanoids is thought to be a contributing factor in the devel- This phenomenon, termed functional sympatholysis (351), is
opment of vascular dysfunction in cardiovascular disease thought to allow adequate perfusion and oxygen delivery to
(444). Limited evidence exist for the effect of exercise training the contracting fibers (379). In accordance, inhibition of α-
on the balance of vasodilating and constricting prostanoids in adrenergic tone has been shown to disturb the distribution of
humans but there are indications in the literature that exercise blood flow and oxygen extraction in contracting skeletal mus-
training may improve the prostanoid balance toward more cle by increasing blood flow around especially inactive muscle
vasodilators (161, 413). fibers (174). The mechanisms underlying functional sympa-
Angiotensin II is also a vasoconstrictor that is considered tholysis is thought to involve locally released substances that
a central factor in vascular dysfunction (376) and, in individ- modulate the postreceptor effect of norepinephrine binding to
uals with cardiovascular disease, exercise training lowers the α-receptors on the smooth muscle cells (379).
angiotensin levels in plasma (468). Although the first report of a contraction-induced
Combined, existing data suggest that exercise training can attenuation of sympathetic nervous activity was presented in
reduce vasoconstrictor levels, which may be a contributing 1937 (349), only a few studies have looked at the effect of
factor to the reduced peripheral resistance and the lowering exercise training on functional sympatholysis. Remensnyder
of blood pressure in cardiovascular disease states. and co-workers (351) demonstrated in 1962 in dogs that the
responsiveness of a vascular bed to adrenergic stimulation at
rest diminishes significantly with a small increase in oxygen
Exercise training and smooth muscle cell function
uptake. It was more recently shown in humans that following
Smooth muscle cell sensitivity is in vivo assessed as vasodi- an exercise bout, a blunting of sympathetic vasoconstriction
lation in response to a compound that can relax the smooth was evident in the skeletal muscle previously engaged
muscle cell without the presence of the endothelium. This in exercise (299). This residual effect of acute exercise
is often referred to as endothelial independent vasodilata- indicates that exercise training is central for stimulating
tion. Experimentally, smooth muscle cell sensitivity is often the signaling pathways that are important for functional
determined by use of an NO donor (e.g., sodium nitroprus- sympatholysis. In accordance, data obtained from both longi-
side or nitroglycerin). Interestingly, most studies examining tudinal (209, 292, 293) and cross-sectional (295) studies have
Volume 6, January 2016 15
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
3.0 availability in older men with impaired functional sympa-
Exercise tholysis does not increase leg exercise hyperemia (295, 314).
Exercise + tyramine
Collectively, these observations indicate that NO may not
be essential for functional sympatholysis in humans and the
Blood flow (L min–1)
findings in the rat (209) may, therefore, be species specific.
As described previously, the concentration of ATP
2.5 increases in the plasma of the arterial inflow and venous
drainage of active skeletal muscle (139, 297), and when
infused, ATP can significantly blunt sympathetic α-adrenergic
vasoconstriction in young adults (230, 364). In accordance,
ATP released from erythrocytes has also been suggested to
2.0 contribute to the regulation of microvascular perfusion dis-
tribution in skeletal muscle (411). Although these findings
0.0
Immobilized Untrained Trained suggest that intravascular ATP may be an important medi-
ator of functional sympatholysis, no evidence for a causal
Figure 7 Femoral arterial blood flow during knee-extensor exercise
link between functional sympatholysis, intravascular ATP and
without and with arterial infusion of tyramine (induces a release of nore-
pinephrine from sympathetic nerve endings) with a previously immobi- training status has been provided. During muscle contractions,
lized, untrained, and trained limb. Immobilization lasted for two weeks the concentration of ATP increases in the extracellular space
and was achieved by casting. Blood flow was determined by ultrasound in proportion to the intensity of contraction (176, 260) and
Doppler methodology, arterio venous oxygen extraction was obtained
by measurements of oxygen content in blood drawn simultaneously from interstitial ATP has been shown to induce vasodilatation in
the femoral artery and femoral vein. Adapted from (292) and (295) skeletal muscle (313). The concentration of skeletal muscle
with permission. interstitial ATP during exercise is reduced with immobiliza-
tion (296) and increased in lifelong physically active men
provided strong evidence for that the ability for functional (295). In agreement with these observations, a close coupling
sympatholysis is related to the training status of the skeletal also exist between the concentration of interstitial ATP and
muscle (Fig. 7). the degree of functional sympatholysis (312). Taken together,
The mechanisms underlying the effect of training on func- the level of interstitial ATP may be important for the degree
tional sympatholysis are still unresolved, but data obtained of functional sympatholysis and one mechanism underlying
from the human leg indicates that a reduced α-adrenergic the beneficial effect of exercise training on the modulation of
responsiveness may be important (293), whereas rodent data sympathetic nervous activity could potentially be an increase
suggest that functional sympatholysis is augmented through a in the concentration of skeletal muscle interstitial ATP.
NO-dependent mechanism in an intensity-dependent manner Oxidative stress has been suggested to impair functional
(209). In regard to the latter study, a more pronounced vaso- sympatholysis in skeletal muscle of rat hindlimb and human
constrictor effect of sympathetic stimulation was observed forearm (107). Since reactive oxygen species (ROS) scavenge
in trained rats at rest. Since sympathetic stimulation elicited NO and thereby decreases the bioavailability of this vasoac-
the same vasoconstrictor response in the control and trained tive substance (106,418), such an effect of oxidative stress on
animal during contractions, the augmented functional sym- functional sympatholysis is in congruence with the reported
patholysis was a direct effect of the increased sympathetic role of NO for functional sympatholysis in the rat (431) and
responsiveness detected at rest (209). Importantly, blood flow human forearm (59,382). Exercise training effectively upreg-
and oxygen delivery is of paramount importance for skeletal ulates antioxidant systems in both blood and skeletal muscle
muscle performance, and the observation that similar sympa- (133, 135, 137, 314, 316), allowing for a greater removal of
thetic stimulation elicited a comparable constrictor response ROS which may contribute to the improved functional sympa-
during contractions in the trained and untrained animals indi- tholysis in trained skeletal muscle. Evidently, more evidence
cates that the augmented functional sympatholysis may have is needed to substantiate such an effect of training on ROS
served to counteract the increased sympathetic responsive- handling and functional sympatholysis.
ness. Conversely, human data have provided evidence for To summarize, contracting skeletal muscle effectively
that the vasoconstrictor response to a similar release of nore- counteracts the vasoconstrictor effect of an increase in sym-
pinephrine from sympathetic nerve endings with infusion of pathetic nervous activity. The mechanisms underlying this
tyramine during contractions is attenuated with exercise train- functional sympatholysis may involve locally released sub-
ing (293, 295). Furthermore, NO has been shown to mediate stances such as ATP and NO that modulate the postrecep-
functional sympatholysis in rat skeletal muscle (431) and NO tor effect of norepinephrine binding to α-receptors on the
has been suggested to play an important role in modulat- smooth muscle cells. It should, however, be noted that species
ing sympathetic vasoconstriction in the microcirculation of and limb differences are likely to exist. The ability for func-
human contracting forearm muscle (59, 382). However, infu- tional sympatholysis is to a large extent related to the training
sion of a NO donor does not blunt sympathetic vasoconstric- status of the contracting skeletal muscle. This close associ-
tion in the forearm of young men (363) and increasing NO ation between training status and the degree of functional
16 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
sympatholysis could be an effect of a training-induced reduc- 3.5
Untrained/moderately trained
tion in α-adrenergic responsiveness and/or changes in the ATP, Well-trained
NO and antioxidant systems. 3.0
2.5
Capillary-to-fibre ratio
Capillary Growth in Skeletal Muscle in 2.0
Response to Training
1.5
The level of capillarization in skeletal muscle is highly impor-
tant for the functional capacity of the muscle, in particular 1.0
for endurance performance but also for performance during
shorter term exercise at high intensities. An increase in car- 0.5
diac output observed with endurance training, allows for an
0.0
enhanced perfusion capacity of the muscle during whole body 0 weeks 4 weeks 7 weeks Cross-sectional
exercise at high to maximal aerobic intensities. Without a par-
allel enlargement of the microvascular network, the conse- Figure 8 Capillary-to-fiber ratio in untrained (VO2max : ∼50 mL O2
min−1 kg−1 ) young men before (0 weeks) and after 7 weeks of exer-
quent increase in velocity of the red blood cells would reduce cise training (7 weeks) and in trained (VO2max : ∼66 mL O2 min−1
the time for gas exchange at the capillary site and lead to less kg−1 ) young men (cross-sectional). The 7-week training period consisted
optimal conditions for oxygen supply and thus uptake in the of high-intensity interval training. Capillary number was obtained by
counting of immunohistochemically stained transverse muscle sections
muscle tissue. Under these conditions, the improved cardiac cut from frozen muscle (m.v. lateralis) samples. Fitness level was deter-
output would not necessarily be fully utilized. An increased mined by measurements of expired air during a graded cycle test to
capillary volume is therefore an advantageous adaptation to exhaustion. Adapted from (210) and (201) with permission.
training, securing sufficient time for off-loading of oxygen
in the muscle. Importantly, the increased capillary density
will also improve the diffusion area and diffusion distance for probably reflects factors such as the activity level of the sub-
gasses, nutrients and metabolic waste products. jects prior to training, the efficacy of the training program
The importance of capillary density in skeletal muscle is and training compliance. The efficacy of the training may be
supported by the plasticity of the capillary network where related to the intensity and duration of training although the
only a few days of muscle activity in rodents and less than importance of training intensity versus volume for capillar-
4 weeks in humans can induce increases in capillary den- ization in humans remains to be fully clarified.
sity (83, 164, 210). It should be pointed out that, although Studies on the time course of capillary growth in response
an increased capillary density is a critical adaptation to exer- to training in humans suggest that the rate of capillary growth
cise training, the specific distribution of capillaries within the is the greatest in the first weeks of training and then lev-
muscle is also an important factor for optimal oxygen supply els off after approximately four weeks (192, 210). Although
to the muscle (97). capillarization clearly will increase with training beyond the
first weeks, it seems that the difference in capillarization
in untrained versus well-trained endurance athletes rarely
Effect of endurance training on capillary growth
exceeds 2-fold to 2.5-fold (Fig. 8). In sedentary individuals,
Endurance training is likely to be the most potent physiologi- values for capillary per fiber and capillary density generally
cal stimulus of capillary growth in skeletal muscle. In humans, lie in the range of 1.5-2.5 and 300-400 caps/mm2 , respec-
a number of studies on the effect of training on skeletal mus- tively, whereas in endurance trained athletes, capillary per
cle characteristics were originally conducted almost half a fiber ratio and the capillary density lie between 2-3.5 and
century ago, when the skeletal muscle biopsy technique of 400-600 caps/mm2 , respectively (205, 340, 434, 469).
Bergstrom was introduced to the field of exercise physiol- In accordance with the concept of symmorphosis (451),
ogy (30, 223). One of the first studies examining the effect of endurance training potently increases capillarization in paral-
endurance training on capillarization in human muscle with lel with improvements in the oxidative potential of the mus-
this technique was conducted by Andersen and Henriksson in cle through enhanced mitochondrial capacity. Accordingly,
1977 (8). They showed that eight weeks of moderate intensity some of the regulatory pathways of mitochondrial biogene-
cycle training in sedentary healthy young males, lead to an sis, including AMPK and peroxisome proliferator-activated
approximate 40% increase in capillary density in the thigh receptor gamma coactivator 1α activation, are also involved
muscle (8). In general, the literature shows that, when previ- in the regulation of capillary growth (12, 253, 254). In com-
ously sedentary, healthy individuals are subjected to periods paring mitochondrial volume density with capillary length
of 4 to 8 weeks of endurance training of moderate intensities density in oxidative muscle and cardiac muscle of differ-
at between 60% and 80% of VO2max , an increase in capillar- ent animal species, a clear relationship between these two
ization of between 10% and 40% is observed (190, 206, 232) variables has been observed (Hoppeler and Kayar 1980). In
(Fig. 8). The difference in magnitude of capillary growth human skeletal muscle, the relationship between oxidative
Volume 6, January 2016 17
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
5 leading to exhaustion within 1 to 4 min (202). For exercise
20-40 years
41-60 years
performed around peak aerobic power, the physiological rele-
61-80 years vance of a high capillary density would lie in optimal oxygen
4
diffusion conditions at very high blood flows to accommo-
Capillary-to-fibre ratio
date the large aerobic energy demand. However, in interval
3 sprint exercise, with energy supply originating mainly from
anaerobic energy production, an increased capillarization may
allow for faster oxygen dependent metabolic recovery pro-
2
cesses and serve to improve the removal of metabolic waste
products such as lactate. The latter physiological function is
r 2 = 0,31 supported by a study showing that selective chronic electrical
1
P < 0.001
stimulation of glycolytic fast twitch fibers led to an increase
in capillarization (98).
0
10 20 30 40 50 60 70 80
VO2max (mL O2 min–1 kg–1) Resistance training
Figure 9 Capillary-to-fiber ratio in relation to maximal oxygen uptake As with exercise of very high intensity, resistance exercise
in young, middle-aged, and older men of different training status. Capil- requires mainly energy from anaerobic energy sources in the
lary number and muscle fibers were obtained by counting of immunohis- muscle thus capillarization may primarily be important for
tochemically stained transverse muscle sections cut from frozen muscle
(m.v. lateralis) samples. Maximal oxygen uptake was determined by
removal of metabolic waste products. From existing data, it
measurements of expired air during a graded cycle test to exhaustion. seems likely that capillary growth in response to resistance
Data adapted, with permission, from (150, 191, 201) and from Ander- training mainly occurs when there is a parallel enlargement
sen and Bangsbo (previously unpublished data) and Nyberg, Hellsten
and Mortensen (previously unpublished data).
in fiber area, ensuring that capillary density is maintained in
the muscle tissue (3). In accordance, the majority of studies
on the effect of resistance training on capillary growth show
capacity and capillary density may not be as clear but a rela- no or minor effects on capillary density (27, 65, 424, 425).
tionship between aerobic power and capillarization can be
demonstrated (197, 469). Such a relationship is illustrated Physiological signals that mediate exercise
in Figure 9 where the relationship between maximal oxygen
training-induced capillary growth
uptake and capillary per fiber ratio has been plotted for young,
middle-aged, and aged individuals of different fitness levels. A relevant question related to the efficacy of different forms of
exercise training in inducing capillary growth is which phys-
iological factors that provide signals for growth (Fig. 10).
High-intensity intermittent training
This topic was initially addressed in skeletal muscle by Olga
When evaluating the effect of high-intensity intermittent train- Hudlicka, Stuart Egginton and co-workers at the University of
ing on capillary growth, it is important to consider that high Birmingham in particular (99, 100, 465). Their work clearly
intensity intermittent training encompasses a large range of demonstrated that mechanical signals present during mus-
intensities and durations, from intervals conducted close to cle contraction, including shear stress and passive stretch,
maximal aerobic power for periods of a few minutes, to very are highly important stimulators of capillary growth. Shear
brief intervals conducted at several hundred percent of max- stress, which is elevated in the capillaries as the blood flow
imal aerobic power. High intensity intermittent training per- to the muscle increases during dynamic exercise, is sensed
formed by inactive young males at intensities between 90% by mechanotransducers in the cell membrane. The mechan-
and 170% of VO2max , has been found to induce a signifi- otransducers mediate the signal through the cytoskeleton of
cant increase in capillarization (211, 392). Moreover, in the the endothelial cells leading to increased expression of angio-
higher end of exercise intensities, Cocks et al. reported that genic proteins (10, 459). Several compounds have been pro-
repeated all-out 30 s Wingate bouts lead to an increase in posed to be of importance for the transmission of shear stress,
capillarization (66). Accordingly, in rodents, high intensity including glycocalyx, PECAM-1, VEGFR2, and VE cadherin
exercise has been shown to be similarly effective in induc- (72,441). The other mechanical stimulus that promotes angio-
ing capillarization (155, 222). Thus, based on existing data it genesis, passive stretch of the tissue, occurs repeatedly when
seems reasonable to conclude that high intensity training has a the muscle contracts. The transduction of this mechanical
similar effect on capillary growth as more moderate intensity impact to the endothelial cells is poorly understood but may
exercise in sedentary individuals. involve integrins (429) and/or fibronectin (187).
The physiological relevance of an increase in capillariza- Shear stress and passive stretch induce capillary growth
tion in the muscle in response to high intensity training is by two different processes. Shear stress induces capillary
supported by the finding of a relationship between the level growth by longitudinal splitting of the existing capillary; the
of capillarization in muscle and performance at intensities capillary endothelial cells grow inward into the lumen and
18 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
Skeletal muscle
contraction
Shear stress Passive stretch Hypoxia
MMP-2 MMP-9 VEGF HIF-1α
eNOS VEGF
VEGF
Pro angiogenic compounds Tie-2 Ang-2
Anti angiogenic compounds Ang-1
Tie-2
TSP-1
Endostatin TIMP
PF-4
Soluble VEGF receptor
Figure 10 Dynamic muscle contraction provides mechanical signals of importance for capil-
lary growth: the associated increase in blood flow to the muscle leads to an increase in shear
stress on the capillary endothelium and the contractile process induces passive stretch of the tis-
sue. This mechanical impact promotes formation of angioregulatory factors, both pro- and antian-
giogenic in nature. To what extent capillary growth occurs in the muscle is determined by the
balance between the pro and the antiangiogenic factors. One of the most central proangiogenic
factors is vascular endothelial growth factor (VEGF) which interacts closely with nitric oxide formed
from endothelial nitric oxide synthase (eNOS), whereas thrombospondin-1 (TSP-1) may be a key
antiangiogenic factor. Apart from muscle contraction, hypoxia can induce angiogenesis in part
by an increase in the transcription factor hypoxia inducible factor-1α (HIF-1α) which promotes
VEGF expression. However, the actual impact of hypoxia on human muscle capillarization is
less certain. MMP: Matrix metalloproteinase, VEGF, vascular endothelial growth factor; eNOS:
endothelial nitric oxide synthase; TSP-1 thrombospondin.1; TIMP-1: tissue inhibitor of matrix met-
alloproteinase; ANG: angiopoietin; PF-4: platelet factor 4; Tie-2: angiopoietin receptor 2.
