Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- List of Members Who Can Vote: Panel - Iii Cosmetics, Toiletries, Soaps, Detergents & Essential OilsДокумент14 страницList of Members Who Can Vote: Panel - Iii Cosmetics, Toiletries, Soaps, Detergents & Essential OilsGirish GuptaОценок пока нет
- Revised ECA List From April 2009 To 21st Aug 2019Документ14 страницRevised ECA List From April 2009 To 21st Aug 2019Chaitali DegavkarОценок пока нет
- Pemakaian Obat Harian Pustu Koto Baru Bulan: Dak /dauДокумент56 страницPemakaian Obat Harian Pustu Koto Baru Bulan: Dak /dauDermawan SstОценок пока нет
- 14 Distribution System of Pharmaceuticals Products A Study On Square1Документ23 страницы14 Distribution System of Pharmaceuticals Products A Study On Square1zamilur shuvoОценок пока нет
- Overview of The Availability and Utilization of Kaolin As A Potential Raw Material in Chemicals & Drugs Formulation in NigeriaДокумент6 страницOverview of The Availability and Utilization of Kaolin As A Potential Raw Material in Chemicals & Drugs Formulation in Nigeriawilolud6720100% (1)
- Mercury Drug V BakingДокумент3 страницыMercury Drug V BakingABОценок пока нет
- The Use of Medical Cannabis To Treat Post Traumatic Stress DisorderДокумент15 страницThe Use of Medical Cannabis To Treat Post Traumatic Stress DisorderRay SternОценок пока нет
- Perfecting Your Pharmaceutical Marketing PlanДокумент3 страницыPerfecting Your Pharmaceutical Marketing Plansimply_joshhОценок пока нет
- Isoprenaline Infusion 2016Документ3 страницыIsoprenaline Infusion 2016Glory Claudia KarundengОценок пока нет
- Consumos Medicamentos 2020Документ568 страницConsumos Medicamentos 2020LUCERO LOPEZОценок пока нет
- Answer: C. 3 SuppДокумент22 страницыAnswer: C. 3 SuppDulle MulletОценок пока нет
- Drug of ChoiceДокумент21 страницаDrug of Choiceadharra crystal dorinОценок пока нет
- Bridging The Gap Between R&D and Commercialization in Pharmaceutical Industry: Role of Medical Affairs and Medical CommunicationsДокумент6 страницBridging The Gap Between R&D and Commercialization in Pharmaceutical Industry: Role of Medical Affairs and Medical CommunicationsInternational Journal of Clinical and Biomedical Research (IJCBR)100% (1)
- Indias Leading Pharmaceutical Companies 2016Документ112 страницIndias Leading Pharmaceutical Companies 2016Manan Tyagi100% (1)
- How To Dispose of Meds FlyerДокумент1 страницаHow To Dispose of Meds FlyerJulie MorenoОценок пока нет
- Aime Pocket Card May 2014 3Документ2 страницыAime Pocket Card May 2014 3Miguel XanaduОценок пока нет
- Formulation and Evaluation of Orodispersible Tablets of CelecoxibДокумент8 страницFormulation and Evaluation of Orodispersible Tablets of CelecoxibdadaОценок пока нет
- Notificari Livrari Intracomunitare 28.05.2019 PDFДокумент1 881 страницаNotificari Livrari Intracomunitare 28.05.2019 PDFMaria Luiza ghidrasanОценок пока нет
- Dietary Supplements: What 'S in A Name? What's in The Bottle?Документ3 страницыDietary Supplements: What 'S in A Name? What's in The Bottle?chrissОценок пока нет
- Rustom Shams PDFДокумент48 страницRustom Shams PDFmtaha85Оценок пока нет
- Dosing of Anticancer Agents in Adults PDFДокумент22 страницыDosing of Anticancer Agents in Adults PDFdupuytrenОценок пока нет
- Aromatherapy in Psychiatric DisordersДокумент24 страницыAromatherapy in Psychiatric Disordersxiuhtlaltzin100% (3)
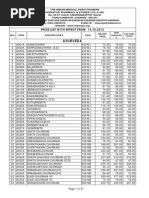
- Price List From 14.10.2013Документ27 страницPrice List From 14.10.2013jasoneinsteinОценок пока нет
- MPharm Course Structure and Syllabus 11-8-2014Документ101 страницаMPharm Course Structure and Syllabus 11-8-2014DongreSanjayОценок пока нет
- Exam Saq Revision QuestionsДокумент5 страницExam Saq Revision QuestionsFarhana Azmira AsmadiОценок пока нет
- Flixotide Nebules PIДокумент9 страницFlixotide Nebules PITatiana BorisenkoОценок пока нет
- Martynia Annuaan OverviewДокумент5 страницMartynia Annuaan OverviewNovy TanoОценок пока нет
- Formulation and Evaluation of Press Coated Tablets of LansoprazoleДокумент8 страницFormulation and Evaluation of Press Coated Tablets of LansoprazoleStevanus HiendrawanОценок пока нет
- GDHHДокумент40 страницGDHHnaelarizqiОценок пока нет
- Bronchodilator From Wikipedia, The Free EncyclopediaДокумент2 страницыBronchodilator From Wikipedia, The Free EncyclopedianandaameliapОценок пока нет