divide the lumen of the capillary into two parallel capillaries also promote capillary growth. Extracellular fluid from con-
(100, 357, 466). Passive stretch induces capillary growth pri- tracting skeletal muscle cells in culture contain the impor-
marily by sprouting angiogenesis, where a new capillary is tant angiogenic growth factor VEGF and enhances endothe-
budded off from an existing capillary (100, 465). Sprouting lial cell proliferation (213, 461). These observations suggest
angiogenesis requires somewhat more disintegration of the that skeletal muscle cells release angiogenic compounds in
basement membrane than the process of longitudinal splitting. response to contraction. Provided that both shear stress and
Capillary growth in response to muscle contraction probably metabolism are important factors for angiogenesis, it could
occurs by both processes. be assumed that exercise of higher intensities, inducing high
In humans, evidence for a role of mechanical signals for levels of blood flow and metabolism, would provide stronger
capillary growth has been provided by use of passive move- angiogenic signals than exercise of moderate intensity. It is,
ment of the lower leg. In this model the lower leg is passively however, probably not quite that straightforward as evidenced
extended and flexed which induces stretch of the tissue and by the finding that high intensity exercise does not appear
increases flow and thereby shear stress, without an effect on to result in more capillary growth than exercise of moderate
metabolism (178). An acute bout of passive movement stimu- intensity (66,191,192,210). Moreover, a study was conducted
lates pro angiogenic factors (178) and weeks of repeated pas- in which exercise training was switched from moderate inten-
sive movement training, leads to a transient increase in prolif- sity to high-intensity interval training to examine whether
eration of endothelial associated cells and a small increase in the added shear stress and metabolic stimulus would induce
capillarization (194). These data support the notion from ani- capillarization beyond that observed with the first weeks of
mal studies that mechanical factors are important in exercise- moderate intensity exercise (192). The study revealed that no
induced angiogenesis in skeletal muscle. further angiogenesis occurred after the first 4 weeks of mod-
In addition to mechanical factors, muscle contraction per erate training despite the added stimulus (192). One explana-
se and the associated increase in muscle metabolism may tion for these observations could be that there is a limitation
Volume 6, January 2016 19
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
to how much the capillary network structurally may be altered is a substantial transient increase in VEGF mRNA levels in
within only a few weeks. Alternatively, there may not be any muscle tissue (43,126,153,355) and in VEGF protein levels in
functional benefit in enhancing the capillary network beyond the muscle interstitial fluid (127,188). The interstitial increase
that achieved in the first training period, in relation to the in VEGF during exercise is believed to mainly originate from
metabolic demands induced by the more intense training. secretion by skeletal muscle cells in response to mechanical
The final potential proangiogenic mechanism that has stimuli (213,221). The exercise-induced increase in VEGF in
been discussed with regard to exercise-induced angiogenesis the muscle interstitium is likely to be an important element
is hypoxia. In in vitro experiments, hypoxia has been shown to in capillary growth; however, regulation of capillary growth
promote endothelial cell activation, proliferation, and migra- clearly requires an orchestration of both proangiogenic and
tion (279, 281). Moreover, hypoxia leads to an upregulation anti angiogenic compounds in the muscle (95, 321). As an
of hypoxia inducible factor 1α which initiates transcription of example, data suggest that a lowering of antiangiogenic com-
the central angiogenic factor VEGF (42). However, findings pounds, such as TSP-1, actually may be essential for initiation
from animals and humans do not show a clear angiogenic of angiogenesis (321, 322).
effect of hypoxia. In fact, VEGF mRNA levels can even be A general finding in response to exercise training is that
suppressed by hypoxia (43, 323, 324). A reasonable assump- the acute exercise-induced increase in mRNA for proangio-
tion based on existing literature is that capillary density is genic factors including VEGF is reduced after a training
increased in chronic hypoxia but that this increase primarily period (191, 212, 267, 356). This reduced response seems to
reflects a decrease in muscle fiber area and less so an increase be present once capillary growth has taken place and proba-
in capillary growth (196,273). It should, nevertheless be noted bly reflects that exercise-induced angiogenic signals, such as
that animal models of local ischemia in muscle clearly show those induced by shear stress, are reduced. Interestingly, the
an effect on angiogenesis (180, 207) suggesting that more anti angiogenic compound TSP-1 has been shown to increase
severe conditions of low oxygen supply in the muscle may with training in parallel with a reduction in VEGF, further sup-
provide a stimulus for capillary growth. It is questionable porting a retardation of capillary growth as adaptation occurs
whether hypoxia is present in muscle during normoxic exer- (322). VEGF protein in skeletal muscle is, in rodents, consis-
cise. However, experimental models involving reduced blood tently found to be increased with chronic electrical stimula-
supply to the muscle in humans during exercise (154) and tion or exercise training (6, 11, 46). In humans, studies show
animal models with training in hypoxia (324) have shown a either unaltered (191,192) or increased (152,154) VEGF pro-
somewhat potentiating effect of training with reduced oxygen tein levels with training. The discrepancies between studies in
supply on the angiogenic response to exercise. humans and animals may largely be related to that earlier time
To summarize, exercise-induced signals that promote cap- points after onset of training are studied in rodents. A study
illarization in skeletal muscle include both mechanical and on the time course of expression of proangiogenic and antian-
metabolically related signals and a training-induced increase giogenic compounds in rodents by Olenich and co-workers
in capillarization is the result of an integration of such signals suggests that VEGF levels are increased within a few days
present during exercise. When training sedentary individuals, of training and then reduced after 2 to 4 weeks of training
the intensity of the exercise training does not appear to play a (320). This time course is consistent with findings in humans
major role for the magnitude of capillary growth. showing an increase in muscle VEGF protein at 10 days of
training but similar VEGF protein levels after 4 weeks of
training (152). The return in VEGF toward baseline after 4
The effect of exercise training on
weeks of training also fits well with the finding that training
angiogenic compounds
does not increase the exercise-induced secretion of VEGF to
The signals produced by mechanical and metabolic alterations the muscle interstitium in young subjects (127,191,192). This
in the muscle during exercise mediate their effects via regula- transient effect of exercise training on the angiogenic poten-
tory angiogenic compounds. These compounds which either tial underlines the open question of whether a similar rate of
promote or inhibit angiogenesis are produced in the vascular capillary growth can be achieved after the first weeks of train-
cells, the interstitial cells or in the muscle cells. The expres- ing. The obvious solution of a marked increase in training
sion of numerous angiogenic compounds have been shown intensity does not appear to provide the answer (192).
to be affected by exercise in skeletal muscle, including the In relation to the above discussion, it is worth noting that
proangiogenic compounds VEGF matrix metalloproteinases, several exercise training studies have shown increased VEGF
eNOS, and angiopoietin 2, and the antiangiogenic compounds protein levels in both muscle tissue and the muscle interstitium
thrombospondin 1, endostatin, and tissue inhibitor of matrix in individuals with reduced cardiovascular health including
metalloproteinases (264, 322, 357, 375). The most central pro individuals with heart failure (151), and essential hyperten-
angiogenic compound in skeletal muscle tissue known to date sion (160) but also in sedentary aged individuals (127, 134).
is VEGF (263,325,423,448). VEGF is stored in large amounts As stated above, training studies in humans and rodents
within the skeletal muscle fibers (159) but smaller amounts have examined a large number of proangiogenic and antian-
are also present in other cell types such as endothelial cells giogenic compounds in skeletal muscle in addition to VEGF,
(124) and pericytes (193). In response to acute exercise there although further studies are warranted to better understand
20 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
their roles and interaction. The present article does not cover shows a more uniform distribution of fiber types where the
data on the many other potentially important angiogenic com- different muscle groups consist mainly of one fiber type.
pounds, instead the reader is referred to excellent reviews that Studies on capillary growth with training in rodents show
specifically address this topic (95, 321). that capillary growth is most marked in glycolytic muscle
To summarize, existing literature suggests that capillary (17, 264).
growth is regulated by a large number of pro- and antian-
giogenic compounds that mainly are transiently altered with
acute exercise and exercise training. In accordance, although Adaptations in Inactive Skeletal Muscle
endurance training is a potent stimulator of capillary growth,
the angiogenic potential, as determined by the expression of There is evidence for that endurance training also affects
proangigenic versus antiangiogenic compounds, is not neces- the vasculature in nonactive muscle during exercise with the
sarily greater in a trained than an untrained young healthy indi- most distinct effect observed in individuals or animal mod-
vidual whereas the potential may be improved with training in els with impaired endothelial function (326). A number of
individuals with an originally reduced angiogenic potential. studies have shown that FMD is improved in the forearm con-
duit artery after a period of cycling training with the legs
(33, 144, 262, 327). One likely mechanism underlying the
The role of muscle characteristics in angiogenesis improvement in the nonactive limb is an increase in shear
The majority of data on training-induced capillary growth stress, as demonstrated in a study by Tinken et al. in which
in healthy individuals stems from determinations in the the blood flow to one of the forearms was occluded during leg
muscle vastus lateralis. The vastus lateralis muscle has a exercise training and improvements were observed only in the
mixture of Type I, Type IIa, and Type IIx fiber types and non-occluded arm (432). The increase in shear stress in the
most individuals have a similar number of Type I and Type II non-active forearm may have been due to an increase in cuta-
muscle fibers although outliers exist (259). The mix of fiber neous blood flow associated with the increase in temperature
types means that most capillaries are shared between Type I, during exercise (308).
Type IIa, and to some extent Type IIx fibers, thus the effect Endothelial function of resistance arteries may also be
of a training regimen on capillary growth in relation to fiber improved in nonactive skeletal muscle with a period of exer-
type is not so easily assessed in humans but can be detected cise training. Improved endothelial function in nonactive mus-
as illustrated in Figure 11. Cross sectional data indicate that cle has been demonstrated in animal models by assessment
endurance athletes have a higher (205) or similar (80) number of the responsiveness to an endothelial-dependent vasodilator
of capillaries around Type I versus around Type II fibers such as ACh (241, 242, 460). The mechanism underlying the
and after high intensity training an unaltered distribution of adaptations in resistance arteries of nonactive limbs remains
capillaries around Type I and Type II fibers has been observed uncertain but circulating factors and shear stress are likely
(210). In contrast to human muscle, rodent locomotor muscle contributors to the effect (326).
With regard to the possible effect of exercise training
and shear stress on changes in microvascular growth in inac-
4.0 tive muscle, an observation was made in a study on humans
in which the effect of passive movement training on the
3.5 angiogenic response in skeletal muscle was examined. The
study showed that passive movement, which induces an NO-
3.0
Capillary-to-fibre ratio
dependent increase in blood flow, and thus shear stress, with-
2.5 out a metabolic demand (178,194,287), lead to an angiogenic
response, as evidenced by upregulation of angiogenic fac-
2.0 tors, a transient increase in proliferating cells associated with
muscle capillaries and a small increment in capillarization
1.5 (194). In addition, in the nontrained leg, a small increase in
r 2 = 0.493
P < 0.001 capillarization and an increase in the mRNA level of angio-
1.0
genic factors were detected. These observations agree with
0.5
the important role of shear stress for vascular adaptations and
20 30 40 50 60 70 80 90 100 indicate that training can induce vascular adaptations also in
MHC I (%) inactive muscle.
Figure 11 Capillary-to-fiber ratio in relation to Myosin Heavy chain
1 (MHC I) positive muscle fibers in subjects of different fitness level
(25-65 mL O2 min−1 kg−1 ) and age (20-71 years). Capillary number
The effect of exercise training on adaptations in
and muscle fibers were obtained by counting of immunohistochemically other tissues
stained transverse muscle sections cut from frozen muscle (m.v. lateralis)
samples. Data adapted, with permission, from (150) and Nyberg, Hell- The effects of exercise training include also alterations in
sten and Mortensen (previously unpublished data). the vascular control in many tissues other than cardiac and
Volume 6, January 2016 21
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
skeletal muscle. The adaptations include primarily changes In the splanchic and renal region, the primary effect of
in endothelial phenotype and function but may also entail exercise training is a higher blood flow during exercise at
an increased microcirculatory network. One example is the the same absolute submaximal work rate (14, 63, 339, 369).
cutaneous circulation, which during exercise, has a primary The mechanisms underlying the training-induced increase in
function in the dissipation of heat. The cutaneous circulation is splanchic blood flow have been proposed to be a reduced
under the control of the sympathetic nervous system, both via sympathetic influence (275, 280) and improved vasodilator
cholinergic vasodilatation, involving corelease of ACh with a capacity (60, 84, 416).
second neurotransmitter, and via adrenergic vasoconstriction Combined, these examples emphasize the influence of
(226, 227). During acute exercise, the cutaneous circulation exercise training on vascular control and function in many of
is increased at the time when core temperature rises. Exer- the organs of the body to optimize aspects of importance for
cise training has been shown to lead to an increase in cuta- performance and with a close coupling to health.
neous blood flow at a lower core temperature (358) and to an
increased magnitude of skin blood flow for a given core tem-
perature (420). In accordance, cross sectional comparisons of
untrained and well-trained individuals show that skin blood
Conclusion
flow during exercise in the heat is higher in well trained than Effective endurance training can result in substantial adap-
in the untrained individuals (185). These systemic adapta- ations in the cardiovascular system ranging from improved
tions may primarily be associated with the training-induced cardiac and arterial dimensions and function and an increased
increase in plasma volume, as plasma volume is a determining number of microcirculatory vessels in skeletal and cardiac
factor for cutaneous perfusion (138, 204). The local respon- muscle (Fig. 12). Such adaptations are important for an
siveness of the skin, for example, with local heating (360) or improvement in aerobic power and performance but can
in response to ACh (238, 450), is also improved by exercise also significantly improve cardiovascular health in sedentary
training, an effect that may be due to a greater contribution individuals. A vast number of studies have characterized the
by NO and prostaglandins (92, 360), at least in part, induced functional adaptations that occur with endurance training
by repetitive increases in shear stress (308). in healthy young and aged individuals and in individuals
Other organs, in which exercise training has been with life style related disease. However, less is known
documented to induce changes in blood flow and vascular regarding the cellular and molecular mechanisms underlying
function, include the brain (4,37), and the splanchic and renal the cardiovascular changes with regular physical activity. For
circulation (60, 84, 243, 306). In the brain, the most marked example, although our understanding regarding the control
effect of exercise training probably lies in protection against of exercise hyperemia has markedly advanced over the last
cerebrovascular events and in improvement in brain function, decades, we still do not have a complete picture of which
where the latter effect is observed primarily in individuals with vasoregulatory mechanisms and compounds that are the
reduced cardiovascular health (235, 252, 452). There may be most central or how physical activity affects these systems.
multiple explanations for this phenomenon but an improved An experimental limitation in this area is the complexity of
vascular function and perfusion of the brain are likely the regulation where redundancy between compounds and
contributing factors. Ainsle et al. showed in a cross-sectional mechanisms make conclusive designs difficult. In the area of
study that middle cerebral arterial blood flow at rest is higher capillary growth in skeletal muscle substantial advancements
in individuals that conduct regular physical activity (4). Simi- have been made, in particular regarding the influence of
larly, Barnes and co-workers reported that the cerebrovascular mechanical factors such as shear stress and passive stretch
reactivity to hypercapnia was related to the aerobic fitness for the promotion of capillary growth. However, similarly
level in aged men (22). The study also reported that inhibition to the regulation of exercise hyperemia, angiogenesis is a
of prostanoid synthesis reduced the cerebrovascular reactivity highly complex process involving an orchestration of a large
to a greater extent in individuals with high aerobic power, number of pro- and antiangiogenic compounds with different
suggesting that one of the underlying mechanisms was related time courses due to their specific involvement in the several
to prostanoids (22). Moreover, the beneficial effect of training steps of the development of a new capillary. Thus, although
may in part be related to NO availability as indicated by the our knowledge regarding these processes and compounds
observation that the increase in resting cerebral perfusion and how they are affected by physical activity has improved,
after exercise training was absent in mice in which NO many aspects remain to be elucidated. Therefore, important
formation had been experimentally abolished (129). There areas that future studies should focus on are the cellular and
is also evidence for that carotid artery structure and function molecular mechanisms underlying the regulation of vascular
is improved and that atherosclerotic plaque is reduced with tone and micro- as well as macrovascular growth in skeletal
exercise training (218, 342). Although the mechanisms of muscle. Furthermore, effort should be made to improve our
improved cerebral vascular function remain unclear, as in understanding of the signals and molecular pathways under-
other tissues, shear stress may be an important contributing lying the training adaptations in cardiac tissue and cardiac
factor. microvessels.
22 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
(A) 50
LV end-diastolic volume References
Maximal cardiac output
Blood volume
1. Aalkjaer C, Heagerty AM, Petersen KK, Swales JD, Mulvany MJ. Evi-
Change with exercise training (%)
Maximum oxygen uptake
40 dence for increased media thickness, increased neuronal amine uptake,
and depressed excitation–contraction coupling in isolated resistance
vessels from essential hypertensives. Circ Res 61: 181-186, 1987.
2. Abergel E, Chatellier G, Hagege AA, Oblak A, Linhart A, Ducardonnet
30 A, Menard J. Serial left ventricular adaptations in world-class profes-
sional cyclists: Implications for disease screening and follow-up. J Am
Coll Cardiol 44: 144-149, 2004.
20 3. Ahmed SK, Egginton S, Jakeman PM, Mannion AF, Ross HF. Is human
skeletal muscle capillary supply modelled according to fibre size or fibre
type? Exp Physiol 82: 231-234, 1997.
4. Ainslie PN, Cotter JD, George KP, Lucas S, Murrell C, Shave R,
10 Thomas KN, Williams MJ, Atkinson G. Elevation in cerebral blood
flow velocity with aerobic fitness throughout healthy human ageing.
J Physiol 586: 4005-4010, 2008.
5. Alam M, Smirk FH. Observations in man upon a blood pressure rais-
0 ing reflex arising from the voluntary muscles. J Physiol 89: 372-383,
(B) 80 1937.
Capillary-to-fibre ratio 6. Amaral SL, Papanek PE, Greene AS. Angiotensin II and VEGF are
Maximal skeletal muscle blood flow involved in angiogenesis induced by short-term exercise training. Am J
Flow-mediated dilation Physiol Heart Circ Physiol 281: H1163-H1169, 2001.
60
Change with exercise training (%)
Arterial wall thickness 7. Andersen P, Adams RP, Sjogaard G, Thorboe A, Saltin B. Dynamic
Arterial diameter knee extension as model for study of isolated exercising muscle in
humans. J Appl Physiol (1985) 59: 1647-1653, 1985.
40 8. Andersen P, Henriksson J. Capillary supply of the quadriceps femoris
muscle of man: Adaptive response to exercise. J Physiol 270: 677-690,
1977.
20 9. Andersen P, Saltin B. Maximal perfusion of skeletal muscle in man.
J Physiol 366: 233-249, 1985.
10. Ando J, Yamamoto K. Effects of shear stress and stretch on endothelial
0 function. Antioxid Redox Signal 15: 1389-1403, 2011.
11. Annex BH, Torgan CE, Lin P, Taylor DA, Thompson MA, Peters KG,
Kraus WE. Induction and maintenance of increased VEGF protein by
–20 chronic motor nerve stimulation in skeletal muscle. Am J Physiol 274:
H860-H867, 1998.
12. Arany Z, Foo SY, Ma Y, Ruas JL, Bommi-Reddy A, Girnun G, Cooper
–40 M, Laznik D, Chinsomboon J, Rangwala SM, Baek KH, Rosenzweig
0 6 12 Well-trained A, Spiegelman BM. HIF-independent regulation of VEGF and angio-
Duration of training (months) genesis by the transcriptional coactivator PGC-1alpha 11. Nature 451:
1008-1012, 2008.
13. Arbab-Zadeh A, Perhonen M, Howden E, Peshock RM, Zhang R,
Figure 12 Time course of relative cardiovascular changes in Adams-Huet B, Haykowsky MJ, Levine BD. Cardiac remodeling in
response to endurance training. The relative changes in cardiovascular response to 1 year of intensive endurance training. Circulation 130:
parameters in relation to duration of regular exercise training are esti- 2152-2161, 2014.
mated based on data from the literature on humans. The included data 14. Armstrong RB, Laughlin MH. Exercise blood flow patterns within and
stem form healthy individuals and the training regimens used in the dif- among rat muscles after training. Am J Physiol 246: H59-H68, 1984.
ferent studies range from moderate to high intensity aerobic exercise 15. Astrand PO, Cuddy TE, Saltin B, Stenberg J. Cardiac output during
submaximal and maximal work. J Appl Physiol 19: 268-274, 1964.
conducted for >30 min, 2 to 4 times per week. The data on well-trained 16. Bada AA, Svendsen JH, Secher NH, Saltin B, Mortensen SP. Peripheral
stem from individuals who have participated in endurance training for vasodilatation determines cardiac output in exercising humans: Insight
several years but that are not competing athletes. Note that for some of from atrial pacing. J Physiol 590: 2051-2060, 2012.
the parameters data only exist for a training duration of two months and 17. Badr I, Brown MD, Egginton S, Hudlicka O, Milkiewicz M, Verhaeg
the amount of data available for 6- and 12-month durations of training J. Differences in local environment determine the site of physiological
is limited for all other variables. For all cardiovascular variables, it is angiogenesis in rat skeletal muscle. Exp Physiol 88: 565-568, 2003.
clear that the largest change occurs at the onset of a training program, 18. Baggish AL, Wood MJ. Athlete’s heart and cardiovascular care of
an effect that likely reflects that the signals for adaptation, for example, the athlete: Scientific and clinical update. Circulation 123: 2723-2735,
2011.
shear stress-induced signaling, are the greatest at the onset of exercise 19. Baggish AL, Yared K, Weiner RB, Wang F, Demes R, Picard MH,
training but then level off as adaptations occur. Figure A represents Hagerman F, Wood MJ. Differences in cardiac parameters among elite
the time course of relative changes in Left ventricular (LV) end diastolic rowers and subelite rowers. Med Sci Sports Exerc 42: 1215-1220, 2010.
volume, maximal cardiac output, blood volume, and maximum oxygen 20. Bagher P, Segal SS. Regulation of blood flow in the microcirculation:
uptake. Figure B represents the time course of relative changes in capil- Role of conducted vasodilation. Acta Physiol (Oxf) 202: 271-284, 2011.
lary to muscle fiber ratio, maximal skeletal muscle blood flow measured 21. Bakker EN, van der Meulen ET, van den Berg BM, Everts V, Spaan
in the leg, FMD, arterial wall thickness, and arterial diameter of conduit JA, VanBavel E. Inward remodeling follows chronic vasoconstriction
arteries. in isolated resistance arteries. J Vasc Res 39: 12-20, 2002.
22. Barnes JN, Taylor JL, Kluck BN, Johnson CP, Joyner MJ. Cerebrovas-
cular reactivity is associated with maximal aerobic capacity in healthy
older adults. J Appl Physiol (1985) 114: 1383-1387, 2013.
23. Barrett-O’Keefe Z, Ives SJ, Trinity JD, Morgan G, Rossman MJ, Donato
AJ, Runnels S, Morgan DE, Gmelch BS, Bledsoe AD, Richardson RS,
Wray DW. Taming the “sleeping giant”: the role of endothelin-1 in
Acknowledgements the regulation of skeletal muscle blood flow and arterial blood pressure
during exercise. Am J Physiol Heart Circ Physiol 304: H162-H169,
2013.
The research of the authors has been funded by The Dan- 24. Baum O, Da Silva-Azevedo L, Willerding G, Wockel A, Planitzer
ish Council on Independent Research-Medical Sciences, The G, Gossrau R, Pries AR, Zakrzewicz A. Endothelial NOS is main
mediator for shear stress-dependent angiogenesis in skeletal muscle
Danish Ministry of Culture, The Lundbeck Foundation and after prazosin administration. Am J Physiol Heart Circ Physiol 287:
The Novo Nordisk Foundation. H2300-H2308, 2004.
Volume 6, January 2016 23
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
25. Beck DT, Casey DP, Martin JS, Emerson BD, Braith RW. Exercise 52. Calbet JA, Jensen-Urstad M, van HG, Holmberg HC, Rosdahl H, Saltin
training improves endothelial function in young prehypertensives. Exp B. Maximal muscular vascular conductances during whole body upright
Biol Med (Maywood) 238: 433-441, 2013. exercise in humans. J Physiol 558: 319-331, 2004.
26. Beere PA, Russell SD, Morey MC, Kitzman DW, Higginbotham MB. 53. Cameron JD, Dart AM. Exercise training increases total systemic arte-
Aerobic exercise training can reverse age-related peripheral circu- rial compliance in humans. Am J Physiol 266: H693-H701, 1994.
latory changes in healthy older men. Circulation 100: 1085-1094, 54. Carrick-Ranson G, Hastings JL, Bhella PS, Fujimoto N, Shibata S,
1999. Palmer MD, Boyd K, Livingston S, Dijk E, Levine BD. The effect
27. Bell DG, Jacobs I. Muscle fibre area, fibre type & capillarization in of lifelong exercise dose on cardiovascular function during exercise.
male and female body builders. Can J Sport Sci 15: 115-119, 1990. J Appl Physiol (1985) 116: 736-745, 2014.
28. Bergman BC, Butterfield GE, Wolfel EE, Casazza GA, Lopaschuk 55. Casey DP, Mohamed EA, Joyner MJ. Role of nitric oxide and adenosine
GD, Brooks GA. Evaluation of exercise and training on muscle lipid in the onset of vasodilation during dynamic forearm exercise. Eur J Appl
metabolism. Am J Physiol 276: E106-E117, 1999. Physiol 113: 295-303, 2013.
29. Bergstrom J. Percutaneous needle biopsy of skeletal muscle in phys- 56. Casey DP, Walker BG, Ranadive SM, Taylor JL, Joyner MJ. Contri-
iological and clinical research. Scand J Clin Lab Invest 35: 609-616, bution of nitric oxide in the contraction-induced rapid vasodilation in
1975. young and older adults. J Appl Physiol (1985) 115: 446-455, 2013.
30. Bergstrom J, Hermansen L, Hultman E, Saltin B. Diet, muscle glycogen 57. Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller
and physical performance. Acta Physiol Scand 71: 140-150, 1967. OI, Sullivan ID, Lloyd JK, Deanfield JE. Non-invasive detection of
31. Bertovic DA, Waddell TK, Gatzka CD, Cameron JD, Dart AM, King- endothelial dysfunction in children and adults at risk of atherosclerosis.
well BA. Muscular strength training is associated with low arterial Lancet 340: 1111-1115, 1992.
compliance and high pulse pressure. Hypertension 33: 1385-1391, 58. Cerretelli P, Samaja M. Acid-base balance at exercise in normoxia and
1999. in chronic hypoxia. Revisiting the “lactate paradox”. Eur J Appl Physiol
32. Bevegard BS, Shepherd JT. Reaction in man of resistance and capacity 90: 431-448, 2003.
vessels in forearm and hand to leg exercise. J Appl Physiol 21: 123-132, 59. Chavoshan B, Sander M, Sybert TE, Hansen J, Victor RG, Thomas
1966. GD. Nitric oxide-dependent modulation of sympathetic neural control
33. Birk GK, Dawson EA, Atkinson C, Haynes A, Cable NT, Thijssen DH, of oxygenation in exercising human skeletal muscle. J Physiol 540:
Green DJ. Brachial artery adaptation to lower limb exercise training: 377-386, 2002.
Role of shear stress. J Appl Physiol (1985) 112: 1653-1658, 2012. 60. Chen SJ, Wu CC, Yen MH. Exercise training activates large-
34. Black JM, Stohr EJ, Shave R, Esformes JI. Influence of exercise training conductance calcium-activated K(+) channels and enhances nitric oxide
mode on arterial diameter: A systematic review and meta-analysis. J Sci production in rat mesenteric artery and thoracic aorta. J Biomed Sci 8:
Med Sport 2014. pii: S1440-2440(14)00639-2. doi: 10.1016. 248-255, 2001.
35. Blomqvist CG, Saltin B. Cardiovascular adaptations to physical train- 61. Christensen EH. Beitriige zur Physiologie schwerer korperlicher
ing. Annu Rev Physiol 45: 169-189, 1983. Arbeit. V. Mitteilung: V. Mitteilung: Minutenvolumen und Schlagvol-
36. Blomstrand E, Radegran G, Saltin B. Maximum rate of oxygen uptake umen des Herzens warend schwerer ktirperlicher Arbeit. Arbeitsphysi-
by human skeletal muscle in relation to maximal activities of enzymes ologie 4: 470-502, 1931.
in the Krebs cycle. J Physiol 501(Pt 2): 455-460, 1997. 62. Clausen JP. Effect of physical training on cardiovascular adjustments
37. Bolduc V, Thorin-Trescases N, Thorin E. Endothelium-dependent con- to exercise in man. Physiol Rev 57: 779-815, 1977.
trol of cerebrovascular functions through age: Exercise for healthy cere- 63. Clausen JP, Klausen K, Rasmussen B, Trap-Jensen J. Central and
brovascular aging. Am J Physiol Heart Circ Physiol 305: H620-H633, peripheral circulatory changes after training of the arms or legs. Am
2013. J Physiol 225: 675-682, 1973.
38. Bolz SS, Fisslthaler B, Pieperhoff S, de WC, Fleming I, Busse R, Pohl 64. Clifford PS, Kluess HA, Hamann JJ, Buckwalter JB, Jasperse JL.
U. Antisense oligonucleotides against cytochrome P450 2C8 attenuate Mechanical compression elicits vasodilatation in rat skeletal muscle
EDHF-mediated Ca(2+) changes and dilation in isolated resistance feed arteries. J Physiol 572: 561-567, 2006.
arteries. FASEB J 14: 255-260, 2000. 65. Cocks M, Shaw CS, Shepherd SO, Fisher JP, Ranasinghe A, Barker
39. Bonne TC, Doucende G, Fluck D, Jacobs RA, Nordsborg NB, Robach TA, Tipton KD, Wagenmakers AJ. Effect of resistance training on
P, Walther G, Lundby C. Phlebotomy eliminates the maximal cardiac microvascular density and eNOS content in skeletal muscle of sedentary
output response to six weeks of exercise training. Am J Physiol Regul men. Microcirculation 21: 738-746, 2014.
Integr Comp Physiol 306: R752-R760, 2014. 66. Cocks M, Shaw CS, Shepherd SO, Fisher JP, Ranasinghe AM, Barker
40. Boushel R, Fuentes T, Hellsten Y, Saltin B. Opposing effects of nitric TA, Tipton KD, Wagenmakers AJ. Sprint interval and endurance train-
oxide and prostaglandin inhibition on muscle mitochondrial Vo(2) dur- ing are equally effective in increasing muscle microvascular den-
ing exercise. Am J Physiol Regul Integr Comp Physiol 303: R94-100, sity and eNOS content in sedentary males. J Physiol 591: 641-656,
2012. 2013.
41. Boushel R, Langberg H, Gemmer C, Olesen J, Crameri R, Scheede 67. Cohen KD, Berg BR, Sarelius IH. Remote arteriolar dilations in
C, Sander M, Kjaer M. Combined inhibition of nitric oxide and response to muscle contraction under capillaries. Am J Physiol Heart
prostaglandins reduces human skeletal muscle blood flow during exer- Circ Physiol 278: H1916-H1923, 2000.
cise. J Physiol 543: 691-698, 2002. 68. Convertino VA. Blood volume: Its adaptation to endurance training.
42. Breen E, Tang K, Olfert M, Knapp A, Wagner P. Skeletal muscle Med Sci Sports Exerc 23: 1338-1348, 1991.
capillarity during hypoxia: VEGF and its activation. High Alt Med Biol 69. Convertino VA. Blood volume response to physical activity and inac-
9: 158-166, 2008. tivity. Am J Med Sci 334: 72-79, 2007.
43. Breen EC, Johnson EC, Wagner H, Tseng HM, Sung LA, Wagner PD. 70. Convertino VA, Brock PJ, Keil LC, Bernauer EM, Greenleaf JE. Exer-
Angiogenic growth factor mRNA responses in muscle to a single bout cise training-induced hypervolemia: Role of plasma albumin, renin, and
of exercise. J Appl Physiol 81: 355-361, 1996. vasopressin. J Appl Physiol Respir Environ Exerc Physiol 48: 665-669,
44. Breisch EA, White FC, Nimmo LE, McKirnan MD, Bloor CM. 1980.
Exercise-induced cardiac hypertrophy: A correlation of blood flow and 71. Convertino VA, Keil LC, Bernauer EM, Greenleaf JE. Plasma volume,
microvasculature. J Appl Physiol (1985) 60: 1259-1267, 1986. osmolality, vasopressin, and renin activity during graded exercise in
45. Brown MD. Exercise and coronary vascular remodelling in the healthy man. J Appl Physiol Respir Environ Exerc Physiol 50: 123-128, 1981.
heart. Exp Physiol 88: 645-658, 2003. 72. Conway DE, Breckenridge MT, Hinde E, Gratton E, Chen CS, Schwartz
46. Brown MD, Hudlicka O. Modulation of physiological angiogenesis MA. Fluid shear stress on endothelial cells modulates mechanical ten-
in skeletal muscle by mechanical forces: Involvement of VEGF and sion across VE-cadherin and PECAM-1. Curr Biol 23: 1024-1030,
metalloproteinases. Angiogenesis 6: 1-14, 2003. 2013.
47. Buick FJ, Gledhill N, Froese AB, Spriet L, Meyers EC. Effect of induced 73. Cornelissen VA, Fagard RH. Effects of endurance training on blood
erythrocythemia on aerobic work capacity. J Appl Physiol Respir Env- pressure, blood pressure-regulating mechanisms, and cardiovascular
iron Exerc Physiol 48: 636-642, 1980. risk factors. Hypertension 46: 667-675, 2005.
48. Burnstock G, Arnett TR, Orriss IR. Purinergic signalling in the muscu- 74. Corr L, Burnstock G. Analysis of P2-purinoceptor subtypes on the
loskeletal system. Purinergic Signal 9: 541-572, 2013. smooth muscle and endothelium of rabbit coronary artery. J Cardiovasc
49. Busse R, Edwards G, Feletou M, Fleming I, Vanhoutte PM, Weston Pharmacol 23: 709-715, 1994.
AH. EDHF: Bringing the concepts together. Trends Pharmacol Sci 23: 75. Cousineau D, Ferguson RJ, de CJ, Gauthier P, Cote P, Bourassa M.
374-380, 2002. Catecholamines in coronary sinus during exercise in man before and
50. Busse R, Pohl U, Luckhoff A. Mechanisms controlling the production after training. J Appl Physiol Respir Environ Exerc Physiol 43: 801-806,
of endothelial autacoids. Z Kardiol 78(Suppl 6): 64-69, 1989. 1977.
51. Buvinic S, Almarza G, Bustamante M, Casas M, Lopez J, Riquelme M, 76. Coyle EF, Martin WH, III, Sinacore DR, Joyner MJ, Hagberg JM, Hol-
Saez JC, Huidobro-Toro JP, Jaimovich E. ATP released by electrical loszy JO. Time course of loss of adaptations after stopping prolonged
stimuli elicits calcium transients and gene expression in skeletal muscle. intense endurance training. J Appl Physiol Respir Environ Exerc Physiol
J Biol Chem 284: 34490-34505, 2009. 57: 1857-1864, 1984.
24 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
77. Crecelius AR, Kirby BS, Luckasen GJ, Larson DG, Dinenno FA. ATP- 103. Ekblom B, Hermansen L. Cardiac output in athletes. J Appl Physiol 25:
mediated vasodilatation occurs via activation of inwardly rectifying 619-625, 1968.
potassium channels in humans. J Physiol 590: 5349-5359, 2012. 104. El-Sayed MS, Ali N, El-Sayed AZ. Haemorheology in exercise and
78. Crecelius AR, Kirby BS, Richards JC, Garcia LJ, Voyles WF, Lar- training. Sports Med 35: 649-670, 2005.
son DG, Luckasen GJ, Dinenno FA. Mechanisms of ATP-mediated 105. Ellsworth ML, Sprague RS. Regulation of blood flow distribution in
vasodilation in humans: modest role for nitric oxide and vasodilating skeletal muscle: Role of erythrocyte-released ATP. J Physiol 590: 4985-
prostaglandins. Am J Physiol Heart Circ Physiol 301: H1302-H1310, 4991, 2012.
2011. 106. Eskurza I, Monahan KD, Robinson JA, Seals DR. Effect of acute and
79. Crecelius AR, Kirby BS, Voyles WF, Dinenno FA. Nitric oxide, but not chronic ascorbic acid on flow-mediated dilatation with sedentary and
vasodilating prostaglandins, contributes to the improvement of exercise physically active human ageing. J Physiol 556: 315-324, 2004.
hyperemia via ascorbic acid in healthy older adults. Am J Physiol Heart 107. Fadel PJ, Farias IM, Gallagher KM, Wang Z, Thomas GD. Oxidative
Circ Physiol 299: H1633-H1641, 2010. stress and enhanced sympathetic vasoconstriction in contracting mus-
80. Crenshaw AG, Friden J, Thornell LE, Hargens AR. Extreme endurance cles of nitrate-tolerant rats and humans. J Physiol 590: 395-407, 2012.
training: Evidence of capillary and mitochondria compartmentalization 108. Feletou M, Vanhoutte PM. Endothelium-derived hyperpolarizing fac-
in human skeletal muscle. Eur J Appl Physiol Occup Physiol 63: 173- tor: where are we now? Arterioscler Thromb Vasc Biol 26: 1215-1225,
178, 1991. 2006.
81. D’Andrea A, Riegler L, Cocchia R, Scarafile R, Salerno G, Gravino 109. Ferguson S, Gledhill N, Jamnik VK, Wiebe C, Payne N. Cardiac per-
R, Golia E, Vriz O, Citro R, Limongelli G, Calabro P, Di SG, Caso P, formance in endurance-trained and moderately active young women.
Russo MG, Bossone E, Calabro R. Left atrial volume index in highly Med Sci Sports Exerc 33: 1114-1119, 2001.
trained athletes. Am Heart J 159: 1155-1161, 2010. 110. Fisher WJ, White MJ. Training-induced adaptations in the central com-
82. Da Silva-Azevedo L, Baum O, Zakrzewicz A, Pries AR. Vascular mand and peripheral reflex components of the pressor response to iso-
endothelial growth factor is expressed in endothelial cells isolated metric exercise of the human triceps surae. J Physiol 520(Pt 2): 621-628,
from skeletal muscles of nitric oxide synthase knockout mice during 1999.
prazosin-induced angiogenesis. Biochem Biophys Res Commun 297: 111. Fisslthaler B, Fleming I, Busse R. EDHF: A cytochrome P450 metabo-
1270-1276, 2002. lite in coronary arteries. Semin Perinatol 24: 15-19, 2000.
83. Dawson JM, Hudlicka O. The effect of long-term activity on the 112. Folkow B, Grimby G, THULESIUS O. Adaptive structural changes of
microvasculature of rat glycolytic skeletal muscle. Int J Microcirc Clin the vascular walls in hypertension and their relation to the control of
Exp 8: 53-69, 1989. the peripheral resistance. Acta Physiol Scand 44: 255-272, 1958.
84. De MR, Gioseffi G, Nobrega AC, Tibirica E. Effects of exercise training 113. Forstermann U, Munzel T. Endothelial nitric oxide synthase in vascular
on the vascular reactivity of the whole kidney circulation in rabbits. disease: From marvel to menace. Circulation 113: 1708-1714, 2006.
J Appl Physiol (1985) 97: 683-688, 2004. 114. Forstermann U, Sessa WC. Nitric oxide synthases: regulation and func-
85. de WC, Jahrbeck B, Schafer C, Bolz SS, Pohl U. Nitric oxide opposes tion. Eur Heart J 33: 829-837d, 2012.
myogenic pressure responses predominantly in large arterioles in vivo. 115. Fortney SM, Wenger CB, Bove JR, Nadel ER. Effect of blood volume
Hypertension 31: 787-794, 1998. on forearm venous and cardiac stroke volume during exercise. J Appl
86. Deer RR, Heaps CL. Exercise training enhances multiple mechanisms Physiol Respir Environ Exerc Physiol 55: 884-890, 1983.
of relaxation in coronary arteries from ischemic hearts. Am J Physiol 116. Frandsen U, Bangsbo J, Langberg H, Saltin B, Hellsten Y. Inhibi-
Heart Circ Physiol 305: H1321-H1331, 2013. tion of nitric oxide synthesis by systemic N(G)-monomethyl-L-arginine
87. Delaney LE, Arce-Esquivel AA, Kuroki K, Laughlin MH. Exercise administration in humans: Effects on interstitial adenosine, prostacy-
training improves vasoreactivity in the knee artery. Int J Sports Med clin and potassium concentrations in resting and contracting skeletal
33: 114-122, 2012. muscle. J Vasc Res 37: 297-302, 2000.
88. Delp MD, McAllister RM, Laughlin MH. Exercise training alters aor- 117. Frandsen U, Hoffner L, Betak A, Saltin B, Bangsbo J, Hellsten Y.
tic vascular reactivity in hypothyroid rats. Am J Physiol 268: H1428- Endurance training does not alter the level of neuronal nitric oxide
H1435, 1995. synthase in human skeletal muscle. J Appl Physiol (1985) 89: 1033-
89. Dinenno FA, Jones PP, Seals DR, Tanaka H. Age-associated arte- 1038, 2000.
rial wall thickening is related to elevations in sympathetic activity in 118. Frandsenn U, Bangsbo J, Sander M, Hoffner L, Betak A, Saltin B,
healthy humans. Am J Physiol Heart Circ Physiol 278: H1205-H1210, Hellsten Y. Exercise-induced hyperaemia and leg oxygen uptake are
2000. not altered during effective inhibition of nitric oxide synthase with
90. Dinenno FA, Tanaka H, Monahan KD, Clevenger CM, Eskurza I, Des- N(G)-nitro-L-arginine methyl ester in humans. J Physiol 531: 257-264,
ouza CA, Seals DR. Regular endurance exercise induces expansive 2001.
arterial remodelling in the trained limbs of healthy men. J Physiol 534: 119. Frank O. The basic shape of the arterial pulse. First treatise: Mathemat-
287-295, 2001. ical analysis. J Mol Cell Cardiol 22: 255-277, 1990.
91. Donato AJ, Lesniewski LA, Delp MD. The effects of aging and exercise 120. Franke WD, Stephens GM, Schmid PG, III. Effects of intense exer-
training on endothelin-1 vasoconstrictor responses in rat skeletal muscle cise training on endothelium-dependent exercise-induced vasodilata-
arterioles. Cardiovasc Res 66: 393-401, 2005. tion. Clin Physiol 18: 521-528, 1998.
92. Durand S, Tartas M, Bouye P, Koitka A, Saumet JL, Abraham P. 121. Franzoni F, Ghiadoni L, Galetta F, Plantinga Y, Lubrano V, Huang Y,
Prostaglandins participate in the late phase of the vascular response to Salvetti G, Regoli F, Taddei S, Santoro G, Salvetti A. Physical activity,
acetylcholine iontophoresis in humans. J Physiol 561: 811-819, 2004. plasma antioxidant capacity, and endothelium-dependent vasodilation
93. Duza T, Sarelius IH. Conducted dilations initiated by purines in arte- in young and older men. Am J Hypertens 18: 510-516, 2005.
rioles are endothelium dependent and require endothelial Ca2+. Am J 122. Fu Q, Levine BD. Cardiovascular response to exercise in women. Med
Physiol Heart Circ Physiol 285: H26-H37, 2003. Sci Sports Exerc 37: 1433-1435, 2005.
94. Eftekhari A, Rahman A, Schaebel LH, Chen H, Rasmussen CV, Aalk- 123. Fu Q, Levine BD. Exercise and the autonomic nervous system. Handb
jaer C, Buus CL, Mulvany MJ. Chronic cystamine treatment inhibits Clin Neurol 117: 147-160, 2013.
small artery remodelling in rats. J Vasc Res 44: 471-482, 2007. 124. Gajdusek C, DiCorleto P, Ross R, Schwartz SM. An endothelial cell-
95. Egginton S. Invited review: Activity-induced angiogenesis. Pflugers derived growth factor. J Cell Biol 85: 467-472, 1980.
Arch 457: 963-977, 2009. 125. Galetta F, Franzoni F, Virdis A, Ghiadoni L, Taddei S, Salvetti A,
96. Egginton S. In vivo shear stress response. Biochem Soc Trans 39: 1633- Santoro G. Endothelium-dependent vasodilation and carotid artery wall
1638, 2011. remodeling in athletes and sedentary subjects. Atherosclerosis 186: 184-
97. Egginton S, Gaffney E. Tissue capillary supply–it’s quality not quantity 192, 2006.
that counts! Exp Physiol 95: 971-979, 2010. 126. Gavin TP, Robinson CB, Yeager RC, England JA, Nifong LW, Hickner
98. Egginton S, Hudlicka O. Selective long-term electrical stimulation RC. Angiogenic growth factor response to acute systemic exercise in
of fast glycolytic fibres increases capillary supply but not oxidative human skeletal muscle. J Appl Physiol 96: 19-24, 2004.
enzyme activity in rat skeletal muscles. Exp Physiol 85: 567-573, 2000. 127. Gavin TP, Ruster RS, Carrithers JA, Zwetsloot KA, Kraus RM, Evans
99. Egginton S, Hudlicka O, Brown MD, Walter H, Weiss JB, Bate A. Cap- CA, Knapp DJ, Drew JL, McCartney JS, Garry JP, Hickner RC. No
illary growth in relation to blood flow and performance in overloaded difference in the skeletal muscle angiogenic response to aerobic exercise
rat skeletal muscle. J Appl Physiol 85: 2025-2032, 1998. training between young and aged men. J Physiol 585: 231-239, 2007.
100. Egginton S, Zhou AL, Brown MD, Hudlicka O. Unorthodox angiogen- 128. Gavin TP, Spector DA, Wagner H, Breen EC, Wagner PD. Nitric
esis in skeletal muscle. Cardiovasc Res 49: 634-646, 2001. oxide synthase inhibition attenuates the skeletal muscle VEGF mRNA
101. Eitenmuller I, Volger O, Kluge A, Troidl K, Barancik M, Cai WJ, Heil response to exercise. J Appl Physiol (1985) 88: 1192-1198, 2000.
M, Pipp F, Fischer S, Horrevoets AJ, Schmitz-Rixen T, Schaper W. The 129. Gertz K, Priller J, Kronenberg G, Fink KB, Winter B, Schrock H, Ji
range of adaptation by collateral vessels after femoral artery occlusion. S, Milosevic M, Harms C, Bohm M, Dirnagl U, Laufs U, Endres M.
Circ Res 99: 656-662, 2006. Physical activity improves long-term stroke outcome via endothelial
102. Ekblom B, Goldbarg AN, Gullbring B. Response to exercise after blood nitric oxide synthase-dependent augmentation of neovascularization
loss and reinfusion. J Appl Physiol 33: 175-180, 1972. and cerebral blood flow. Circ Res 99: 1132-1140, 2006.
Volume 6, January 2016 25
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
130. Gillen CM, Lee R, Mack GW, Tomaselli CM, Nishiyasu T, Nadel ER. 155. Gute D, Laughlin MH, Amann JF. Regional changes in capillary sup-
Plasma volume expansion in humans after a single intense exercise ply in skeletal muscle of interval-sprint and low-intensity, endurance-
protocol. J Appl Physiol (1985) 71: 1914-1920, 1991. trained rats. Microcirculation 1: 183-193, 1994.
131. Gilligan DM, Panza JA, Kilcoyne CM, Waclawiw MA, Casino PR, 156. Guyton AC. Regulation of cardiac output. N Engl J Med 277: 805-812,
Quyyumi AA. Contribution of endothelium-derived nitric oxide to 1967.
exercise-induced vasodilation. Circulation 90: 2853-2858, 1994. 157. Guyton AC, Coleman TG, Granger HJ. Circulation: Overall regulation.
132. Gledhill N, Cox D, Jamnik R. Endurance athletes’ stroke volume does Annu Rev Physiol 34: 13-46, 1972.
not plateau: major advantage is diastolic function. Med Sci Sports Exerc 158. Hambrecht R, Wolf A, Gielen S, Linke A, Hofer J, Erbs S, Schoene
26: 1116-1121, 1994. N, Schuler G. Effect of exercise on coronary endothelial function in
133. Gliemann L, Nyberg M, Hellsten Y. Nitric oxide and reactive oxygen patients with coronary artery disease. N Engl J Med 342: 454-460,
species in limb vascular function: What is the effect of physical activity? 2000.
Free Radic Res 48: 71-83, 2014. 159. Hang J, Kong L, Gu JW, Adair TH. VEGF gene expression is upreg-
134. Gliemann L, Olesen J, Bienso RS, Schmidt J, Akerstrom T, Nyberg ulated in electrically stimulated rat skeletal muscle. Am J Physiol 269:
M, Lindqvist A, Bangsbo J, Hellsten Y. Resveratrol Modulates the H1827-H1831, 1995.
Angiogenic Response to Exercise Training in Skeletal Muscle of Aged 160. Hansen AH, Nielsen JJ, Saltin B, Hellsten Y. Exercise training normal-
Men. Am J Physiol Heart Circ Physiol 307: H1111-H1119, 2014. izes skeletal muscle vascular endothelial growth factor levels in patients
135. Gliemann L, Schmidt JF, Olesen J, Bienso RS, Peronard SL, Grand- with essential hypertension. J Hypertens 28: 1176-1185, 2010.
jean SU, Mortensen SP, Nyberg M, Bangsbo J, Pilegaard H, Hellsten 161. Hansen AH, Nyberg M, Bangsbo J, Saltin B, Hellsten Y. Exercise
Y. Resveratrol blunts the positive effects of exercise training on cardio- training alters the balance between vasoactive compounds in skeletal
vascular health in aged men. J Physiol 591: 5047-5059, 2013. muscle of individuals with essential hypertension. Hypertension 58:
136. Gloe T, Riedmayr S, Sohn HY, Pohl U. The 67-kDa laminin-binding 943-949, 2011.
protein is involved in shear stress-dependent endothelial nitric-oxide 162. Hansen J, Thomas GD, Harris SA, Parsons WJ, Victor RG. Differential
synthase expression. J Biol Chem 274: 15996-16002, 1999. sympathetic neural control of oxygenation in resting and exercising
137. Gomez-Cabrera MC, Domenech E, Vina J. Moderate exercise is an human skeletal muscle. J Clin Invest 98: 584-596, 1996.
antioxidant: Upregulation of antioxidant genes by training. Free Radic 163. Hansen J, Thomas GD, Jacobsen TN, Victor RG. Muscle metaboreflex
Biol Med 44: 126-131, 2008. triggers parallel sympathetic activation in exercising and resting human
138. Gonzalez-Alonso J, Mora-Rodriguez R, Below PR, Coyle EF. Dehy- skeletal muscle. Am J Physiol 266: H2508-H2514, 1994.
dration reduces cardiac output and increases systemic and cutaneous 164. Hansen-Smith FM, Hudlicka O, Egginton S. In vivo angiogenesis in
vascular resistance during exercise. J Appl Physiol (1985) 79: 1487- adult rat skeletal muscle: Early changes in capillary network architec-
1496, 1995. ture and ultrastructure. Cell Tissue Res 286: 123-136, 1996.
139. Gonzalez-Alonso J, Olsen DB, Saltin B. Erythrocyte and the regulation 165. Harris MB, Mitchell BM, Sood SG, Webb RC, Venema RC. Increased
of human skeletal muscle blood flow and oxygen delivery: Role of nitric oxide synthase activity and Hsp90 association in skeletal mus-
circulating ATP. Circ Res 91: 1046-1055, 2002. cle following chronic exercise. Eur J Appl Physiol 104: 795-802,
140. Green DJ, Cable NT, Fox C, Rankin JM, Taylor RR. Modification of 2008.
forearm resistance vessels by exercise training in young men. J Appl 166. Haskell WL, Sims C, Myll J, Bortz WM, St Goar FG, Alderman EL.
Physiol (1985) 77: 1829-1833, 1994. Coronary artery size and dilating capacity in ultradistance runners.
141. Green DJ, Dawson EA, Groenewoud HM, Jones H, Thijssen DH. Is Circulation 87: 1076-1082, 1993.
flow-mediated dilation nitric oxide mediated?: A meta-analysis. Hyper- 167. Hauser AM, Dressendorfer RH, Vos M, Hashimoto T, Gordon S, Tim-
tension 63: 376-382, 2014. mis GC. Symmetric cardiac enlargement in highly trained endurance
142. Green DJ, Eijsvogels T, Bouts YM, Maiorana AJ, Naylor LH, Scholten athletes: A two-dimensional echocardiographic study. Am Heart J 109:
RR, Spaanderman ME, Pugh CJ, Sprung VS, Schreuder T, Jones H, 1038-1044, 1985.
Cable T, Hopman MT, Thijssen DH. Exercise training and artery func- 168. Hayes SG, McCord JL, Rainier J, Liu Z, Kaufman MP. Role played by
tion in humans: Nonresponse and its relationship to cardiovascular risk acid-sensitive ion channels in evoking the exercise pressor reflex. Am J
factors. J Appl Physiol (1985) 117: 345-352, 2014. Physiol Heart Circ Physiol 295: H1720-H1725, 2008.
143. Green DJ, Fowler DT, O’Driscoll JG, Blanksby BA, Taylor RR. 169. Heerkens EH, Izzard AS, Heagerty AM. Integrins, vascular remodeling,
Endothelium-derived nitric oxide activity in forearm vessels of tennis and hypertension. Hypertension 49: 1-4, 2007.
players. J Appl Physiol (1985) 81: 943-948, 1996. 170. Heinicke K, Wolfarth B, Winchenbach P, Biermann B, Schmid A,
144. Green DJ, Maiorana A, O’Driscoll G, Taylor R. Effect of exercise train- Huber G, Friedmann B, Schmidt W. Blood volume and hemoglobin
ing on endothelium-derived nitric oxide function in humans. J Physiol mass in elite athletes of different disciplines. Int J Sports Med 22:
561: 1-25, 2004. 504-512, 2001.
145. Green DJ, O’Driscoll G, Blanksby BA, Taylor RR. Control of skele- 171. Heinonen I, Kudomi N, Kemppainen J, Kiviniemi A, Noponen T, Luo-
tal muscle blood flow during dynamic exercise: Contribution of tolahti M, Luoto P, Oikonen V, Sipila HT, Kopra J, Mononen I, Duncker
endothelium-derived nitric oxide. Sports Med 21: 119-146, 1996. DJ, Knuuti J, Kalliokoski KK. Myocardial blood flow and its transit
146. Green DJ, Rowley N, Spence A, Carter H, Whyte G, George K, Naylor time, oxygen utilization, and efficiency of highly endurance-trained
LH, Cable NT, Dawson EA, DH JT. Why isn’t flow-mediated dilation human heart. Basic Res Cardiol 109: 413, 2014.
enhanced in athletes? Med Sci Sports Exerc 45: 75-82, 2013. 172. Heinonen I, Nesterov SV, Liukko K, Kemppainen J, Nagren K, Luo-
147. Green DJ, Spence A, Rowley N, Thijssen DH, Naylor LH. Vascular tolahti M, Virsu P, Oikonen V, Nuutila P, Kujala UM, Kainulainen
adaptation in athletes: is there an ‘athlete’s artery’? Exp Physiol 97: H, Boushel R, Knuuti J, Kalliokoski KK. Myocardial blood flow and
295-304, 2012. adenosine A2A receptor density in endurance athletes and untrained
148. Griffin KL, Laughlin MH, Parker JL. Exercise training improves men. J Physiol 586: 5193-5202, 2008.
endothelium-mediated vasorelaxation after chronic coronary occlusion. 173. Heinonen I, Saltin B, Kemppainen J, Sipila HT, Oikonen V, Nuutila P,
J Appl Physiol (1985) 87: 1948-1956, 1999. Knuuti J, Kalliokoski K, Hellsten Y. Skeletal muscle blood flow and
149. Gunduz F, Kocer G, Ulker S, Meiselman HJ, Baskurt OK, Senturk UK. oxygen uptake at rest and during exercise in humans: A pet study with
Exercise training enhances flow-mediated dilation in spontaneously nitric oxide and cyclooxygenase inhibition. Am J Physiol Heart Circ
hypertensive rats. Physiol Res 60: 589-597, 2011. Physiol 300: H1510-H1517, 2011.
150. Gunnarsson TP, Christensen PM, Holse K, Christiansen D, Bangsbo 174. Heinonen I, Wendelin-Saarenhovi M, Kaskinoro K, Knuuti J, Scheinin
J. Effect of additional speed endurance training on performance and M, Kalliokoski KK. Inhibition of alpha-adrenergic tone disturbs the
muscle adaptations. Med Sci Sports Exerc 44: 1942-1948, 2012. distribution of blood flow in the exercising human limb. Am J Physiol
151. Gustafsson T, Bodin K, Sylven C, Gordon A, Tyni-Lenne R, Jansson E. Heart Circ Physiol 305: H163-H172, 2013.
Increased expression of VEGF following exercise training in patients 175. Hellsten Y, Jensen L, Thaning P, Nyberg M, Mortensen S. Impaired
with heart failure. Eur J Clin Invest 31: 362-366, 2001. formation of vasodilators in peripheral tissue in essential hypertension
152. Gustafsson T, Knutsson A, Puntschart A, Kaijser L, Nordqvist AC, is normalized by exercise training: Role of adenosine and prostacyclin.
Sundberg CJ, Jansson E. Increased expression of vascular endothelial J Hypertens 30: 2007-2014, 2012.
growth factor in human skeletal muscle in response to short-term one- 176. Hellsten Y, Maclean D, Radegran G, Saltin B, Bangsbo J. Adenosine
legged exercise training. Pflugers Arch 444: 752-759, 2002. concentrations in the interstitium of resting and contracting human
153. Gustafsson T, Puntschart A, Kaijser L, Jansson E, Sundberg CJ. skeletal muscle. Circulation 98: 6-8, 1998.
Exercise-induced expression of angiogenesis-related transcription and 177. Hellsten Y, Nyberg M, Jensen LG, Mortensen SP. Vasodilator inter-
growth factors in human skeletal muscle. Am J Physiol 276: H679- actions in skeletal muscle blood flow regulation. J Physiol 590: 6297-
H685, 1999. 6305, 2012.
154. Gustafsson T, Rundqvist H, Norrbom J, Rullman E, Jansson E, Sund- 178. Hellsten Y, Rufener N, Nielsen JJ, Hoier B, Krustrup P, Bangsbo J.
berg CJ. The influence of physical training on the angiopoietin and Passive leg movement enhances interstitial VEGF protein, endothelial
VEGF-A systems in human skeletal muscle. J Appl Physiol 103: 1012- cell proliferation, and eNOS mRNA content in human skeletal muscle.
1020, 2007. Am J Physiol Regul Integr Comp Physiol 294: R975-R982, 2008.
26 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
179. Henschen S. Skilauf und Skiwettlauf. Eine medizinische Sportsstudie. 5-day aerobic training in a warm environment in young men. J Appl
Mitt Med klin upsala 2: 15-18, 1899. Physiol (1985) 110: 972-980, 2011.
180. Hershey JC, Baskin EP, Glass JD, Hartman HA, Gilberto DB, Rogers 205. Ingjer F. Capillary supply and mitochondrial content of different skele-
IT, Cook JJ. Revascularization in the rabbit hindlimb: dissociation tal muscle fiber types in untrained and endurance-trained men. A histo-
between capillary sprouting and arteriogenesis. Cardiovasc Res 49: chemical and ultrastructural study. Eur J Appl Physiol Occup Physiol
618-625, 2001. 40: 197-209, 1979.
181. Higashi Y, Sasaki S, Kurisu S, Yoshimizu A, Sasaki N, Mat- 206. Ingjer F. Effects of endurance training on muscle fibre ATP-ase activity,
suura H, Kajiyama G, Oshima T. Regular aerobic exercise augments capillary supply and mitochondrial content in man. J Physiol 294: 419-
endothelium-dependent vascular relaxation in normotensive as well as 432, 1979.
hypertensive subjects: Role of endothelium-derived nitric oxide. Cir- 207. Ito WD, Arras M, Scholz D, Winkler B, Htun P, Schaper W. Angiogen-
culation 100: 1194-1202, 1999. esis but not collateral growth is associated with ischemia after femoral
182. Higginbotham MB, Morris KG, Williams RS, McHale PA, Coleman artery occlusion. Am J Physiol 273: H1255-H1265, 1997.
RE, Cobb FR. Regulation of stroke volume during submaximal, maxi- 208. Jacobs RA, Rasmussen P, Siebenmann C, Diaz V, Gassmann M, Pesta
mal upright exercise in normal man. Circ Res 58: 281-291, 1986. D, Gnaiger E, Nordsborg NB, Robach P, Lundby C. Determinants of
183. Hildick-Smith DJ, Johnson PJ, Wisbey CR, Winter EM, Shapiro time trial performance and maximal incremental exercise in highly
LM. Coronary flow reserve is supranormal in endurance athletes: An trained endurance athletes. J Appl Physiol (1985) 111: 1422-1430,
adenosine transthoracic echocardiographic study. Heart 84: 383-389, 2011.
2000. 209. Jendzjowsky NG, DeLorey DS. Short-term exercise training enhances
184. Hillig T, Krustrup P, Fleming I, Osada T, Saltin B, Hellsten Y. functional sympatholysis through a nitric oxide-dependent mechanism.
Cytochrome P450 2C9 plays an important role in the regulation of J Physiol 591: 1535-1549, 2013.
exercise-induced skeletal muscle blood flow and oxygen uptake in 210. Jensen L, Bangsbo J, Hellsten Y. Effect of high intensity training on
humans. J Physiol 546: 307-314, 2003. capillarization and presence of angiogenic factors in human skeletal
185. Ho CW, Beard JL, Farrell PA, Minson CT, Kenney WL. Age, fitness, muscle. J Physiol 557: 571-582, 2004.
and regional blood flow during exercise in the heat. J Appl Physiol 211. Jensen L, Bangsbo J, Hellsten Y. Effect of high intensity training on
(1985) 82: 1126-1135, 1997. capillarization and presence of angiogenic factors in human skeletal
186. Ho KW, Roy RR, Taylor JF, Heusner WW, Van Huss WD. Differential muscle. J Physiol 557: 571-582, 2004.
effects of running and weight-lifting on the rat coronary arterial tree. 212. Jensen L, Pilegaard H, Neufer PD, Hellsten Y. Effect of acute exer-
Med Sci Sports Exerc 15: 472-477, 1983. cise and exercise training on VEGF splice variants in human skeletal
187. Hocking DC, Titus PA, Sumagin R, Sarelius IH. Extracellular matrix muscle. Am J Physiol Regul Integr Comp Physiol 287: R397-R402,
fibronectin mechanically couples skeletal muscle contraction with local 2004.
vasodilation. Circ Res 102: 372-379, 2008. 213. Jensen L, Schjerling P, Hellsten Y. Regulation of VEGF and bFGF
188. Hoffner L, Nielsen JJ, Langberg H, Hellsten Y. Exercise but not mRNA expression and other proliferative compounds in skeletal muscle
prostanoids enhance levels of vascular endothelial growth factor and cells. Angiogenesis 7: 255-267, 2004.
other proliferative agents in human skeletal muscle interstitium. J Phys- 214. Jordao MT, Ladd FV, Coppi AA, Chopard RP, Michelini LC. Exercise
iol 550: 217-225, 2003. training restores hypertension-induced changes in the elastic tissue of
189. Hoglund C. Enlarged left atrial dimension in former endurance athletes: the thoracic aorta. J Vasc Res 48: 513-524, 2011.
An echocardiographic study. Int J Sports Med 7: 133-136, 1986. 215. Joyner MJ, Freund BJ, Jilka SM, Hetrick GA, Martinez E, Ewy GA,
190. Hoier B, Hellsten Y. Exercise-induced capillary growth in human skele- Wilmore JH. Effects of beta-blockade on exercise capacity of trained
tal muscle and the dynamics of VEGF. Microcirculation 21: 301-314, and untrained men: A hemodynamic comparison. J Appl Physiol (1985)
2014. 60: 1429-1434, 1986.
191. Hoier B, Nordsborg N, Andersen S, Jensen L, Nybo L, Bangsbo J, 216. Jozkowicz A, Cooke JP, Guevara I, Huk I, Funovics P, Pachinger O,
Hellsten Y. Pro- and anti-angiogenic factors in human skeletal muscle Weidinger F, Dulak J. Genetic augmentation of nitric oxide synthase
in response to acute exercise and training. J Physiol 590: 595-606, increases the vascular generation of VEGF. Cardiovasc Res 51: 773-
2012. 783, 2001.
192. Hoier B, Passos M, Bangsbo J, Hellsten Y. Intense intermittent exercise 217. Juel C, Klarskov C, Nielsen JJ, Krustrup P, Mohr M, Bangsbo J. Effect
provides weak stimulus for vascular endothelial growth factor secretion of high-intensity intermittent training on lactate and H+ release from
and capillary growth in skeletal muscle. Exp Physiol 98: 585-597, 2013. human skeletal muscle. Am J Physiol Endocrinol Metab 286: E245-
193. Hoier B, Prats C, Qvortrup K, Pilegaard H, Bangsbo J, Hellsten Y. Sub- E251, 2004.
cellular localization and mechanism of secretion of vascular endothelial 218. Kadoglou NP, Iliadis F, Liapis CD. Exercise and carotid atherosclerosis.
growth factor in human skeletal muscle. FASEB J 27: 3496-3504, 2013. Eur J Vasc Endovasc Surg 35: 264-272, 2008.
194. Hoier B, Rufener N, Bojsen-Moller J, Bangsbo J, Hellsten Y. The 219. Kalliokoski KK, Laaksonen MS, Knuuti J, Nuutila P. Perfusion distri-
effect of passive movement training on angiogenic factors and capillary bution between and within muscles during intermittent static exercise
growth in human skeletal muscle. J Physiol 588: 3833-3845, 2010. in endurance-trained and untrained men. Int J Sports Med 24: 400-403,
195. Hoogsteen J, Hoogeveen A, Schaffers H, Wijn PF, van der Wall EE. 2003.
Left atrial and ventricular dimensions in highly trained cyclists. Int J 220. Kalliokoski KK, Oikonen V, Takala TO, Sipila H, Knuuti J, Nuutila P.
Cardiovasc Imaging 19: 211-217, 2003. Enhanced oxygen extraction and reduced flow heterogeneity in exercis-
196. Hoppeler H. Vascular growth in hypoxic skeletal muscle. Adv Exp Med ing muscle in endurance-trained men. Am J Physiol Endocrinol Metab
Biol 474: 277-286, 1999. 280: E1015-E1021, 2001.
197. Hoppeler H, Howald H, Conley K, Lindstedt SL, Claassen H, Vock 221. Kanno S, Oda N, Abe M, Saito S, Hori K, Handa Y, Tabayashi K,
P, Weibel ER. Endurance training in humans: Aerobic capacity and Sato Y. Establishment of a simple and practical procedure applicable
structure of skeletal muscle. J Appl Physiol (1985) 59: 320-327, 1985. to therapeutic angiogenesis. Circulation 99: 2682-2687, 1999.
198. Hopper MK, Coggan AR, Coyle EF. Exercise stroke volume relative to 222. Kano Y, Shimegi S, Masuda K, Sakato H, Ohmori H, Katsuta S. Effects
plasma-volume expansion. J Appl Physiol (1985) 64: 404-408, 1988. of different intensity endurance training on the capillary network in rat
199. Huang A, Sun D, Koller A. Shear stress-induced release of skeletal muscle. Int J Microcirc Clin Exp 17: 93-96, 1997.
prostaglandin H(2) in arterioles of hypertensive rats. Hypertension 35: 223. Karlsson J, Saltin B. [Effect of physical training on lactate-, adenosine
925-930, 2000. triphosphate, and creatine phosphate concentration in working mus-
200. Huonker M, Schmid A, Schmidt-Trucksass A, Grathwohl D, Keul J. cles]. Nord Med 86: 1010, 1971.
Size and blood flow of central and peripheral arteries in highly trained 224. Katona PG, McLean M, Dighton DH, Guz A. Sympathetic and
able-bodied and disabled athletes. J Appl Physiol (1985) 95: 685-691, parasympathetic cardiac control in athletes and nonathletes at rest.
2003. J Appl Physiol Respir Environ Exerc Physiol 52: 1652-1657, 1982.
201. Iaia FM, Hellsten Y, Nielsen JJ, Fernstrom M, Sahlin K, Bangsbo 225. Kaufman MP, Rybicki KJ. Discharge properties of group III and IV
J. Four weeks of speed endurance training reduces energy expendi- muscle afferents: Their responses to mechanical and metabolic stimuli.
ture during exercise and maintains muscle oxidative capacity despite a Circ Res 61: I60-I65, 1987.
reduction in training volume. J Appl Physiol 106: 73-80, 2009. 226. Kellogg DL, Jr. In vivo mechanisms of cutaneous vasodilation and
202. Iaia FM, Perez-Gomez J, Thomassen M, Nordsborg NB, Hellsten Y, vasoconstriction in humans during thermoregulatory challenges. J Appl
Bangsbo J. Relationship between performance at different exercise Physiol (1985) 100: 1709-1718, 2006.
intensities and skeletal muscle characteristics. J Appl Physiol (1985) 227. Kellogg DL, Jr., Pergola PE, Piest KL, Kosiba WA, Crandall CG,
110: 1555-1563, 2011. Grossmann M, Johnson JM. Cutaneous active vasodilation in humans is
203. Iglarz M, Matrougui K, Levy BI, Henrion D. Chronic blockade of mediated by cholinergic nerve cotransmission. Circ Res 77: 1222-1228,
endothelin ETA receptors improves flow dependent dilation in resis- 1995.
tance arteries of hypertensive rats. Cardiovasc Res 39: 657-664, 1998. 228. Kiens B, Essen-Gustavsson B, Christensen NJ, Saltin B. Skeletal mus-
204. Ikegawa S, Kamijo Y, Okazaki K, Masuki S, Okada Y, Nose H. Effects cle substrate utilization during submaximal exercise in man: Effect of
of hypohydration on thermoregulation during exercise before and after endurance training. J Physiol 469: 459-478, 1993.
Volume 6, January 2016 27
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
229. Kingwell BA, Berry KL, Cameron JD, Jennings GL, Dart AM. Arterial 253. Leick L, Hellsten Y, Fentz J, Lyngby SS, Wojtaszewski JF, Hidalgo
compliance increases after moderate-intensity cycling. Am J Physiol J, Pilegaard H. PGC-1alpha mediates exercise-induced skeletal muscle
273: H2186-H2191, 1997. VEGF expression in mice. Am J Physiol Endocrinol Metab 297: E92-
230. Kirby BS, Voyles WF, Carlson RE, Dinenno FA. Graded sympatholytic 103, 2009.
effect of exogenous ATP on postjunctional alpha-adrenergic vasocon- 254. Leick L, Wojtaszewski JF, Johansen ST, Kiilerich K, Comes G, Hellsten
striction in the human forearm: Implications for vascular control in Y, Hidalgo J, Pilegaard H. PGC-1alpha is not mandatory for exercise-
contracting muscle. J Physiol 586: 4305-4316, 2008. and training-induced adaptive gene responses in mouse skeletal muscle.
231. Kirby BS, Voyles WF, Simpson CB, Carlson RE, Schrage WG, Dinenno Am J Physiol Endocrinol Metab 294: E463-E474, 2008.
FA. Endothelium-dependent vasodilatation and exercise hyperaemia in 255. Leinonen H, Salminen S, Peltokallio P. Capillary permeability and
ageing humans: Impact of acute ascorbic acid administration. J Physiol maximal blood flow in skeletal muscle in athletes and non-athletes
587: 1989-2003, 2009. measured by local clearances of 133Xe and 131I-. Scand J Clin Lab
232. Klausen K, Andersen LB, Pelle I. Adaptive changes in work capacity, Invest 38: 223-227, 1978.
skeletal muscle capillarization and enzyme levels during training and 256. Leung HS, Leung FP, Yao X, Ko WH, Chen ZY, Vanhoutte PM, Huang
detraining. Acta Physiol Scand 113: 9-16, 1981. Y. Endothelial mediators of the acetylcholine-induced relaxation of the
233. Klausen K, Secher NH, Clausen JP, Hartling O, Trap-Jensen J. Central rat femoral artery. Vascul Pharmacol 44: 299-308, 2006.
and regional circulatory adaptations to one-leg training. J Appl Physiol 257. Levine BD, Lane LD, Buckey JC, Friedman DB, Blomqvist CG. Left
Respir Environ Exerc Physiol 52: 976-983, 1982. ventricular pressure-volume and Frank-Starling relations in endurance
234. Kozakova M, Galetta F, Gregorini L, Bigalli G, Franzoni F, Giusti C, athletes. Implications for orthostatic tolerance and exercise perfor-
Palombo C. Coronary vasodilator capacity and epicardial vessel remod- mance. Circulation 84: 1016-1023, 1991.
eling in physiological and hypertensive hypertrophy. Hypertension 36: 258. Lewis SF, Nylander E, Gad P, Areskog NH. Non-autonomic component
343-349, 2000. in bradycardia of endurance trained men at rest and during exercise.
235. Kramer AF, Hahn S, Cohen NJ, Banich MT, McAuley E, Harrison CR, Acta Physiol Scand 109: 297-305, 1980.
Chason J, Vakil E, Bardell L, Boileau RA, Colcombe A. Ageing, fitness 259. Lexell J, Taylor C, Sjostrom M. Analysis of sampling errors in biopsy
and neurocognitive function. Nature 400: 418-419, 1999. techniques using data from whole muscle cross sections. J Appl Physiol
236. Krip B, Gledhill N, Jamnik V, Warburton D. Effect of alterations in (1985) 59: 1228-1235, 1985.
blood volume on cardiac function during maximal exercise. Med Sci 260. Li J, King NC, Sinoway LI. ATP concentrations and muscle tension
Sports Exerc 29: 1469-1476, 1997. increase linearly with muscle contraction. J Appl Physiol 95: 577-583,
237. Krustrup P, Hellsten Y, Bangsbo J. Intense interval training enhances 2003.
human skeletal muscle oxygen uptake in the initial phase of dynamic 261. Li Z, Lu N, Shi L. Exercise training reverses alterations in Kv and
exercise at high but not at low intensities. J Physiol 559: 335-345, 2004. BKCa channel molecular expression in thoracic aorta smooth muscle
238. Kvernmo HD, Stefanovska A, Kirkeboen KA, Osterud B, Kvernebo K. cells from spontaneously hypertensive rats. J Vasc Res 51: 447-457,
Enhanced endothelium-dependent vasodilatation in human skin vas- 2014.
culature induced by physical conditioning. Eur J Appl Physiol Occup 262. Linke A, Schoene N, Gielen S, Hofer J, Erbs S, Schuler G, Hambrecht R.
Physiol 79: 30-36, 1998. Endothelial dysfunction in patients with chronic heart failure: Systemic
239. Laaksonen MS, Kalliokoski KK, Luotolahti M, Kemppainen J, Teras effects of lower-limb exercise training. J Am Coll Cardiol 37: 392-397,
M, Kyrolainen H, Nuutila P, Knuuti J. Myocardial perfusion during 2001.
exercise in endurance-trained and untrained humans. Am J Physiol 263. Lloyd PG, Prior BM, Li H, Yang HT, Terjung RL. VEGF receptor
Regul Integr Comp Physiol 293: R837-R843, 2007. antagonism blocks arteriogenesis, but only partially inhibits angiogen-
240. Langille BL, O’Donnell F. Reductions in arterial diameter produced by esis, in skeletal muscle of exercise-trained rats. Am J Physiol Heart
chronic decreases in blood flow are endothelium-dependent. Science Circ Physiol 288: H759-H768, 2005.
231: 405-407, 1986. 264. Lloyd PG, Prior BM, Yang HT, Terjung RL. Angiogenic growth factor
241. Lash JM. Exercise training enhances adrenergic constriction and dila- expression in rat skeletal muscle in response to exercise training. Am J
tion in the rat spinotrapezius muscle. J Appl Physiol (1985) 85: 168-174, Physiol Heart Circ Physiol 284: H1668-H1678, 2003.
1998. 265. Lloyd PG, Yang HT, Terjung RL. Arteriogenesis and angiogenesis in
242. Lash JM, Bohlen HG. Time- and order-dependent changes in func- rat ischemic hindlimb: Role of nitric oxide. Am J Physiol Heart Circ
tional and NO-mediated dilation during exercise training. J Appl Phys- Physiol 281: H2528-H2538, 2001.
iol (1985) 82: 460-468, 1997. 266. Luetkemeier MJ, Thomas EL. Hypervolemia and cycling time trial
243. Lash JM, Reilly T, Thomas M, Bohlen HG. Adrenergic and pressure- performance. Med Sci Sports Exerc 26: 503-509, 1994.
dependent vascular regulation in sedentary and trained rats. Am J Phys- 267. Lundby C, Gassmann M, Pilegaard H. Regular endurance training
iol 265: H1064-H1073, 1993. reduces the exercise induced HIF-1alpha and HIF-2alpha mRNA
244. Laterza MC, de Matos LD, Trombetta IC, Braga AM, Roveda F, Alves expression in human skeletal muscle in normoxic conditions. Eur J
MJ, Krieger EM, Negrao CE, Rondon MU. Exercise training restores Appl Physiol 96: 363-369, 2006.
baroreflex sensitivity in never-treated hypertensive patients. Hyperten- 268. Lundgren Y, Hallback M, Weiss L, Folkow B. Rate and extent of adap-
sion 49: 1298-1306, 2007. tive cardiovascular changes in rats during experimental renal hyperten-
245. Laughlin MH, Bowles DK, Duncker DJ. The coronary circulation in sion. Acta Physiol Scand 91: 103-115, 1974.
exercise training. Am J Physiol Heart Circ Physiol 302: H10-H23, 2012. 269. Maeda S, Sugawara J, Yoshizawa M, Otsuki T, Shimojo N, Jesmin
246. Laughlin MH, Cook JD, Tremble R, Ingram D, Colleran PN, Turk JR. S, Ajisaka R, Miyauchi T, Tanaka H. Involvement of endothelin-1 in
Exercise training produces nonuniform increases in arteriolar density habitual exercise-induced increase in arterial compliance. Acta Physiol
of rat soleus and gastrocnemius muscle. Microcirculation 13: 175-186, (Oxf) 196: 223-229, 2009.
2006. 270. Maeda S, Tanabe T, Miyauchi T, Otsuki T, Sugawara J, Iemitsu M,
247. Laughlin MH, Korthuis RJ, Sexton WL, Armstrong RB. Regional mus- Kuno S, Ajisaka R, Yamaguchi I, Matsuda M. Aerobic exercise training
cle blood flow capacity and exercise hyperemia in high-intensity trained reduces plasma endothelin-1 concentration in older women. J Appl
rats. J Appl Physiol (1985) 64: 2420-2427, 1988. Physiol (1985) 95: 336-341, 2003.
248. Laughlin MH, Ripperger J. Vascular transport capacity of hindlimb 271. Mairbaurl H. Red blood cells in sports: Effects of exercise and train-
muscles of exercise-trained rats. J Appl Physiol (1985) 62: 438-443, ing on oxygen supply by red blood cells. Front Physiol 4: 332,
1987. 2013.
249. Laughlin MH, Roseguini B. Mechanisms for exercise training-induced 272. Martin EA, Nicholson WT, Eisenach JH, Charkoudian N, Joyner MJ.
increases in skeletal muscle blood flow capacity: Differences with inter- Influences of adenosine receptor antagonism on vasodilator responses
val sprint training versus aerobic endurance training. J Physiol Phar- to adenosine and exercise in adenosine responders and nonresponders.
macol 59(Suppl 7): 71-88, 2008. J Appl Physiol (1985) 101: 1678-1684, 2006.
250. Laughlin MH, Schrage WG, McAllister RM, Garverick HA, Jones 273. Mathieu-Costello O. Muscle adaptation to altitude: Tissue capillarity
AW. Interaction of gender and exercise training: Vasomotor reactivity and capacity for aerobic metabolism. High Alt Med Biol 2: 413-425,
of porcine skeletal muscle arteries. J Appl Physiol (1985) 90: 216-227, 2001.
2001. 274. Matsuda M, Nosaka T, Sato M, Iijima J, Ohshima N, Fukushima H.
251. Laughlin MH, Woodman CR, Schrage WG, Gute D, Price EM. Interval Effects of exercise training on biochemical and biomechanical proper-
sprint training enhances endothelial function and eNOS content in some ties of rat aorta. Angiology 40: 51-58, 1989.
arteries that perfuse white gastrocnemius muscle. J Appl Physiol (1985) 275. McAllister RM. Adaptations in control of blood flow with training:
96: 233-244, 2004. Splanchnic and renal blood flows. Med Sci Sports Exerc 30: 375-381,
252. Lee SJ, Yoo JS. [The effects of a physical activity reinforcement pro- 1998.
gram on exercise compliance, depression, and anxiety in continuous 276. McAllister RM, Jasperse JL, Laughlin MH. Nonuniform effects of
ambulatory peritoneal dialysis patients]. Taehan Kanho Hakhoe Chi endurance exercise training on vasodilation in rat skeletal muscle. J Appl
34: 440-448, 2004. Physiol (1985) 98: 753-761, 2005.
28 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
277. McAllister RM, Newcomer SC, Laughlin MH. Vascular nitric oxide: 299. Moynes J, Bentley RF, Bravo M, Kellawan JM, Tschakovsky ME.
Effects of exercise training in animals. Appl Physiol Nutr Metab 33: Persistence of functional sympatholysis post-exercise in human skeletal
173-178, 2008. muscle. Front Physiol 4: 131, 2013.
278. McAllister RM, Price EM. Effects of exercise training on vasodilatory 300. Mueller PJ. Exercise training and sympathetic nervous system activity:
protein expression and activity in rats. Eur J Appl Physiol 110: 1019- Evidence for physical activity dependent neural plasticity. Clin Exp
1027, 2010. Pharmacol Physiol 34: 377-384, 2007.
279. Meininger CJ, Schelling ME, Granger HJ. Adenosine and hypoxia 301. Muller JM, Myers PR, Laughlin MH. Vasodilator responses of coronary
stimulate proliferation and migration of endothelial cells. Am J Physiol resistance arteries of exercise-trained pigs. Circulation 89: 2308-2314,
255: H554-H562, 1988. 1994.
280. Meredith IT, Friberg P, Jennings GL, Dewar EM, Fazio VA, Lambert 302. Mulvany MJ, Hansen OK, Aalkjaer C. Direct evidence that the greater
GW, Esler MD. Exercise training lowers resting renal but not cardiac contractility of resistance vessels in spontaneously hypertensive rats
sympathetic activity in humans. Hypertension 18: 575-582, 1991. is associated with a narrowed lumen, a thickened media, and an
281. Michiels C, Arnould T, Remacle J. Endothelial cell responses to increased number of smooth muscle cell layers. Circ Res 43: 854-864,
hypoxia: Initiation of a cascade of cellular interactions. Biochim Bio- 1978.
phys Acta 1497: 1-10, 2000. 303. Munch GD, Svendsen JH, Damsgaard R, Secher NH, Gonzalez-Alonso
282. Mitchell JH, Kaufman MP, Iwamoto GA. The exercise pressor reflex: J, Mortensen SP. Maximal heart rate does not limit cardiovascular
Its cardiovascular effects, afferent mechanisms, and central pathways. capacity in healthy humans: Insight from right atrial pacing during
Annu Rev Physiol 45: 229-242, 1983. maximal exercise. J Physiol 592: 377-390, 2014.
283. Miyachi M, Tanaka H, Yamamoto K, Yoshioka A, Takahashi K, 304. Murohara T, Horowitz JR, Silver M, Tsurumi Y, Chen D, Sullivan
Onodera S. Effects of one-legged endurance training on femoral arte- A, Isner JM. Vascular endothelial growth factor/vascular permeability
rial and venous size in healthy humans. J Appl Physiol (1985) 90: factor enhances vascular permeability via nitric oxide and prostacyclin.
2439-2444, 2001. Circulation 97: 99-107, 1998.
284. Mohiaddin RH, Underwood SR, Bogren HG, Firmin DN, Klipstein 305. Murrant CL, Sarelius IH. Local and remote arteriolar dilations initiated
RH, Rees RS, Longmore DB. Regional aortic compliance studied by by skeletal muscle contraction. Am J Physiol Heart Circ Physiol 279:
magnetic resonance imaging: the effects of age, training, and coronary H2285-H2294, 2000.
artery disease. Br Heart J 62: 90-96, 1989. 306. Musch TI, Terrell JA, Hilty MR. Effects of high-intensity sprint training
285. Mombouli JV, Nakashima M, Hamra M, Vanhoutte PM. Endothelium- on skeletal muscle blood flow in rats. J Appl Physiol (1985) 71: 1387-
dependent relaxation and hyperpolarization evoked by bradykinin in 1395, 1991.
canine coronary arteries: Enhancement by exercise-training. Br J Phar- 307. Naylor LH, Arnolda LF, Deague JA, Playford D, Maurogiovanni A,
macol 117: 413-418, 1996. O’Driscoll G, Green DJ. Reduced ventricular flow propagation velocity
286. Morganroth J, Maron BJ, Henry WL, Epstein SE. Comparative left in elite athletes is augmented with the resumption of exercise training.
ventricular dimensions in trained athletes. Ann Intern Med 82: 521- J Physiol 563: 957-963, 2005.
524, 1975. 308. Naylor LH, Carter H, FitzSimons MG, Cable NT, Thijssen DH, Green
287. Mortensen SP, Askew CD, Walker M, Nyberg M, Hellsten Y. The DJ. Repeated increases in blood flow, independent of exercise, enhance
hyperaemic response to passive leg movement is dependent on nitric conduit artery vasodilator function in humans. Am J Physiol Heart Circ
oxide: A new tool to evaluate endothelial nitric oxide function. J Physiol Physiol 300: H664-H669, 2011.
590: 4391-4400, 2012. 309. Naylor LH, O’Driscoll G, Fitzsimons M, Arnolda LF, Green DJ. Effects
288. Mortensen SP, Damsgaard R, Dawson EA, Secher NH, Gonzalez- of training resumption on conduit arterial diameter in elite rowers. Med
Alonso J. Restrictions in systemic and locomotor skeletal muscle per- Sci Sports Exerc 38: 86-92, 2006.
fusion, oxygen supply and VO2 during high-intensity whole-body exer- 310. Ng AV, Callister R, Johnson DG, Seals DR. Endurance exercise training
cise in humans. J Physiol 586: 2621-2635, 2008. is associated with elevated basal sympathetic nerve activity in healthy
289. Mortensen SP, Dawson EA, Yoshiga CC, Dalsgaard MK, Damsgaard R, older humans. J Appl Physiol (1985) 77: 1366-1374, 1994.
Secher NH, Gonzalez-Alonso J. Limitations to systemic and locomotor 311. Nicholson WT, Vaa B, Hesse C, Eisenach JH, Joyner MJ. Aging is
limb muscle oxygen delivery and uptake during maximal exercise in associated with reduced prostacyclin-mediated dilation in the human
humans. J Physiol 566: 273-285, 2005. forearm. Hypertension 53: 973-978, 2009.
290. Mortensen SP, Gonzalez-Alonso J, Bune LT, Saltin B, Pilegaard H, 312. Nyberg M. Vascular function and regulation of blood flow in resting and
Hellsten Y. ATP-induced vasodilation and purinergic receptors in the contracting skeletal muscle: Insight from essential hypertension, aging
human leg: Roles of nitric oxide, prostaglandins, and adenosine. Am J and physical activity (Dissertation). Department of nutrition, exercise
Physiol Regul Integr Comp Physiol 296: R1140-R1148, 2009. and sports faculty of science university of copenhagen, 2013.
291. Mortensen SP, Gonzalez-Alonso J, Damsgaard R, Saltin B, Hellsten 313. Nyberg M, Al-Khazraji BK, Mortensen SP, Jackson DN, Ellis CG,
Y. Inhibition of nitric oxide and prostaglandins, but not endothelial- Hellsten Y. Effect of extraluminal ATP application on vascular tone
derived hyperpolarizing factors, reduces blood flow and aerobic energy and blood flow in skeletal muscle: Implications for exercise hyperemia.
turnover in the exercising human leg. J Physiol 581: 853-861, 2007. Am J Physiol Regul Integr Comp Physiol 305: R281-R290, 2013.
292. Mortensen SP, Morkeberg J, Thaning P, Hellsten Y, Saltin B. Two 314. Nyberg M, Blackwell JR, Damsgaard R, Jones AM, Hellsten Y,
weeks of muscle immobilization impairs functional sympatholysis but Mortensen SP. Lifelong physical activity prevents an age-related reduc-
increases exercise hyperemia and the vasodilatory responsiveness to tion in arterial and skeletal muscle nitric oxide bioavailability in
infused ATP. Am J Physiol Heart Circ Physiol 302: H2074-H2082, humans. J Physiol 590: 5361-5370, 2012.
2012. 315. Nyberg M, Jensen LG, Thaning P, Hellsten Y, Mortensen SP. Role of
293. Mortensen SP, Nyberg M, Gliemann L, Thaning P, Saltin B, Hellsten nitric oxide and prostanoids in the regulation of leg blood flow and blood
Y. Exercise training modulates functional sympatholysis and alpha- pressure in humans with essential hypertension: effect of high-intensity
adrenergic vasoconstrictor responsiveness in hypertensive and nor- aerobic training. J Physiol 590: 1481-1494, 2012.
motensive individuals. J Physiol 592: 3063-3073, 2014. 316. Nyberg M, Mortensen SP, Cabo H, Gomez-Cabrera MC, Vina J, Hell-
294. Mortensen SP, Nyberg M, Thaning P, Saltin B, Hellsten Y. Adenosine sten Y. Roles of sedentary aging and lifelong physical activity in
contributes to blood flow regulation in the exercising human leg by exchange of glutathione across exercising human skeletal muscle. Free
increasing prostaglandin and nitric oxide formation. Hypertension 53: Radic Biol Med 73C: 166-173, 2014.
993-999, 2009. 317. Nyberg M, Mortensen SP, Hellsten Y. Physical activity opposes the
295. Mortensen SP, Nyberg M, Winding K, Saltin B. Lifelong physical age-related increase in skeletal muscle and plasma endothelin-1 levels
activity preserves functional sympatholysis and purinergic signalling and normalizes plasma endothelin-1 levels in individuals with essential
in the ageing human leg. J Physiol 590: 6227-6236, 2012. hypertension. Acta Physiol (Oxf) 207: 524-535, 2013.
296. Mortensen SP, Svendsen JH, Ersboll M, Hellsten Y, Secher NH, Saltin 318. Nyberg M, Mortensen SP, Thaning P, Saltin B, Hellsten Y. Interstitial
B. Skeletal muscle signaling and the heart rate and blood pressure and plasma adenosine stimulate nitric oxide and prostacyclin formation
response to exercise: Insight from heart rate pacing during exercise in human skeletal muscle. Hypertension 56: 1102-1108, 2010.
with a trained and a deconditioned muscle group. Hypertension 61: 319. Nyberg M, Seidelin K, Andersen TR, Overby NN, Hellsten Y, Bangsbo
1126-1133, 2013. J. Biomarkers of vascular function in premenopausal and recent post-
297. Mortensen SP, Thaning P, Nyberg M, Saltin B, Hellsten Y. Local menopausal women of similar age: Effect of exercise training. Am J
release of ATP into the arterial inflow and venous drainage of human Physiol Regul Integr Comp Physiol 306: R510-R517, 2014.
skeletal muscle: Insight from ATP determination with the intravascular 320. Olenich SA, Gutierrez-Reed N, Audet GN, Olfert IM. Temporal
microdialysis technique. J Physiol 589: 1847-1857, 2011. response of positive and negative regulators in response to acute and
298. Mourtzakis M, Gonzalez-Alonso J, Graham TE, Saltin B. Hemodynam- chronic exercise training in mice. J Physiol 591: 5157-5169, 2013.
ics and O2 uptake during maximal knee extensor exercise in untrained 321. Olfert IM, Birot O. Importance of anti-angiogenic factors in the regu-
and trained human quadriceps muscle: Effects of hyperoxia. J Appl lation of skeletal muscle angiogenesis. Microcirculation 18: 316-330,
Physiol 97: 1796-1802, 2004. 2011.
Volume 6, January 2016 29
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
322. Olfert IM, Breen EC, Gavin TP, Wagner PD. Temporal 349. Rein HSM. Die lokale Stoffwechseleinschrankung bei reflektoriseh-
thrombospondin-1 mRNA response in skeletal muscle exposed to acute nervoser Dureblutungdrosselung. Arch ges Physiol 239: 464, 1937.
and chronic exercise. Growth Factors 24: 253-259, 2006. 350. Reindell H, Roskamm H, Steim H. [The heart and blood circulation in
323. Olfert IM, Breen EC, Mathieu-Costello O, Wagner PD. Chronic athletes]. Med Welt 31: 1557-1563, 1960.
hypoxia attenuates resting and exercise-induced VEGF, flt-1, and flk-1 351. Remensnyder JP, Mitchell JH, Arnoff SJ. Functional sympatholysis
mRNA levels in skeletal muscle. J Appl Physiol 90: 1532-1538, 2001. during muscular activity. Observations on influence of carotid sinus on
324. Olfert IM, Breen EC, Mathieu-Costello O, Wagner PD. Skeletal mus- oxygen uptake. Circ Res 11: 370-380, 1962.
cle capillarity and angiogenic mRNA levels after exercise training in 352. Resnick N, Gimbrone MA, Jr. Hemodynamic forces are complex reg-
normoxia and chronic hypoxia. J Appl Physiol 91: 1176-1184, 2001. ulators of endothelial gene expression. FASEB J 9: 874-882, 1995.
325. Olfert IM, Howlett RA, Wagner PD, Breen EC. Myocyte vascular 353. Richardson RS, Poole DC, Knight DR, Kurdak SS, Hogan MC, Grassi
endothelial growth factor is required for exercise-induced skeletal mus- B, Johnson EC, Kendrick KF, Erickson BK, Wagner PD. High muscle
cle angiogenesis. Am J Physiol Regul Integr Comp Physiol 299: R1059- blood flow in man: is maximal O2 extraction compromised? J Appl
R1067, 2010. Physiol (1985) 75: 1911-1916, 1993.
326. Padilla J, Simmons GH, Bender SB, Arce-Esquivel AA, Whyte JJ, 354. Richardson RS, Saltin B. Human muscle blood flow and metabolism
Laughlin MH. Vascular effects of exercise: Endothelial adaptations studied in the isolated quadriceps muscles. Med Sci Sports Exerc 30:
beyond active muscle beds. Physiology (Bethesda) 26: 132-145, 2011. 28-33, 1998.
327. Padilla J, Simmons GH, Vianna LC, Davis MJ, Laughlin MH, Fadel 355. Richardson RS, Wagner H, Mudaliar SR, Henry R, Noyszewski EA,
PJ. Brachial artery vasodilatation during prolonged lower limb exercise: Wagner PD. Human VEGF gene expression in skeletal muscle: Effect
role of shear rate. Exp Physiol 96: 1019-1027, 2011. of acute normoxic and hypoxic exercise. Am J Physiol 277: H2247-
328. Papapetropoulos A, Garcia-Cardena G, Madri JA, Sessa WC. Nitric H2252, 1999.
oxide production contributes to the angiogenic properties of vascular 356. Richardson RS, Wagner H, Mudaliar SR, Saucedo E, Henry R, Wagner
endothelial growth factor in human endothelial cells. J Clin Invest 100: PD. Exercise adaptation attenuates VEGF gene expression in human
3131-3139, 1997. skeletal muscle. Am J Physiol Heart Circ Physiol 279: H772-H778,
329. Patterson GCWRF. The measurement of blood flow during reactive 2000.
hyperaemia in man. J Physiol 127: 13-4P, 1955. 357. Rivilis I, Milkiewicz M, Boyd P, Goldstein J, Brown MD, Egginton S,
330. Pearson JD, Gordon JL. P2 purinoceptors in the blood vessel wall. Hansen FM, Hudlicka O, Haas TL. Differential involvement of MMP-2
Biochem Pharmacol 38: 4157-4163, 1989. and VEGF during muscle stretch- versus shear stress-induced angio-
331. Pelliccia A, Culasso F, Di Paolo FM, Maron BJ. Physiologic left ven- genesis. Am J Physiol Heart Circ Physiol 283: H1430-H1438, 2002.
tricular cavity dilatation in elite athletes. Ann Intern Med 130: 23-31, 358. Roberts MF, Wenger CB, Stolwijk JA, Nadel ER. Skin blood flow
1999. and sweating changes following exercise training and heat acclimation.
332. Pelliccia A, Maron BJ, Culasso F, Spataro A, Caselli G. Athlete’s heart J Appl Physiol Respir Environ Exerc Physiol 43: 133-137, 1977.
in women. Echocardiographic characterization of highly trained elite 359. Robinson BF, Epstein SE, Beiser GD, Braunwald E. Control of heart
female athletes. JAMA 276: 211-215, 1996. rate by the autonomic nervous system. Studies in man on the inter-
333. Pelliccia A, Maron BJ, Spataro A, Proschan MA, Spirito P. The upper relation between baroreceptor mechanisms and exercise. Circ Res 19:
limit of physiologic cardiac hypertrophy in highly trained elite athletes. 400-411, 1966.
N Engl J Med 324: 295-301, 1991. 360. Roche DM, Rowland TW, Garrard M, Marwood S, Unnithan VB. Skin
334. Pelliccia A, Spataro A, Granata M, Biffi A, Caselli G, Alabiso A. Coro- microvascular reactivity in trained adolescents. Eur J Appl Physiol 108:
nary arteries in physiological hypertrophy: Echocardiographic evidence 1201-1208, 2010.
of increased proximal size in elite athletes. Int J Sports Med 11: 120- 361. Roeske WR, O’Rourke RA, Klein A, Leopold G, Karliner JS. Non-
126, 1990. invasive evaluation of ventricular hypertrophy in professional athletes.
335. Pipp F, Boehm S, Cai WJ, Adili F, Ziegler B, Karanovic G, Ritter Circulation 53: 286-291, 1976.
R, Balzer J, Scheler C, Schaper W, Schmitz-Rixen T. Elevated fluid 362. Rongen GA, Smits P, Thien T. Characterization of ATP-induced vasodi-
shear stress enhances postocclusive collateral artery growth and gene lation in the human forearm vascular bed. Circulation 90: 1891-1898,
expression in the pig hind limb. Arterioscler Thromb Vasc Biol 24: 1994.
1664-1668, 2004. 363. Rosenmeier JB, Fritzlar SJ, Dinenno FA, Joyner MJ. Exogenous NO
336. Powers SK, Ji LL, Leeuwenburgh C. Exercise training-induced alter- administration and alpha-adrenergic vasoconstriction in human limbs.
ations in skeletal muscle antioxidant capacity: A brief review. Med Sci J Appl Physiol 95: 2370-2374, 2003.
Sports Exerc 31: 987-997, 1999. 364. Rosenmeier JB, Hansen J, Gonzalez-Alonso J. Circulating ATP-
337. Prasad A, Popovic ZB, Arbab-Zadeh A, Fu Q, Palmer D, Dijk E, induced vasodilatation overrides sympathetic vasoconstrictor activity
Greenberg NL, Garcia MJ, Thomas JD, Levine BD. The effects of in human skeletal muscle. J Physiol 558: 351-365, 2004.
aging and physical activity on Doppler measures of diastolic function. 365. Rosenmeier JB, Yegutkin GG, Gonzalez-Alonso J. Activation of
Am J Cardiol 99: 1629-1636, 2007. ATP/UTP-selective receptors increases blood flow and blunts sym-
338. Pressler A, Haller B, Scherr J, Heitkamp D, Esefeld K, Boscheri A, pathetic vasoconstriction in human skeletal muscle. J Physiol 586:
Wolfarth B, Halle M. Association of body composition and left ven- 4993-5002, 2008.
tricular dimensions in elite athletes. Eur J Prev Cardiol 19: 1194-1204, 366. Rosenwinkel ET, Bloomfield DM, Arwady MA, Goldsmith RL. Exer-
2012. cise and autonomic function in health and cardiovascular disease. Car-
339. Proctor DN, Miller JD, Dietz NM, Minson CT, Joyner MJ. Reduced diol Clin 19: 369-387, 2001.
submaximal leg blood flow after high-intensity aerobic training. J Appl 367. Roskamm H, Reindell H, Musshoff K, Koenig K. [Relations between
Physiol (1985) 91: 2619-2627, 2001. heart size and physical efficiency in male and female athletes in compar-
340. Proctor DN, Sinning WE, Walro JM, Sieck GC, Lemon PW. Oxidative ison with normal male and female subjects. III]. Arch Kreislaufforsch
capacity of human muscle fiber types: Effects of age and training status 35: 67-102, 1961.
4. J Appl Physiol 78: 2033-2038, 1995. 368. Rowell LB. Human Cardiovascular Control. Oxford University Press,
341. Pugh LG. Blood volume changes in outdoor exercise of 8-10 hour New York, 1993.
duration. J Physiol 200: 345-351, 1969. 369. Rowell LB, Blackmon JR, Bruce RA. Indocyanine green clearance and
342. Pynn M, Schafer K, Konstantinides S, Halle M. Exercise training estimated hepatic blood flow during mild to maximal exercise in upright
reduces neointimal growth and stabilizes vascular lesions developing man. J Clin Invest 43: 1677-1690, 1964.
after injury in apolipoprotein e-deficient mice. Circulation 109: 386- 370. Rowell LB, Saltin B, Kiens B, Christensen NJ. Is peak quadriceps
392, 2004. blood flow in humans even higher during exercise with hypoxemia?
343. Radegran G, Calbet JA. Role of adenosine in exercise-induced human Am J Physiol 251: H1038-H1044, 1986.
skeletal muscle vasodilatation. Acta Physiol Scand 171: 177-185, 2001. 371. Rowley NJ, Dawson EA, Birk GK, Cable NT, George K, Whyte G,
344. Radegran G, Saltin B. Nitric oxide in the regulation of vasomotor tone Thijssen DH, Green DJ. Exercise and arterial adaptation in humans:
in human skeletal muscle. Am J Physiol 276: H1951-H1960, 1999. Uncoupling localized and systemic effects. J Appl Physiol (1985) 110:
345. Radegran G, Saltin B. Human femoral artery diameter in relation to 1190-1195, 2011.
knee extensor muscle mass, peak blood flow, and oxygen uptake. Am J 372. Rowley NJ, Dawson EA, Hopman MT, George KP, Whyte GP, Thijssen
Physiol Heart Circ Physiol 278: H162-H167, 2000. DH, Green DJ. Conduit diameter and wall remodeling in elite athletes
346. Ray CA. Sympathetic adaptations to one-legged training. J Appl Physiol and spinal cord injury. Med Sci Sports Exerc 44: 844-849, 2012.
(1985) 86: 1583-1587, 1999. 373. Rowley NJ, Green DJ, George K, Thijssen DH, Oxborough D, Sharma
347. Ray CA, Mark AL. Sympathetic nerve activity to nonactive muscle S, Somauroo JD, Jones J, Sheikh N, Whyte G. Peripheral vascular
of the exercising and nonexercising limb. Med Sci Sports Exerc 27: structure and function in hypertrophic cardiomyopathy. Br J Sports
183-187, 1995. Med 46 Suppl 1: i98-103, 2012.
348. Ray CJ, Abbas MR, Coney AM, Marshall JM. Interactions of adenosine, 374. Rubanyi GM, Romero JC, Vanhoutte PM. Flow-induced release of
prostaglandins and nitric oxide in hypoxia-induced vasodilatation: In endothelium-derived relaxing factor. Am J Physiol 250: H1145-H1149,
vivo and in vitro studies. J Physiol 544: 195-209, 2002. 1986.
30 Volume 6, January 2016
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Comprehensive Physiology Cardiovascular Effects of Endurance Training
375. Rullman E, Rundqvist H, Wagsater D, Fischer H, Eriksson P, Sundberg 402. Sinoway LI, Musch TI, Minotti JR, Zelis R. Enhanced maximal
CJ, Jansson E, Gustafsson T. A single bout of exercise activates matrix metabolic vasodilatation in the dominant forearms of tennis players.
metalloproteinase in human skeletal muscle. J Appl Physiol 102: 2346- J Appl Physiol (1985) 61: 673-678, 1986.
2351, 2007. 403. Sinoway LI, Shenberger J, Wilson J, McLaughlin D, Musch T, Zelis
376. Rush JW, Aultman CD. Vascular biology of angiotensin and the impact R. A 30-day forearm work protocol increases maximal forearm blood
of physical activity. Appl Physiol Nutr Metab 33: 162-172, 2008. flow. J Appl Physiol (1985) 62: 1063-1067, 1987.
377. Saltin B. Capacity of blood flow delivery to exercising skeletal muscle 404. Sivertsson R. The hemodynamic importance of structural vascular
in humans. Am J Cardiol 62: 30E-35E, 1988. changes in essential hypertension. Acta Physiol Scand Suppl 343: 1-56,
378. Saltin B, Blomqvist G, Mitchell JH, Johnson RL, Jr., Wildenthal K, 1970.
Chapman CB. Response to exercise after bed rest and after training. 405. Smith ML, Hudson DL, Graitzer HM, Raven PB. Exercise training
Circulation 38: VII1-78, 1968. bradycardia: The role of autonomic balance. Med Sci Sports Exerc 21:
379. Saltin B, Mortensen SP. Inefficient functional sympatholysis is an over- 40-44, 1989.
looked cause of malperfusion in contracting skeletal muscle. J Physiol 406. Smits P, Williams SB, Lipson DE, Banitt P, Rongen GA, Creager MA.
590: 6269-6275, 2012. Endothelial release of nitric oxide contributes to the vasodilator effect
380. Saltin B, Nazar K, Costill DL, Stein E, Jansson E, Essen B, Gollnick D. of adenosine in humans. Circulation 92: 2135-2141, 1995.
The nature of the training response; peripheral and central adaptations 407. Snell PG, Martin WH, Buckey JC, Blomqvist CG. Maximal vascular
of one-legged exercise. Acta Physiol Scand 96: 289-305, 1976. leg conductance in trained and untrained men. J Appl Physiol (1985)
381. Saltin B, Rowell LB. Functional adaptations to physical activity and 62: 606-610, 1987.
inactivity. Fed Proc 39: 1506-1513, 1980. 408. Song W, Kwak HB, Kim JH, Lawler JM. Exercise training modu-
382. Sander M, Chavoshan B, Harris SA, Iannaccone ST, Stull JT, Thomas lates the nitric oxide synthase profile in skeletal muscle from old rats.
GD, Victor RG. Functional muscle ischemia in neuronal nitric oxide J Gerontol A Biol Sci Med Sci 64: 540-549, 2009.
synthase-deficient skeletal muscle of children with Duchenne muscular 409. Spence AL, Carter HH, Naylor LH, Green DJ. A prospective random-
dystrophy. Proc Natl Acad Sci U S A 97: 13818-13823, 2000. ized longitudinal study involving 6 months of endurance or resistance
383. Sandoval YH, Atef ME, Levesque LO, Li Y, Anand-Srivastava MB. exercise. Conduit artery adaptation in humans. J Physiol 591: 1265-
Endothelin-1 signaling in vascular physiology and pathophysiology. 1275, 2013.
Curr Vasc Pharmacol 12: 202-214, 2014. 410. Spirito P, Pelliccia A, Proschan MA, Granata M, Spataro A, Bellone P,
384. Sarelius I, Pohl U. Control of muscle blood flow during exercise: Local Caselli G, Biffi A, Vecchio C, Maron BJ. Morphology of the “athlete’s
factors and integrative mechanisms. Acta Physiol (Oxf) 199: 349-365, heart” assessed by echocardiography in 947 elite athletes representing
2010. 27 sports. Am J Cardiol 74: 802-806, 1994.
385. Sawka MN, Convertino VA, Eichner ER, Schnieder SM, Young AJ. 411. Sprague RS, Bowles EA, Achilleus D, Ellsworth ML. Erythrocytes as
Blood volume: importance and adaptations to exercise training, envi- controllers of perfusion distribution in the microvasculature of skeletal
ronmental stresses, and trauma/sickness. Med Sci Sports Exerc 32: muscle. Acta Physiol (Oxf) 202: 285-292, 2011.
332-348, 2000. 412. Sprague RS, Ellsworth ML. Erythrocyte-derived ATP and perfusion dis-
386. Sayed A, Schierling W, Troidl K, Ruding I, Nelson K, Apfelbeck H, tribution: Role of intracellular and intercellular communication. Micro-
Benli I, Schaper W, Schmitz-Rixen T. Exercise linked to transient circulation 19: 430-439, 2012.
increase in expression and activity of cation channels in newly formed 413. Stergioulas AT, Filippou DK. Effects of physical conditioning on lipids
hind-limb collaterals. Eur J Vasc Endovasc Surg 40: 81-87, 2010. and arachidonic acid metabolites in untrained boys: A longitudinal
387. Scharf M, Brem MH, Wilhelm M, Schoepf UJ, Uder M, Lell MM. study. Appl Physiol Nutr Metab 31: 432-441, 2006.
Cardiac magnetic resonance assessment of left and right ventricular 414. Strange S. Cardiovascular control during concomitant dynamic leg exer-
morphologic and functional adaptations in professional soccer players. cise and static arm exercise in humans. J Physiol 514(Pt 1): 283-291,
Am Heart J 159: 911-918, 2010. 1999.
388. Scharhag J, Schneider G, Urhausen A, Rochette V, Kramann B, Kinder- 415. Stratton JR, Levy WC, Cerqueira MD, Schwartz RS, Abrass IB. Car-
mann W. Athlete’s heart: Right and left ventricular mass and function diovascular responses to exercise. Effects of aging and exercise training
in male endurance athletes and untrained individuals determined by in healthy men. Circulation 89: 1648-1655, 1994.
magnetic resonance imaging. J Am Coll Cardiol 40: 1856-1863, 2002. 416. Sun D, Huang A, Koller A, Kaley G. Adaptation of flow-induced dila-
389. Schmidt-Trucksass A, Schmid A, Dorr B, Huonker M. The relationship tion of arterioles to daily exercise. Microvasc Res 56: 54-61, 1998.
of left ventricular to femoral artery structure in male athletes. Med Sci 417. Taddei S, Galetta F, Virdis A, Ghiadoni L, Salvetti G, Franzoni F, Giusti
Sports Exerc 35: 214-219, 2003. C, Salvetti A. Physical activity prevents age-related impairment in nitric
390. Schrage WG, Joyner MJ, Dinenno FA. Local inhibition of nitric oxide oxide availability in elderly athletes. Circulation 101: 2896-2901, 2000.
and prostaglandins independently reduces forearm exercise hyperaemia 418. Taddei S, Virdis A, Ghiadoni L, Salvetti G, Bernini G, Magagna A,
in humans. J Physiol 557: 599-611, 2004. Salvetti A. Age-related reduction of NO availability and oxidative stress
391. Schrage WG, Wilkins BW, Dean VL, Scott JP, Henry NK, Wylam in humans. Hypertension 38: 274-279, 2001.
ME, Joyner MJ. Exercise hyperemia and vasoconstrictor responses in 419. Taddei S, Virdis A, Mattei P, Ghiadoni L, Fasolo CB, Sudano I, Salvetti
humans with cystic fibrosis. J Appl Physiol (1985) 99: 1866-1871, 2005. A. Hypertension causes premature aging of endothelial function in
392. Scribbans TD, Edgett BA, Vorobej K, Mitchell AS, Joanisse SD, Matu- humans. Hypertension 29: 736-743, 1997.
siak JB, Parise G, Quadrilatero J, Gurd BJ. Fibre-specific responses 420. Takeno Y, Kamijo YI, Nose H. Thermoregulatory and aerobic changes
to endurance and low volume high intensity interval training: Striking after endurance training in a hypobaric hypoxic and warm environment.
similarities in acute and chronic adaptation. PLoS One 9: e98119, 2014. J Appl Physiol (1985) 91: 1520-1528, 2001.
393. Seals DR. Sympathetic neural adjustments to stress in physically trained 421. Takeshita A, Mark AL. Decreased vasodilator capacity of forearm resis-
and untrained humans. Hypertension 17: 36-43, 1991. tance vessels in borderline hypertension. Hypertension 2: 610-616,
394. Seals DR, Victor RG. Regulation of muscle sympathetic nerve activity 1980.
during exercise in humans. Exerc Sport Sci Rev 19: 313-349, 1991. 422. Tanaka H, Dinenno FA, Monahan KD, Desouza CA, Seals DR. Carotid
395. Secher NH, Clausen JP, Klausen K, Noer I, Trap-Jensen J. Central and artery wall hypertrophy with age is related to local systolic blood pres-
regional circulatory effects of adding arm exercise to leg exercise. Acta sure in healthy men. Arterioscler Thromb Vasc Biol 21: 82-87, 2001.
Physiol Scand 100: 288-297, 1977. 423. Tang K, Breen EC, Gerber HP, Ferrara NM, Wagner PD. Capillary
396. Segal SS, Duling BR. Conduction of vasomotor responses in arterioles: regression in vascular endothelial growth factor-deficient skeletal mus-
A role for cell-to-cell coupling? Am J Physiol 256: H838-H845, 1989. cle. Physiol Genomics 18: 63-69, 2004.
397. Sexton WL, Korthuis RJ, Laughlin MH. High-intensity exercise train- 424. Tesch PA. Skeletal muscle adaptations consequent to long-term heavy
ing increases vascular transport capacity of rat hindquarters. Am J Phys- resistance exercise. Med Sci Sports Exerc 20: S132-S134, 1988.
iol 254: H274-H278, 1988. 425. Tesch PA, Thorsson A, Colliander EB. Effects of eccentric and concen-
398. Shoemaker JK, Halliwill JR, Hughson RL, Joyner MJ. Contributions of tric resistance training on skeletal muscle substrates, enzyme activities
acetylcholine and nitric oxide to forearm blood flow at exercise onset and capillary supply. Acta Physiol Scand 140: 575-580, 1990.
and recovery. Am J Physiol 273: H2388-H2395, 1997. 426. Thijssen DH, Black MA, Pyke KE, Padilla J, Atkinson G, Harris RA,
399. Sindler AL, Delp MD, Reyes R, Wu G, Muller-Delp JM. Effects of Parker B, Widlansky ME, Tschakovsky ME, Green DJ. Assessment of
ageing and exercise training on eNOS uncoupling in skeletal muscle flow-mediated dilation in humans: A methodological and physiological
resistance arterioles. J Physiol 587: 3885-3897, 2009. guideline. Am J Physiol Heart Circ Physiol 300: H2-12, 2011.
400. Sindler AL, Reyes R, Chen B, Ghosh P, Gurovich AN, Kang LS, 427. Thijssen DH, Dawson EA, van den Munckhof IC, Birk GK, Timothy
Cardounel AJ, Delp MD, Muller-Delp JM. Age and exercise training CN, Green DJ. Local and systemic effects of leg cycling training on
alter signaling through reactive oxygen species in the endothelium of arterial wall thickness in healthy humans. Atherosclerosis 229: 282-286,
skeletal muscle arterioles. J Appl Physiol (1985) 114: 681-693, 2013. 2013.
401. Singel DJ, Stamler JS. Chemical physiology of blood flow regulation 428. Thijssen DH, Rongen GA, van DA, Smits P, Hopman MT. Enhanced
by red blood cells: the role of nitric oxide and S-nitrosohemoglobin. endothelin-1-mediated leg vascular tone in healthy older subjects.
Annu Rev Physiol 67: 99-145, 2005. J Appl Physiol (1985) 103: 852-857, 2007.
Volume 6, January 2016 31
JWBT335-c140080 JWBT335-CompPhys-3G-v1 Printer: Yet to Come November 9, 2015 13:21 8in×10.75in
Cardiovascular Effects of Endurance Training Comprehensive Physiology
429. Thodeti CK, Matthews B, Ravi A, Mammoto A, Ghosh K, Bracha AL, 449. Wang E, Solli GS, Nyberg SK, Hoff J, Helgerud J. Stroke volume does
Ingber DE. TRPV4 channels mediate cyclic strain-induced endothelial not plateau in female endurance athletes. Int J Sports Med 33: 734-739,
cell reorientation through integrin-to-integrin signaling. Circ Res 104: 2012.
1123-1130, 2009. 450. Wang JS. Effects of exercise training and detraining on cutaneous
430. Thomas GD, Sander M, Lau KS, Huang PL, Stull JT, Victor RG. microvascular function in man: the regulatory role of endothelium-
Impaired metabolic modulation of alpha-adrenergic vasoconstriction dependent dilation in skin vasculature. Eur J Appl Physiol 93: 429-434,
in dystrophin-deficient skeletal muscle. Proc Natl Acad Sci U S A 95: 2005.
15090-15095, 1998. 451. Weibel ER, Taylor CR, Hoppeler H. The concept of symmorphosis: A
431. Thomas GD, Victor RG. Nitric oxide mediates contraction-induced testable hypothesis of structure-function relationship 1. Proc Natl Acad
attenuation of sympathetic vasoconstriction in rat skeletal muscle. Sci U S A 88: 10357-10361, 1991.
J Physiol 506(Pt 3): 817-826, 1998. 452. Wendel-Vos GC, Schuit AJ, Feskens EJ, Boshuizen HC, Verschuren
432. Tinken TM, Thijssen DH, Hopkins N, Black MA, Dawson EA, Minson WM, Saris WH, Kromhout D. Physical activity and stroke. A meta-
CT, Newcomer SC, Laughlin MH, Cable NT, Green DJ. Impact of analysis of observational data. Int J Epidemiol 33: 787-798, 2004.
shear rate modulation on vascular function in humans. Hypertension 453. Wieling W, Borghols EA, Hollander AP, Danner SA, Dunning AJ.
54: 278-285, 2009. Echocardiographic dimensions and maximal oxygen uptake in oarsmen
433. Tinken TM, Thijssen DH, Hopkins N, Dawson EA, Cable NT, Green during training. Br Heart J 46: 190-195, 1981.
DJ. Shear stress mediates endothelial adaptations to exercise training 454. Wilhelm M, Roten L, Tanner H, Wilhelm I, Schmid JP, Saner H. Atrial
in humans. Hypertension 55: 312-318, 2010. remodeling, autonomic tone, and lifetime training hours in nonelite
434. Trappe SW, Costill DL, Fink WJ, Pearson DR. Skeletal muscle char- athletes. Am J Cardiol 108: 580-585, 2011.
acteristics among distance runners: A 20-yr follow-up study. J Appl 455. Williams MH, Wesseldine S, Somma T, Schuster R. The effect of
Physiol (1985) 78: 823-829, 1995. induced erythrocythemia upon 5-mile treadmill run time. Med Sci
435. Tronc F, Wassef M, Esposito B, Henrion D, Glagov S, Tedgui A. Role Sports Exerc 13: 169-175, 1981.
of NO in flow-induced remodeling of the rabbit common carotid artery. 456. Windecker S, Allemann Y, Billinger M, Pohl T, Hutter D, Orsucci T,
Arterioscler Thromb Vasc Biol 16: 1256-1262, 1996. Blaga L, Meier B, Seiler C. Effect of endurance training on coronary
436. Trott DW, Gunduz F, Laughlin MH, Woodman CR. Exercise training artery size and function in healthy men: An invasive followup study.
reverses age-related decrements in endothelium-dependent dilation in Am J Physiol Heart Circ Physiol 282: H2216-H2223, 2002.
skeletal muscle feed arteries. J Appl Physiol (1985) 106: 1925-1934, 457. Winder WW, Hagberg JM, Hickson RC, Ehsani AA, McLane JA. Time
2009. course of sympathoadrenal adaptation to endurance exercise training in
437. Tschakovsky ME, Sujirattanawimol K, Ruble SB, Valic Z, Joyner MJ. man. J Appl Physiol Respir Environ Exerc Physiol 45: 370-374, 1978.
Is sympathetic neural vasoconstriction blunted in the vascular bed of 458. Woodman CR, Muller JM, Rush JW, Laughlin MH, Price EM. Flow
exercising human muscle? J Physiol 541: 623-635, 2002. regulation of ecNOS and Cu/Zn SOD mRNA expression in porcine
438. Tu J, Le G, Ballard HJ. Involvement of the cystic fibrosis transmem- coronary arterioles. Am J Physiol 276: H1058-H1063, 1999.
brane conductance regulator in the acidosis-induced efflux of ATP from 459. Wragg JW, Durant S, McGettrick HM, Sample KM, Egginton S, Bick-
rat skeletal muscle. J Physiol 588: 4563-4578, 2010. nell R. Shear stress regulated gene expression and angiogenesis in
439. Turner DL, Hoppeler H, Noti C, Gurtner HP, Gerber H, Schena F, vascular endothelium. Microcirculation 21: 290-300, 2014.
Kayser B, Ferretti G. Limitations to VO2max in humans after blood 460. Xiang L, Naik J, Hester RL. Exercise-induced increase in skeletal mus-
retransfusion. Respir Physiol 92: 329-341, 1993. cle vasodilatory responses in obese Zucker rats. Am J Physiol Regul
440. Tuttle JL, Nachreiner RD, Bhuller AS, Condict KW, Connors BA, Integr Comp Physiol 288: R987-R991, 2005.
Herring BP, Dalsing MC, Unthank JL. Shear level influences resistance 461. Yamashita H, Sato N, Yamamoto M, Gasa S, Izawa T, Komabayashi T,
artery remodeling: Wall dimensions, cell density, and eNOS expression. Ishikawa M, Sato Y, Ohno H. Effect of endurance training on angio-
Am J Physiol Heart Circ Physiol 281: H1380-H1389, 2001. genic activity in skeletal muscles. Pflugers Arch 422: 332-338, 1993.
441. Tzima E, Irani-Tehrani M, Kiosses WB, Dejana E, Schultz DA, Engel- 462. Yellin EL, Nikolic S, Frater RW. Left ventricular filling dynamics and
hardt B, Cao G, DeLisser H, Schwartz MA. A mechanosensory complex diastolic function. Prog Cardiovasc Dis 32: 247-271, 1990.
that mediates the endothelial cell response to fluid shear stress. Nature 463. Zavorsky GS. Evidence and possible mechanisms of altered maximum
437: 426-431, 2005. heart rate with endurance training and tapering. Sports Med 29: 13-26,
442. Underwood FB, Laughlin MH, Sturek M. Altered control of calcium 2000.
in coronary smooth muscle cells by exercise training. Med Sci Sports 464. Zhao HC, Wang F. Exercise training changes the gating properties of
Exerc 26: 1230-1238, 1994. large-conductance Ca2+-activated K+ channels in rat thoracic aorta
443. Utomi V, Oxborough D, Whyte GP, Somauroo J, Sharma S, Shave R, smooth muscle cells. J Biomech 43: 263-267, 2010.
Atkinson G, George K. Systematic review and meta-analysis of training 465. Zhou A, Egginton S, Hudlicka O, Brown MD. Internal division of
mode, imaging modality and body size influences on the morphology capillaries in rat skeletal muscle in response to chronic vasodilator
and function of the male athlete’s heart. Heart 99: 1727-1733, 2013. treatment with alpha1-antagonist prazosin. Cell Tissue Res 293: 293-
444. Vanhoutte PM. COX-1 and vascular disease. Clin Pharmacol Ther 86: 303, 1998.
212-215, 2009. 466. Zhou AL, Egginton S, Brown MD, Hudlicka O. Capillary growth in
445. Victor RG, Bertocci LA, Pryor SL, Nunnally RL. Sympathetic nerve overloaded, hypertrophic adult rat skeletal muscle: An ultrastructural
discharge is coupled to muscle cell pH during exercise in humans. J Clin study. Anat Rec 252: 49-63, 1998.
Invest 82: 1301-1305, 1988. 467. Zhou B, Conlee RK, Jensen R, Fellingham GW, George JD, Fisher
446. Volianitis S, Secher NH. Arm blood flow and metabolism during arm AG. Stroke volume does not plateau during graded exercise in elite
and combined arm and leg exercise in humans. J Physiol 544: 977-984, male distance runners. Med Sci Sports Exerc 33: 1849-1854, 2001.
2002. 468. Zucker IH, Schultz HD, Patel KP, Wang HJ. Modulation of Angiotensin
447. Vongpatanasin W, Wang Z, Arbique D, Arbique G, Adams-Huet B, II Signaling Following Exercise Training in Heart Failure. Am J Physiol
MITCHELL JH, Victor RG, Thomas GD. Functional sympatholysis is Heart Circ Physiol 308: H781-H791, 2015.
impaired in hypertensive humans. J Physiol 589: 1209-1220, 2011. 469. Zumstein A, Mathieu O, Howald H, Hoppeler H. Morphometric analy-
448. Wagner PD, Olfert IM, Tang K, Breen EC. Muscle-targeted deletion sis of the capillary supply in skeletal muscles of trained and untrained
of VEGF and exercise capacity in mice. Respir Physiol Neurobiol 151: subjects–its limitations in muscle biopsies. Pflugers Arch 397: 277-283,
159-166, 2006. 1983.
32 Volume 6, January 2016
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Dor LombarДокумент27 страницDor LombarLeonardoCampanelliОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Gagal GinjalДокумент21 страницаGagal Ginjalidam zhukrufОценок пока нет
- Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewДокумент13 страницPathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewJose de Jesus Ayala LeyvaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Nature Review CryoglobulinemiaДокумент16 страницNature Review CryoglobulinemiaCristina Adriana PopaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Depressão ScreeningДокумент8 страницDepressão ScreeningLeonardoCampanelliОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Screening Dislipidemia em Crianças e AdolescentesДокумент2 страницыScreening Dislipidemia em Crianças e AdolescentesLeonardoCampanelliОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- CARE Checklist English 2013 PDFДокумент1 страницаCARE Checklist English 2013 PDFNithin NairОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Amiloidose de Cadeias LevesДокумент19 страницAmiloidose de Cadeias LevesLeonardoCampanelliОценок пока нет
- Laceration Repair: A Practical Approach: Randall T. Forsch, MD, MPH Sahoko H. Little, MD, PHD and Christa Williams, MDДокумент10 страницLaceration Repair: A Practical Approach: Randall T. Forsch, MD, MPH Sahoko H. Little, MD, PHD and Christa Williams, MDLeonardoCampanelliОценок пока нет
- Pca ScreeningДокумент6 страницPca ScreeningNariska CooperОценок пока нет
- Screening Cancer 2019Документ4 страницыScreening Cancer 2019LeonardoCampanelliОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Screening Cancer GinecológicoДокумент18 страницScreening Cancer GinecológicoLeonardoCampanelliОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Dac ScreeningДокумент2 страницыDac ScreeningLeonardoCampanelliОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Acute Coronary Syndrome PDFДокумент8 страницAcute Coronary Syndrome PDFVedranaJovanovicОценок пока нет
- Nrcardio 2014 26 PDFДокумент14 страницNrcardio 2014 26 PDFLeonardoCampanelliОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The OMI Manifesto PDF 3.29.18Документ39 страницThe OMI Manifesto PDF 3.29.18LeonardoCampanelliОценок пока нет
- Primer: AtherosclerosisДокумент18 страницPrimer: AtherosclerosisLeonardoCampanelliОценок пока нет
- Bloqueadores Do Sraa Não Devem Ser A Primeira EscolhaДокумент3 страницыBloqueadores Do Sraa Não Devem Ser A Primeira EscolhaLeonardoCampanelliОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Nrcardio 2014 26 PDFДокумент14 страницNrcardio 2014 26 PDFLeonardoCampanelliОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Mechanisms of Acute Coronary Syndromes NEJMДокумент10 страницMechanisms of Acute Coronary Syndromes NEJMJavieraAlondraDiazОценок пока нет
- adenoCA Gástrico PDFДокумент19 страницadenoCA Gástrico PDFLeonardoCampanelliОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- 10 1016@j Amjcard 2012 08 001Документ2 страницы10 1016@j Amjcard 2012 08 001LeonardoCampanelliОценок пока нет
- 10 1097@mol 0000000000000330Документ11 страниц10 1097@mol 0000000000000330LeonardoCampanelliОценок пока нет
- Use of "Bioglue" in Aortic Surgical RepairДокумент3 страницыUse of "Bioglue" in Aortic Surgical RepairLeonardoCampanelliОценок пока нет
- Fraturas de Estresse Tornozelo e Pé PDFДокумент23 страницыFraturas de Estresse Tornozelo e Pé PDFLeonardoCampanelliОценок пока нет
- Anemia Approach To The PatientДокумент8 страницAnemia Approach To The PatientLeonardoCampanelliОценок пока нет
- 2019 Nature Endo Exercício e Conversa Músculo CérebroДокумент10 страниц2019 Nature Endo Exercício e Conversa Músculo CérebroLeonardoCampanelliОценок пока нет
- 2019 Nature Endo Tecido Adiposo Risco CardiovascularДокумент18 страниц2019 Nature Endo Tecido Adiposo Risco CardiovascularLeonardoCampanelliОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Lesões de TornozeloДокумент43 страницыLesões de TornozeloLeonardoCampanelliОценок пока нет
- MFC Texto 1Документ12 страницMFC Texto 1Gaetano Di GiovanniОценок пока нет
- Annotated Bibliography 2Документ3 страницыAnnotated Bibliography 2api-458997989Оценок пока нет
- Standalone Financial Results, Limited Review Report For December 31, 2016 (Result)Документ4 страницыStandalone Financial Results, Limited Review Report For December 31, 2016 (Result)Shyam SunderОценок пока нет
- New KitДокумент195 страницNew KitRamu BhandariОценок пока нет
- TM9-1904 - Ammunition Inspection Guide - 1944 PDFДокумент414 страницTM9-1904 - Ammunition Inspection Guide - 1944 PDFhodhodhodsribdОценок пока нет
- Skills Check Extra 2AДокумент1 страницаSkills Check Extra 2AVishmi JayawardeneОценок пока нет
- Robert Egby - DecreesДокумент9 страницRobert Egby - DecreesmuzickaueОценок пока нет
- Flange CheckДокумент6 страницFlange CheckMohd. Fadhil JamirinОценок пока нет
- The Abcs of Edi: A Comprehensive Guide For 3Pl Warehouses: White PaperДокумент12 страницThe Abcs of Edi: A Comprehensive Guide For 3Pl Warehouses: White PaperIgor SangulinОценок пока нет
- Study of Subsonic Wind Tunnel and Its Calibration: Pratik V. DedhiaДокумент8 страницStudy of Subsonic Wind Tunnel and Its Calibration: Pratik V. DedhiaPratikDedhia99Оценок пока нет
- SchedulingДокумент47 страницSchedulingKonark PatelОценок пока нет
- The Evolution of Knowledge Management Systems Needs To Be ManagedДокумент14 страницThe Evolution of Knowledge Management Systems Needs To Be ManagedhenaediОценок пока нет
- Duties and Responsibilities - Filipino DepartmentДокумент2 страницыDuties and Responsibilities - Filipino DepartmentEder Aguirre Capangpangan100% (2)
- Marketing Plan Nokia - Advanced MarketingДокумент8 страницMarketing Plan Nokia - Advanced MarketingAnoop KeshariОценок пока нет
- Pharmacy System Project PlanДокумент8 страницPharmacy System Project PlankkumarОценок пока нет
- As I Lay Writing How To Write Law Review ArticleДокумент23 страницыAs I Lay Writing How To Write Law Review ArticleWalter Perez NiñoОценок пока нет
- Market Structure and TrendДокумент10 страницMarket Structure and TrendbillОценок пока нет
- Mystakidis2022 MetaverseДокумент13 страницMystakidis2022 MetaverseVennela NandikondaОценок пока нет
- Chapter 3-CP For Armed Conflict SituationДокумент23 страницыChapter 3-CP For Armed Conflict Situationisidro.ganadenОценок пока нет
- Pepsi Mix Max Mox ExperimentДокумент2 страницыPepsi Mix Max Mox Experimentanon_192325873Оценок пока нет
- Turbine Flowmeters-Commonly Asked Questions and Answers: For Chemical Composition Information.)Документ8 страницTurbine Flowmeters-Commonly Asked Questions and Answers: For Chemical Composition Information.)Alexander KlmОценок пока нет
- Đề Anh DHBB K10 (15-16) CBNДокумент17 страницĐề Anh DHBB K10 (15-16) CBNThân Hoàng Minh0% (1)
- Jail Versus Substance Abuse TreatmentДокумент5 страницJail Versus Substance Abuse Treatmentapi-240257564Оценок пока нет
- Matrix CPP CombineДокумент14 страницMatrix CPP CombineAbhinav PipalОценок пока нет
- ETSI EG 202 057-4 Speech Processing - Transmission and Quality Aspects (STQ) - Umbrales de CalidaДокумент34 страницыETSI EG 202 057-4 Speech Processing - Transmission and Quality Aspects (STQ) - Umbrales de Calidat3rdacОценок пока нет
- Term Paper A and CДокумент9 страницTerm Paper A and CKishaloy NathОценок пока нет
- 1000 Base - T Magnetics Modules P/N: Gst5009 LF Data Sheet: Bothhand USA Tel: 978-887-8050Документ2 страницы1000 Base - T Magnetics Modules P/N: Gst5009 LF Data Sheet: Bothhand USA Tel: 978-887-8050DennisSendoyaОценок пока нет
- Introduction To Human MovementДокумент5 страницIntroduction To Human MovementNiema Tejano FloroОценок пока нет
- Enzymatic Hydrolysis, Analysis of Mucic Acid Crystals and Osazones, and Thin - Layer Chromatography of Carbohydrates From CassavaДокумент8 страницEnzymatic Hydrolysis, Analysis of Mucic Acid Crystals and Osazones, and Thin - Layer Chromatography of Carbohydrates From CassavaKimberly Mae MesinaОценок пока нет
- Basics of Petroleum GeologyДокумент23 страницыBasics of Petroleum GeologyShahnawaz MustafaОценок пока нет
- 02 Laboratory Exercise 1Документ2 страницы02 Laboratory Exercise 1Mico Bryan BurgosОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)